A discrete, palpable swelling in an otherwise normal thyroid gland.
Clinically important because it has a higher risk of malignancy compared to multinodular goitre, hence requires evaluation with TFTs, ultrasound, and FNAC
PATIENT.PARTICULARS
Name :ABC Dateof Admission : 10/03/2020
Age : 35years. Date of Examination : 12/03/2020
Sex : Female
Education : Illiterate
Occupation : Farmer
Address :Arsikere taluk, Hassan
Low Socioeconomic status
3.
HISTORY OF PRESENTINGILLNESS
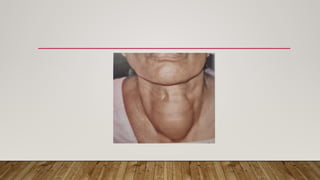
• Patient was apparently alright 8 years back then she noticed a swelling in front of the
lower neck while taking bathe. It was insidious in onset, gradually progressive ; Initially
was about the size of pea (2*2cm) and since 2 months it has progressed to current size
of a Orange (7*7cm) ; Not associated with pain.
• Complaints of noisy breathing since 1 month
• Complaints of Palpitation since 1 month on walking
4.
CONTD..
• Complaints ofeasy fatigability since 1 month
• History of weight gain since 5 months (5 kg)
5.
CONTD..
• No historyof diplopia / change in glasses / blurring of vision
• No history of diarrhoea / constipation
• No history of chest pain / tachycardia / bradycardia
• No history of tremors
• No history of hair loss / pruritus / dupuytren’s contracture
• No history of oligomenorrhea / menorrhagia
• No history of irritability / nervousness / insomnia
• No history of features of Hyperthyroidism or Hypothyroidism
• No history of bone pain
6.
PRESSURE SIGNS
• Nohistory of dysphagia
• No history of ptosis or anhydrosis
7.
PAST HISTORY
• Nohistory of Radiation therapy.
• Not a known case of Diabetes Mellitus / Hypertension / Epilepsy / Asthma
8.
MENSTRUAL HISTORY
• Ageat menarche - 13 years
30 days cycle 5 days flow
2 to 3 pads per day Dysmenorrhea present, no clots
9.
OBSTETRIC HISTORY
• Marriedat 18 years ; Non consanguinous marriage.
• First child - male ; 17 years old
• Second child - female ; 15 years old
10.
FAMILY HISTORY
• Nohistory of thyroid diseases in the family or locality
• No history of Cancers in family (MEN syndrome)
11.
PERSONAL HISTORY
• Diet– non vegetarian diet consumes high brassica containing diet.
• Consumes packaged salt
• Apetite - Normal
• Sleep – Disturbed
• Bowel and bladder – Normal and regular
• Habits - No habits of substance abuse
12.
TREATMENT HISTORY
Medical
• Historyof over the counter antacids and analgesics.
• No History of usage of thyroid related medications.
• No History of contraceptive medications.
Surgical
• No history of any surgeries in the past, other than tubectomy.
13.
SUMMARY
• A 35year old lady presented with OPD with the chief complaints of swelling in the
lower part of the neck since 8 years and gradually increased in size since 1 month with
NO suggestive of features of hypo or hyperthyroidism.
14.
GENERAL PHYSICAL EXAMINATION
•Patient is made to sit in a well lighted room and oral consent was taken for the
examination
• Here is a middle aged lady, who is comfortable at rest,, conscious, cooperative and well
oriented to time place and person.
• Built – Moderate
• Nourishment (BMI)– 20kg/m², No overt signs of Nutritional deficiency.
• Mild pallor present
• No idencece of Icterus, Cyanosis, Clubbing, Lymphadenopathy and Edem
15.
VITALS
• Respiratory rate– 18 cycles per minute, regular rhythm, bilaterally symmetrical,
thoraco- abdominal type.
• Pulse(right radial) – 70 beats per minute, regular rhythm, normal in volume and
character; condition of arterial wall normal, other peripheral pulses were palpable and
bilaterally symmetrical;
Collapsing pulse was absent
• Blood pressure – 130 / 80 mmHg, right arm supine position
• Temperature – 98°F
16.
HEADTOTOE EXAMINATION
• Hair– black, lustrous
• Face – dull, facial flusing
• Eyes – Pallor present
No other eye signs are positive
• Skin - dry skin
• Spine - normal
• Limbs - normal
18.
LOCAL EXAMINATION
Inspection
• Thereis a solitary swelling in the front of the lower neck measuring about 5 cm
horizontally and 7cm vertically extending longitudinally from thyroid cartilage to about
5cm above suprasternal notch and horizontally between anterior border of
sternocleidomastoid muscle on both sides.
• PIZZILLO’s method – the swelling becomes more prominent.
• Surface appears smooth ; nodular swelling.
• Moves up with deglutition.
• Doesn’t move on protrusion of tongue
20.
CONTD..
• Skin overthe swelling is normal
• No scars, sinuses or engorged veins
• Trachea appears to be Central
• PEMBERTON‘s Sign – Negetive
(Neck veins do not become prominent on raising arms)
21.
PALPATION
• All inspectoryfindings are confirmed.
• No tenderness
• No local rise of temperature
• Surface - smooth, firm in consistency, solitary nodule
• Mobility - mobile in horizontal plane ; not vertically.
• Not reducible ; non compressible.
• Able to get below the swelling.
22.
CONTD..
• CRILE‘S METHOD– nodularity felt at pulp of thumb that moves with deglutition
• LAHEY’S METHOD – margins of both Lateral lobes felt
• KOCHER’S SIGN – Negetive
• BERRY’S SIGN – Negative
• Trachea is central
SYSTEMIC EXAMINATION
• Cardiovascularsystem – S1 AND S2 heard, no murmurs.
• Central nervous system – clinically normal
• Respiratory system – normal vesicular breath sounds heard
• Per abdomen – soft, non tender, no organomegaly