Download to read offline
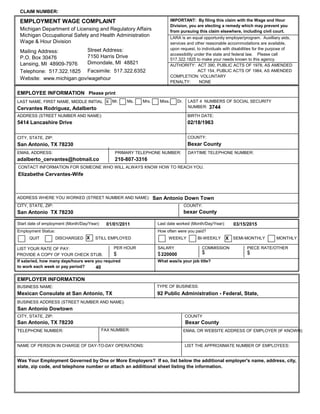



This document is an employment wage complaint filed by Adalberto Cervantes Rodriguez with the Michigan Department of Licensing and Regulatory Affairs against his former employer, the Mexican Consulate in San Antonio, Texas. Mr. Rodriguez claims he is owed $22,000 in unpaid wages for the period of March 15, 2015 to January 1, 2011. He worked as a consular official and claims the unpaid amount is for hourly wages and overtime pay.















































