UTI
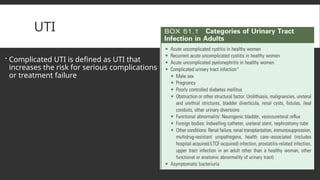
Complicated UTIis defined as UTI that
increases the risk for serious complications
or treatment failure
3.
EPIDEMIOLOGY
The incidenceof cystitis in sexually active young women is about 0.5 per 1 person-
year, recur in 27% to 44% of healthy women, even though they have a normal
urinary tract.3
The incidence of pyelonephritis in young women is about 3 per 1000 person-years.
The selfreported incidence of symptomatic UTI in postmenopausal women is
about 10% per year.
The incidence of symptomatic UTI in adult men younger than 50 years is much
lower than in women, ranging from 5 to 8 per 10,000 men annually
Complicated UTIs occur in a wide range of settings
Asymptomatic bacteriuria is defined as the presence of two separate consecutive
clean-voided urine specimens, both with 105 or more cfu/ml of the same
uropathogen in the absence of symptoms referable to the urinary tract
4.
PATHOGENESIS
Uncomplicated Infetcion
Uropathogens(e.coli) from rectum enter bladder through urethra
From sex partner’s(vag,rectum,penis)
Hematogenous seeding (s.aures)
R/f->behavioral,genetic and biologic factors
Protecting factors are:immune respon, normal vag flora and micturition
Virulence factors -> E.coli p.fimbrae they adherence properties, others like
adherence factors(type 1,S and Dr fimbrae),toxins,immune evasion,flagella
5.
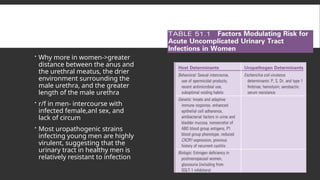
Why morein women->greater
distance between the anus and
the urethral meatus, the drier
environment surrounding the
male urethra, and the greater
length of the male urethra
r/f in men- intercourse with
infected female,anl sex, and
lack of circum
Most uropathogenic strains
infecting young men are highly
virulent, suggesting that the
urinary tract in healthy men is
relatively resistant to infection
6.
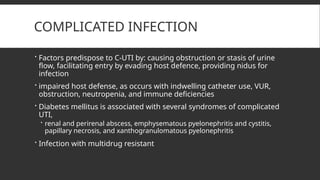
COMPLICATED INFECTION
Factorspredispose to C-UTI by: causing obstruction or stasis of urine
flow, facilitating entry by evading host defence, providing nidus for
infection
impaired host defense, as occurs with indwelling catheter use, VUR,
obstruction, neutropenia, and immune deficiencies
Diabetes mellitus is associated with several syndromes of complicated
UTI,
renal and perirenal abscess, emphysematous pyelonephritis and cystitis,
papillary necrosis, and xanthogranulomatous pyelonephritis
Infection with multidrug resistant
7.
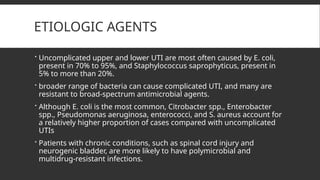
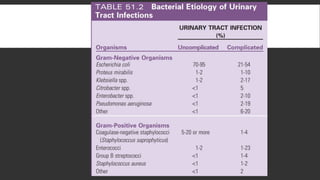
ETIOLOGIC AGENTS
Uncomplicatedupper and lower UTI are most often caused by E. coli,
present in 70% to 95%, and Staphylococcus saprophyticus, present in
5% to more than 20%.
broader range of bacteria can cause complicated UTI, and many are
resistant to broad-spectrum antimicrobial agents.
Although E. coli is the most common, Citrobacter spp., Enterobacter
spp., Pseudomonas aeruginosa, enterococci, and S. aureus account for
a relatively higher proportion of cases compared with uncomplicated
UTIs
Patients with chronic conditions, such as spinal cord injury and
neurogenic bladder, are more likely to have polymicrobial and
multidrug-resistant infections.
9.
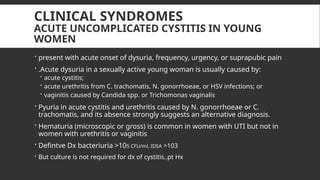
CLINICAL SYNDROMES
ACUTE UNCOMPLICATEDCYSTITIS IN YOUNG
WOMEN
present with acute onset of dysuria, frequency, urgency, or suprapubic pain
.Acute dysuria in a sexually active young woman is usually caused by:
acute cystitis;
acute urethritis from C. trachomatis, N. gonorrhoeae, or HSV infections; or
vaginitis caused by Candida spp. or Trichomonas vaginalis
Pyuria in acute cystitis and urethritis caused by N. gonorrhoeae or C.
trachomatis, and its absence strongly suggests an alternative diagnosis.
Hematuria (microscopic or gross) is common in women with UTI but not in
women with urethritis or vaginitis
Defintve Dx bacteriuria >105 CFU/ml, IDSA >103
But culture is not required for dx of cystitis..pt Hx
10.
E.coli isoften resistant to sulfonamides and amoxicillin in uncomplicated infection, IN
US cotri resistance range 15-42%
Prevalence of E.coli resistance to nitrofurantoin is <5%, although nitrofurantoin is inactive
against Proteus spp. and some Enterobacter and Klebsiella spp
Fluoroquinolones remain active against most E. coli strains causing uncomplicated
cystitis, although resistance is increasing in many areas of the world
Short course regimens are recommended as 1st
line
Nitrofurantooin is well tolerated, has low ecological adverse effects
TMP-SMX despite high resistance, remains effective
Fosfomycin is also 1st
line, b/c of low ecologic adv effect, though it is inferior clinically to
TMP-SMX and flouriqui
both nitrofurantoin and fosfomycin appear to have a role as therapeutic agents
effective against ESBL E. coli UTIs.
11.
The choiceof an antimicrobial agent should be individualized based on:
patient’s allergy and compliance history,
local practice patterns, availability, cost
prevalence of resistance in the local community (if known),
If first line are not good choice- FQs (3-day duration)and beta lactmas
can be used
Cure rate of beta lactams is lower than FQ as 3 day regimen both
Routine post-treatment cultures in women are not indicated unless the
patient is symptomatic
15.
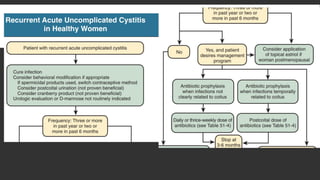
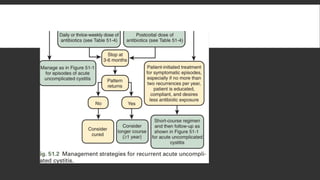
RECURRENT ACUTE UNCOMPLICATEDCYSTITIS
IN WOMEN
Most caused by persistence of the initially infecting strain in the fecal
flora
Expermntal mice study which may occur in human->suggest that some
same-strain recurrent UTIs may be caused by a latent reservoir of
uropathogens in the bladder epithelium that persist after the initial UTI
If the recurrence is within 1 or 2 weeks of treatment, an antimicrobial-
resistant uropathogen should be considered, and a urine culture
should be performed followed by treatment with an alternative
regimen
It is reasonable to treat later recurrences the same as the original
infection, although if the recurrence is within 6 months, one should
consider a first-line drug other than the one used originally, especially if
TMP-SMX was used, because of the likelihood of resistance
16.
Behavioral modificationsavoiding spermicides, increasing fluid intake, and ensuring
postcoital micturition
cranberry products – studie shows no benefit
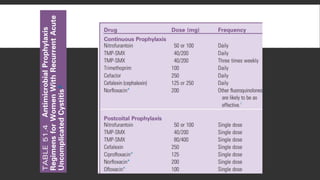
Antimicrobial prophlaxis _reduce recurrence by 95%
for women who experience three or more infections during a 12-month period or
whenever quality of life is being adversely affected by frequent recurrences
Approaches continuous prophlaxis, postcoital prophylaxis, and intermittent self-
treatment
In postmenopausal women with recurrent UTI, intravaginal estradiol is effective,
presumably by normalizing the vaginal flora, which reduces the risk for coliform
colonization of the vagina
Antimicrobial sparing approaches specifically target virulence pathways, which might
prevent uropathogens from causing disease
20.
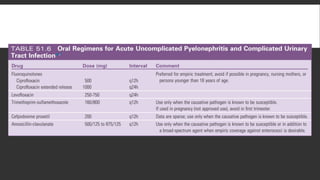
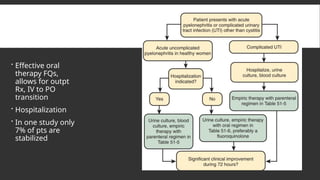
ACUTE UNCOMPLICATED PYELONEPHRITISIN
WOMEN
suggested by fever (temperature 38° C), chills, flank pain, nausea and
≥
vomiting, and costovertebral angle tenderness, Cystitis symptoms are
variably present
Symptoms may vary from a mild illness to a sepsis syndrome with or
without shock and renal failure
Pyuria is almost always present, but leukocyte casts, specific for UTI,
are infrequently seen
Gram stain to differentiate G+ve from G-
A urine culture, which should be performed in all women with acute
pyelonephritis, will have 104 cfu/ml or more of uropathogens in up to
95% of patients
21.
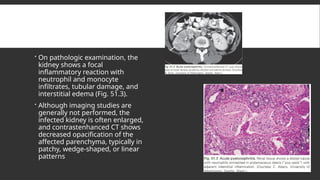
On pathologicexamination, the
kidney shows a focal
inflammatory reaction with
neutrophil and monocyte
infiltrates, tubular damage, and
interstitial edema (Fig. 51.3).
Although imaging studies are
generally not performed, the
infected kidney is often enlarged,
and contrastenhanced CT shows
decreased opacification of the
affected parenchyma, typically in
patchy, wedge-shaped, or linear
patterns
22.
Effective oral
therapyFQs,
allows for outpt
Rx, IV to PO
transition
Hospitalization
In one study only
7% of pts are
stabilized
25.
For outpatients,an oral fluoroquinolone should be used for initial empiric treatment of
infection caused by gram-negative bacilli.
TMP-SMX or other agents can be used if the infecting strain is known to be susceptible.
If enterococci are suspected from the Gram stain, amoxicillin should be added to the
treatment regimen until the causative organism is identified
Second- and third-generation cephalosporins also appear effective, although published
data are sparse.
Nitrofurantoin, fosfomycin, and pivmecillinam are not approved or recommended for the
treatment of pyelonephritis.
or hospitalized patients without evidence of gram-positive infection, ceftriaxone is
effective and inexpensive.
If enterococci are suspected based on the Gram stain, ampicillin plus gentamicin,
ampicillin-sulbactam, and piperacillin-tazobactam are reasonable empiric choices
26.
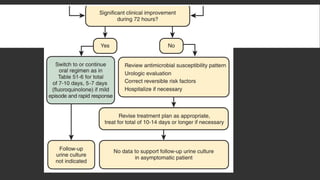
acute uncomplicatedpyelonephritis often can be switched to oral
therapy after 24 to 48 hours,
Treatment of acute uncomplicated pyelonephritis can be limited to 5 to
7 days for patients who have a rapid resolution of fever and symptoms
soon after initiation of treatment.
However, β-lactam regimens shorter than 14 days have been associated
with unacceptably high failure rates in some studies.
27.
COMPLICATED INFECTIONS
Urethritismust be excluded in dysuric sexually active men by a urethral
Gram stain or a first-voided urine specimen wet-mount evaluation for
urethral leukocytosi
Complicated UTI, as with uncomplicated infection, is generally
associated with pyuria and bacteriuria, although these may be absent if
the infection does not communicate with the collecting system
Urine culture should be done
The IDSA consensus definition of complicated UTI is 105 cfu/ml or more in the
urine of women and 104 cfu/ml or more in men,19 but lower counts in
symptomatic persons, as demonstrated in patients with uncomplicated UTI
Correction of any underlying anatomic, functional, or metabolic defect
must be attempted, because antibiotics alone may not be successful
28.
For empirictherapy in patients with mild to moderate illness who can be
treated with oral medication, fluoroquinolones provide the broadest spectrum
of antimicrobial activity, cover most expected pathogens, and achieve high
levels in the urine and urinary tract tissue.
An exception is moxifloxacin, which may not achieve sufficient concentrations in
urine to be effective for complicated UTI.
Nitrofurantoin and fosfomycin should be avoided except for cystitis in pregnancy, in
which duration of treatment is 5 days or single-dose, respectively
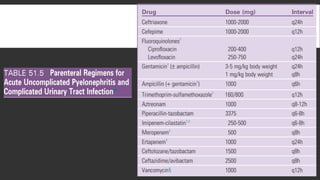
For initial treatment in more seriously ill, hospitalized patients, several
parenteral antimicrobial agents are available (see Table 51.5).
S. aureus is more common in complicated UTIs, and, if suspected, even community
methicillin resistance is vancomycin should be include din the regimen
Duration: a 5- to 10-day regimen is reasonable for most patients with complicated
UTI, depending on their severity of illness and clinical response;
29.
Potential concernsthat must be considered in the management of
complicated UTI include the increasing prevalence of resistance to
fluoroquinolones in institutional settings and the frequency of
enterococcal infections
A recent large retrospective study of male veterans with UTI found no
difference in recurrence rates with 7 days of treatment versus longer, with
a trend toward more Clostridium difficile infections in those treated longer.
At least 10 to 14 days of therapy is recommended in patients who have a
delayed response.
In men, early recurrence of UTI with the same species suggests a prostatic
source of infection and warrants a 4- to 6-week regimen of either a
fluoroquinolone (preferable) or TMP-SMX, depending on the antimicrobial
susceptibility of the infecting strain
30.
CKD
Studies inanimals suggest that:
urine drug concentrations are necessary to sterilize urine,
effective tissue concentrations are necessary to treat pyelonephritis, and
serum concentrations of antimicrobials are correlated with the drug concentrations in renal tissue
some oral agents for cystitis may not deliver adequate concentrations to the urine
As noted previously, however, β-lactams are not as effective as fluoroquinolones, even in
patients with normal renal function.
For oral treatment, renal function adjusted doses of ciprofloxacin or levofloxacin, but not
moxifloxacin, are recommended.
Nitrofurantoin and sulfamethoxazole are not recommended in patients with reduced
creatinine clearance, although trimethoprim concentrations appear to be adequate
Likewise, according to the package insert, renal impairment significantly decreases the
excretion of fosfomycin, which also should not be used in such patients.
31.
CATHETER-ASSOCIATED INFECTIONS.
Theincidence of bacteriuria associated with indwelling catheters is 3%
to 10% per day of catheterization,
the duration of catheterization is the most important risk factor for the
development of catheter-associated bacteriuria.
It is the most common source of gram negative bacteremia in
hospitalized patients
Complications of long-term catheterization ( 30 days) include:
≥
almost universal bacteriuria, often with multiple antibiotic-resistant flora,
frequent febrile episodes, catheter obstruction, stone formation associated
with urease-producing uropathogens, and local genitourinary infections
Other rare complications include fistula formation and bladder cancer.
32.
Most episodesof catheter-associated bacteriuria are asymptomatic and do not require
routine screening or treatment because treatment does not reduce the complications of
bacteriuria and can lead to antimicrobial resistance
the presence or absence of pyuria does not differentiate symptomatic from asymptomatic
urinary infection
In a symptomatic catheterized patient, a urine culture specimen should be obtained from a
freshly placed catheter
clinical outcomes are improved if the catheter is replaced at the time of antimicrobial therapy.
Seven days is the recommended duration of treatment for patients who have prompt
resolution of symptoms, and 10 to 14 days if response is delayed
Prevention: avoid catheter, if is necessary, sterile insertion, prompt removal, and strict
adherence to a closed collecting system, condom cath, antibiotic coated cath
Prophylactic ATB – not recommended
33.
PROSTATITIS
Prostatitis occursin up to 25% of men during their lifetime,
it is caused by acute or chronic bacterial infection in a minority.
The most common organisms causing bacterial prostatitis are gram-
negative bacilli, including E. coli, Proteus spp., Klebsiella spp., P.
aeruginosa, and, less frequently, enterococci and S. aureus.
The pathogenesis related to reflux of infected urine from the urethra
into the prostatic ducts.
Prostatic calculi, commonly found in adult men, may provide a nidus for
bacteria and protection from antibacterial agents.
34.
Acute bacterialprostatitis is rare
Patients present with dysuria, frequency, urgency, obstructive voiding symptoms,
fever, chills, and myalgias
The prostate is tender and swollen
Prostatic massage, as a diagnostic test, is contraindicated because of the risk for
precipitating bacteremia.
The patient will usually have pyuria and a positive urine culture
Patients who are severely ill require hospitalization and parenteral antibiotics, but
many patients can be treated in the outpatient setting with oral fluoroquinolones.
The recommended duration of treatment is 14 to 30 days.57 Rarely, abscess
formation may occur.
35.
Chronic bacterialprostatitis is characterized by recurrent UTIs with the same uropathogen with
intervening asymptomatic periods.
The prostate typically is normal to palpation during asymptomatic periods.
It is characterized microscopically by the presence of 10 or more leukocytes per HPF in expressed
prostatic secretions or postmassage voided urine in the absence of significant pyuria in first-voided
and midstream urine specimens, as well as a uropathogen colony count at least 10-fold higher in the
expressed prostatic secretions or postmassage voided urine compared with the first-voided
midstream urine.
In addition, macrophage-laden fat droplets (oval fat bodies) are usually prominent in the prostatic
secretions.
Cure rates, which historically have been low, are 60% to 80% with the fluoroquinolones, which are the
antibiotics of choice.
The optimal duration of treatment is unknown, but 4 to 6 weeks is recommended by some
authorities, whereas others recommend up to 3 months.
Some patients require long-term, low-dose suppressive therapy to prevent symptomatic UTIs.
Surgical intervention is only rarely considered and is associated with high morbidity
36.
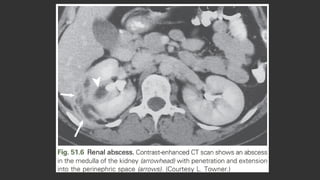
RENAL ABSCESS
Renalcortical and corticomedullary abscesses and perirenal abscesses occur in 1 to 10
per 10,000 hospital admissions
CM: fever, chills, back or abdominal pain, and CVA tenderness, but they may have no
urinary symptoms or findings if the abscess does not communicate with the collecting
system, as in cortical abscess
Bacteremia may be primary (cortical abscess) or secondary (corticomedullary or
perirenal).
The clinical presentation may be insidious and nonspecific, especially with perirenal
abscess, and the diagnosis may not be made until admission to a hospital or at autopsy
CT is recommended to establish the diagnosis and location of a renal or perirenal
abscess
Empiric antibiotic therapy should be broad and cover S. aureus and other uropathogens
causing complicated UTI and modified once urine culture results are known
37.
renal corticalabscess (renal carbuncle)
is usually caused by S. aureus, which reaches the kidney by hematogenous spread.
Treatment antibiotics, and drainage is not required unless the patient is slow to
respond.
renal corticomedullary abscess
usually results from ascending UTI in association with an underlying urinary tract
abnormality, such as obstructive uropathy or VUR
caused by common uropathogenic species such as E. coli
may extend deep into the renal parenchyma, perforate the renal capsule, and form a
perirenal abscess.
Treatment with antimicrobial agents without drainage may be effective if the abscess is
small and if the underlying urinary tract abnormality can be corrected
Aspiration of the abscess may be necessary in some patients, and nephrectomy may
occasionally be required in patients with diffuse renal involvement or with severe sepsis.
38.
Perirenal abscesses
usually occur in the setting of obstruction or other complicating factors (see
Box 51.1)
result from ruptured intrarenal abscesses, hematogenous spread, or spread
from a contiguous infection.
Causative uropathogens are those usually found in complicated UTIs
including S. aureus and enterococci; polymicrobial infections are common.
Anaerobes or Mycobacterium tuberculosis may be causative
A previously high mortality rate has been lowered with earlier diagnosis and
therapy.
In contrast to the other types of renal abscesses, drainage of pus is the
cornerstone of therapy and nephrectomy may be indicated.
40.
PAPILLARY NECROSIS.
Morethan half of patients have diabetes, almost always in conjunction with a UTI,
It can also complicates sickle cell disease, analgesic abuse, and obstruction
Renal papillae are vulnerable to ischemia because of the sluggish blood flow in the vasa recta, and
relatively modest ischemic insults may cause papillary necrosis.
The clinical features are those typical of pyelonephritis. In addition, passage of sloughed papillae
into the ureter may cause renal colic, renal impairment or failure, or obstruction with severe
urosepsis.
Papillary necrosis in the setting of pyelonephritis is associated with pyuria and a positive urine
culture
Causative uropathogens are those typical of complicated UTI
CT is the preferred diagnostic procedure
Radiologic findings include an irregular papillary tip; dilated calyceal fornix; extension of contrast material
into the parenchyma; and a separated crescent-shaped papilla surrounded by contrast, called the ring sign
Broad-spectrum antibiotics are indicated. Papillae obstructing the ureter may require removal with
a cystoscopic ureteral basket or relief of obstruction by insertion of a ureteral stent.
41.
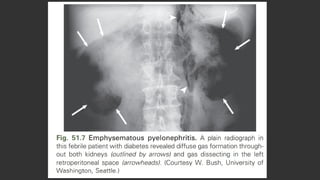
EMPHYSEMATOUS PYELONEPHRITIS.
Itis a fulminant, necrotizing, life-threatening variant of acute pyelonephritis caused by gas-
forming organisms, including E. coli, Klebsiella pneumoniae, P. aeruginosa, and Proteus
mirabilis.
Up to 90% of cases occur in diabetic patients, and obstruction may be present
Symptoms are suggestive of pyelonephritis, and there may be a flank mass.
Pyuria and a positive urine culture with Dehydration and ketoacidosis are common
Gas is usually detected by a plain abdominal radiograph or ultrasound
CT is the diagnostic modality of choice, it can localize the gas better than ultrasound
Parenteral broad-spectrum antibiotics and percutaneous catheter drainage with relief of
obstruction may be adequate for less severely ill patients,
Nephrectomy is warranted for those who are more severely ill and those less severely ill who
do not respond to the preceding steps
Medical treatment is associated with mortality of 60% to 80%, which is lowered to 20% or less
with surgical intervention (e.g., nephrectomy, percutaneous drainage)
43.
RENAL MALACOPLAKIA
Isa chronic granulomatous disorder of unknown etiology involving the GTU, GIT, skin, and pulmonary systems.
It is characterized by an unusual inflammatory reaction to a variety of infections and is manifested by the
accumulation of macrophages containing calcified bacterial debris called Michaelis-Gutmann bodies (Fig. 51.8).
The underlying disorder appears to be a monocyte-macrophage bactericidal defect.
The diagnosis is made by histologic examination of involved tissue.
Genitourinary malacoplakia, most often involving the bladder, is usually associated with gram-negative UTI.
CP: fever, flank pain, pyuria and hematuria, bacteriuria, and, if both kidneys are involved, impaired renal
function
CT usually shows enlarged kidneys with areas of poor enhancement, indistinguishable from other infectious or
neoplastic lesions.
Occasionally may extend through the renal capsule into the perinephric space, simulating a renal carcinoma (see Fig.
51.8).
Rx: broad-spectrum antimicrobial, attempted correction of any underlying complicating conditions, and
improvement of renal function.
Nephrectomy is recommended for advanced unilateral disease. When the disease is bilateral or occurs in a
transplanted kidney, the patient’s prognosis is very poor.
44.
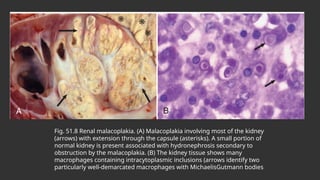
Fig. 51.8 Renalmalacoplakia. (A) Malacoplakia involving most of the kidney
(arrows) with extension through the capsule (asterisks). A small portion of
normal kidney is present associated with hydronephrosis secondary to
obstruction by the malacoplakia. (B) The kidney tissue shows many
macrophages containing intracytoplasmic inclusions (arrows identify two
particularly well-demarcated macrophages with MichaelisGutmann bodies
45.
XANTHOGRANULOMATOUS PYELONEPHRITIS
Isa poorly understood granulomatous inflammation of renal parenchyma associated with
obstruction and infection of the urinary tract
The renal parenchyma is replaced with a diffuse or segmental cellular infiltrate of foam cells,
which are lipid-laden macrophages, which may extend beyond the renal capsule to the
retroperitoneum
Its pathogenesis appears to be multifactorial, with infection complicating obstruction and leading
to ischemia, tissue destruction, and accumulation of lipid deposits.
Typical pts are middle-aged women and have chronic symptoms such as flank pain, fever, chills,
and malaise.
Flank tenderness, a palpable mass, and irritative voiding symptoms are common.
The urine culture is usually positive with E. coli, other gram-negative bacilli, or S. aureus.
CT generally shows an enlarged nonfunctioning kidney, often the presence of calculi and low-
density masses (xanthomatous tissue), maybe difficult to distinguish from neoplastic disease.
Broad-spectrum antimicrobials are indicated, but total or partial nephrectomy is usually
necessary for cure
46.
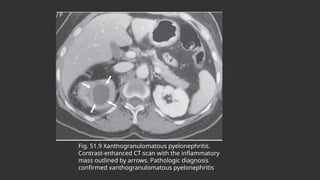
Fig. 51.9 Xanthogranulomatouspyelonephritis.
Contrast-enhanced CT scan with the inflammatory
mass outlined by arrows. Pathologic diagnosis
confirmed xanthogranulomatous pyelonephritis
47.
ASYMPTOMATIC BACTERIURIA
Iscommon and generally benign.
Pyuria is often present, especially in elderly people, and is a predictor for
subsequent symptomatic UTI in some groups.
Screening and treatment is generally not warranted.
In young women with recurrent UTI, asymptomatic bacteriuria may be protective against
symptomatic recurrence and treatment may increase the risk for such recurrences.
patients at high risk for serious complications warrant diagnosis and treatment,
including pregnant women and patients undergoing urologic surgery.
Some authorities advise treatment of asymptomatic bacteriuria found in patients
with anatomic or functional abnormalities of the urinary tract, diabetic patients,
and patients with urea-splitting bacteria (e.g., P. mirabilis, Klebsiella spp.)
Evidence based guidelines for screening and treatment of asymptomatic bacteriuria in
these populations are needed.
48.
IMAGING OF THEURINARY TRACT
Urologic consultation and evaluation of the UT should be considered in patients:
S/S of obstruction, urolithiasis, flank mass, or urosepsis
No clinical response after 72 hours of treatment to exclude complicating factors
renal ultrasound can detect
the size and contour of the kidneys and bladder, the presence of a renal mass or
abscess, certain renal and ureteral calculi, hydronephrosis suggestive of obstructive
uropathy, and elevated postvoid residual urine.
A plain abdominal radiograph (KUB) can identify radiopaque calculi along the
GUT, especially proximal and distal ureteral stones that can be missed on U/S
CT offers fine anatomic detail and is thus the superior study for evaluation of
focal inflammation, renal or perirenal abscess and masses, and both radio-
opaque and radiolucent stones.
49.
Radionuclide imagingprocedures have no role in the evaluation of adults
with UTI, although they are very useful in children with pyelonephritis
Excretory urography and cystoscopy in women with recurrent cystitis
rarely demonstrate abnormalities or alter management3 and therefore
are not recommended.
Likewise, imaging studies in young women with acute pyelonephritis are
also generally not cost-effective and have a low diagnostic yield, although
it is reasonable to obtain such studies after two episodes of
pyelonephritis or if any complicating factor is present
Imaging studies and cystoscopy are probably unnecessary in a man who
has had a single UTI with no obvious complicating factors and whose
infection responds promptly to treatment.
Editor's Notes
#3 Asymptomatic bacteriuria is found in about 5% of young adult women,8 but rarely in men younger than 50. The prevalence increases up to 16% of ambulatory women and 19% of ambulatory men older than 70 and up to 50% of elderly women and 40% of elderly men who are institutionalized.
#7 .15 Among otherwise healthy nonpregnant women, the isolation of lactobacilli, enterococci, group B streptococci, and coagulase-negative staphylococci other than S. saprophyticus most often represents contamination of the urine specimen16 unless found in voided midstream urine in high counts and pure growth in symptomatic women
#10 Pivmecillinam, an extended gram-negative spectrum penicillin used only for treatment of UTI, is an appropriate choice for therapy in regions where it is available (availability limited to some European countries; not licensed and/or available for use in North America), because of minimal resistance and propensity for collateral damage, but efficacy rates are notably lower than with other recommended agents.26 Pivmecillinam also may have a role in the treatment of ESBL-producing uropathogens
#25 TMP-SMX should not be used alone for empiric therapy for pyelonephritis in areas with a high prevalence of resistance to this combination.
#31 (in addition to cystitis, pyelonephritis, and bacteremia, as seen with short-term catheterization
#41 . Accurate localization of gas is important because gas also may form in an infected obstructed collecting system or renal abscess; although serious, these conditions do not carry the same poor prognosis and are managed differently.
#47 Causative uropathogens are the same as those causing UTIs in the same population
Asymptomatic bacteriuria in catheterized patients in hospitals and longterm care facilities, although thought to be generally benign, represents a large reservoir of antimicrobial-resistant urinary pathogens that increases the risk for cross-infection among catheterized patients and results in frequent inappropriate antimicrobial use