SEPSIS-3
The Third InternationalConsensus Definitions for Sepsis and
Septic Shock. JAMA. 2016
Clínica Medica Integral, 403-C, UABC Valle de las Palmas
Rodríguez arenas pedro
2.
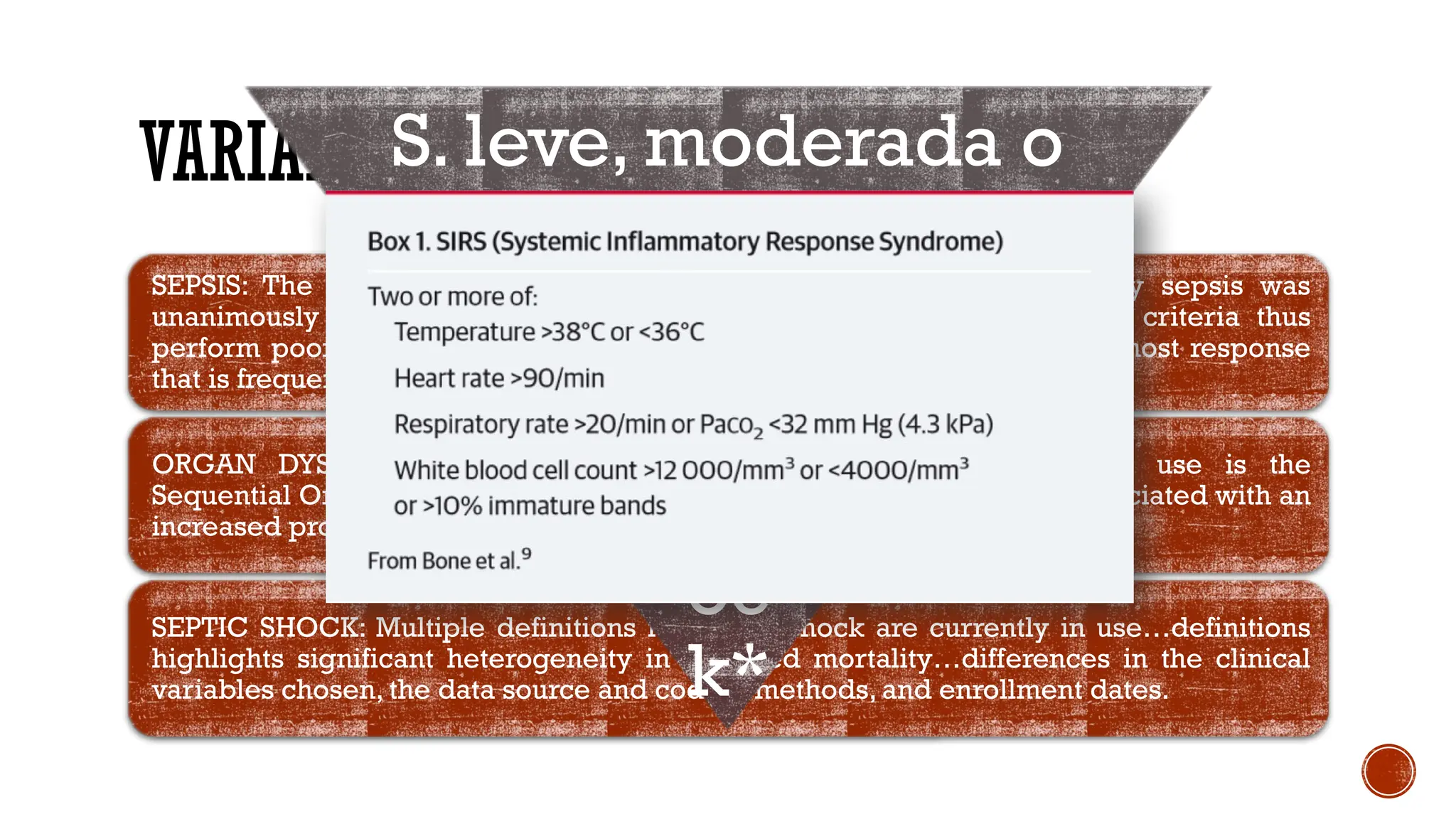
VARIABLE DEFINITIONS
SEPSIS: Thecurrent use of 2 or more SIRS criteria (Box1) to identify sepsis was
unanimously considered by the task force to be unhelpful…the SIRS criteria thus
perform poorly on both counts. SIRS may simply reflect an appropriate host response
that is frequently adaptive.
ORGAN DYSFUNCTION/FAILURE: The predominant score in current use is the
Sequential Organ Failure Assessment (SOFA). A higher SOFA score is associated with an
increased probability of mortality.
SEPTIC SHOCK: Multiple definitions for septic shock are currently in use…definitions
highlights significant heterogeneity in reported mortality…differences in the clinical
variables chosen, the data source and coding methods, and enrollment dates.
S. leve, moderada o
severa
SIRS
Sh
oc
k*
3.
NEW TERMS ANDDEFINTIONS
SEPSIS: life-threatening organ dysfunction caused by a dysregulated host response to infection -when the
body’s response to an infection injures its own tissues and organs-.
ORGAN DYSFUNCTION: Acute change in total SOFA score ≥ 2 points consequent to the infection
(mortality risk of approximately 10%).. Future iterations of the sepsis definitions should include an
updated SOFA score with more optimal variable selection, cutoff values, and weighting,or a superior
scoring system.
qSOFA: Alteration in mental status, systolic blood pressure ≤100mmHg, or respiratory rate ≥ 22/min. The
task forcé suggests that qSOFAcriteria be used to prompt clinicians to further investigate for organ
dysfunction, to initiate or escalate therapy as appropriate, and to consider referral to critical care or
increase the frequency of monitoring.
SEPTIC SHOCK is defined as a subset of sepsis in which underlying circulatory and celular metabolism
abnormalities are profound enough to substantially increase mortality.
Hiperlactatsemia
(>2 mmol/L
[18mg/dL])
Hipotension
(65mm Hg)
![NEW TERMS AND DEFINTIONS
SEPSIS: life-threatening organ dysfunction caused by a dysregulated host response to infection -when the
body’s response to an infection injures its own tissues and organs-.
ORGAN DYSFUNCTION: Acute change in total SOFA score ≥ 2 points consequent to the infection
(mortality risk of approximately 10%).. Future iterations of the sepsis definitions should include an
updated SOFA score with more optimal variable selection, cutoff values, and weighting,or a superior
scoring system.
qSOFA: Alteration in mental status, systolic blood pressure ≤100mmHg, or respiratory rate ≥ 22/min. The
task forcé suggests that qSOFAcriteria be used to prompt clinicians to further investigate for organ
dysfunction, to initiate or escalate therapy as appropriate, and to consider referral to critical care or
increase the frequency of monitoring.
SEPTIC SHOCK is defined as a subset of sepsis in which underlying circulatory and celular metabolism
abnormalities are profound enough to substantially increase mortality.
Hiperlactatsemia
(>2 mmol/L
[18mg/dL])
Hipotension
(65mm Hg)](https://image.slidesharecdn.com/sepsis-3-251009153626-49095d05/75/Survival-Sepsis-3-conceptos-basicos-y-protocolo-3-2048.jpg)





























































