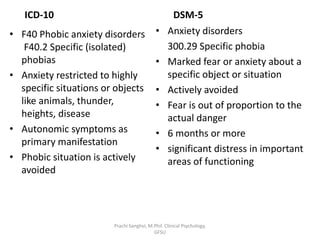
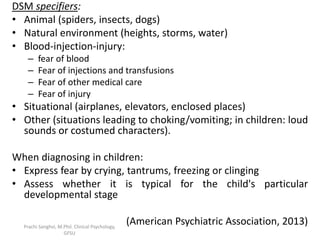
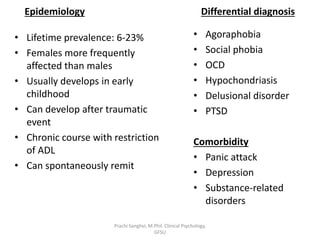
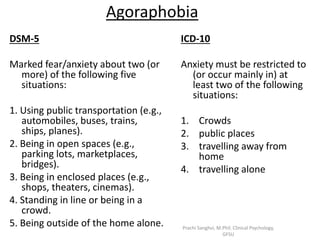
The document provides a comprehensive overview of specific phobia, differentiating it from general anxiety and fear, and detailing its diagnostic criteria according to ICD-10 and DSM-5. It explores the epidemiology, differential diagnosis, comorbidities, assessment techniques, and various aetiological perspectives, including biological, psychoanalytic, behavioral, and cognitive theories. Management strategies for specific phobias are also discussed, highlighting behavioral therapy, cognitive-behavioral therapy, and pharmacotherapy.