Downloaded 635 times
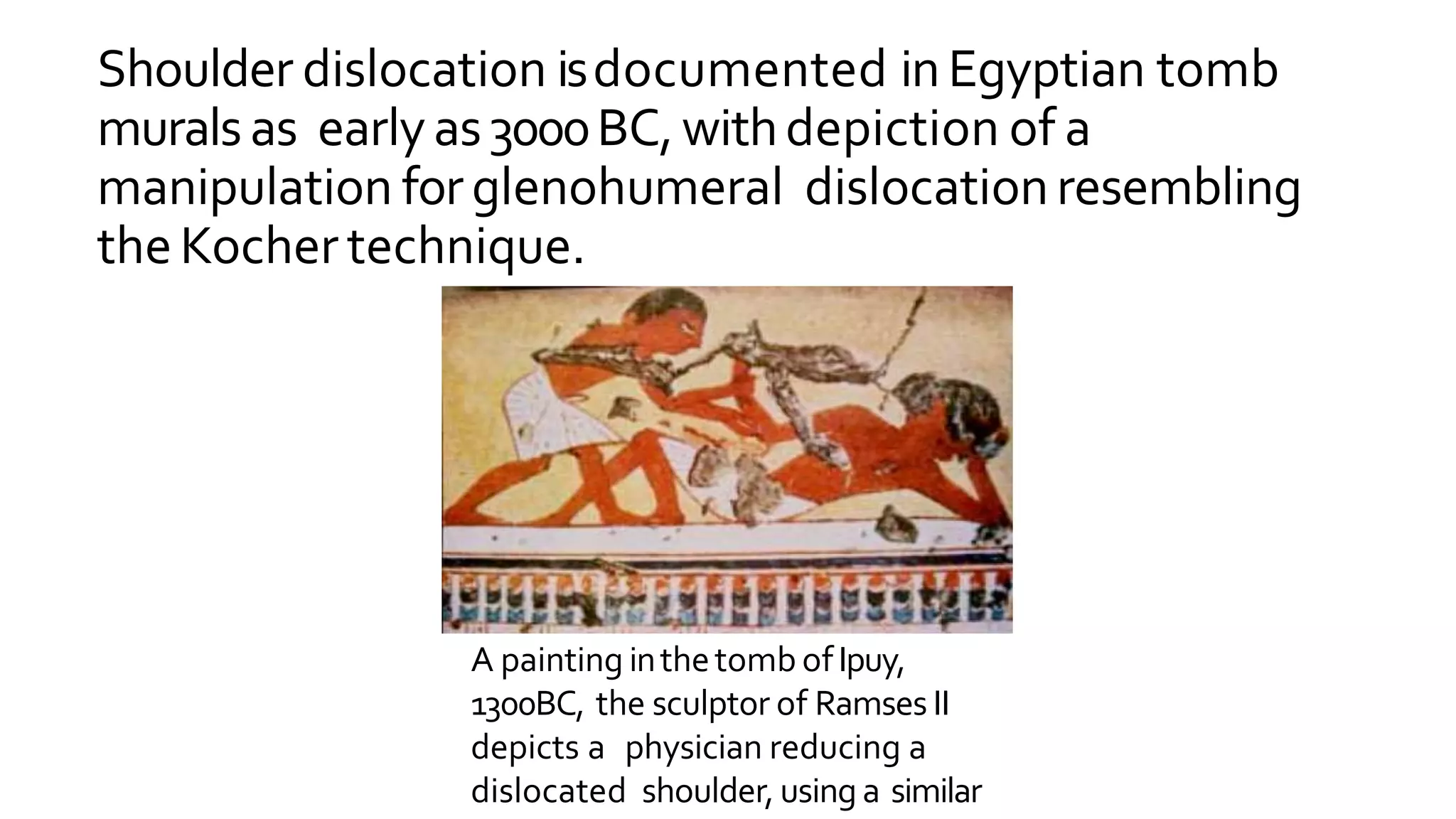
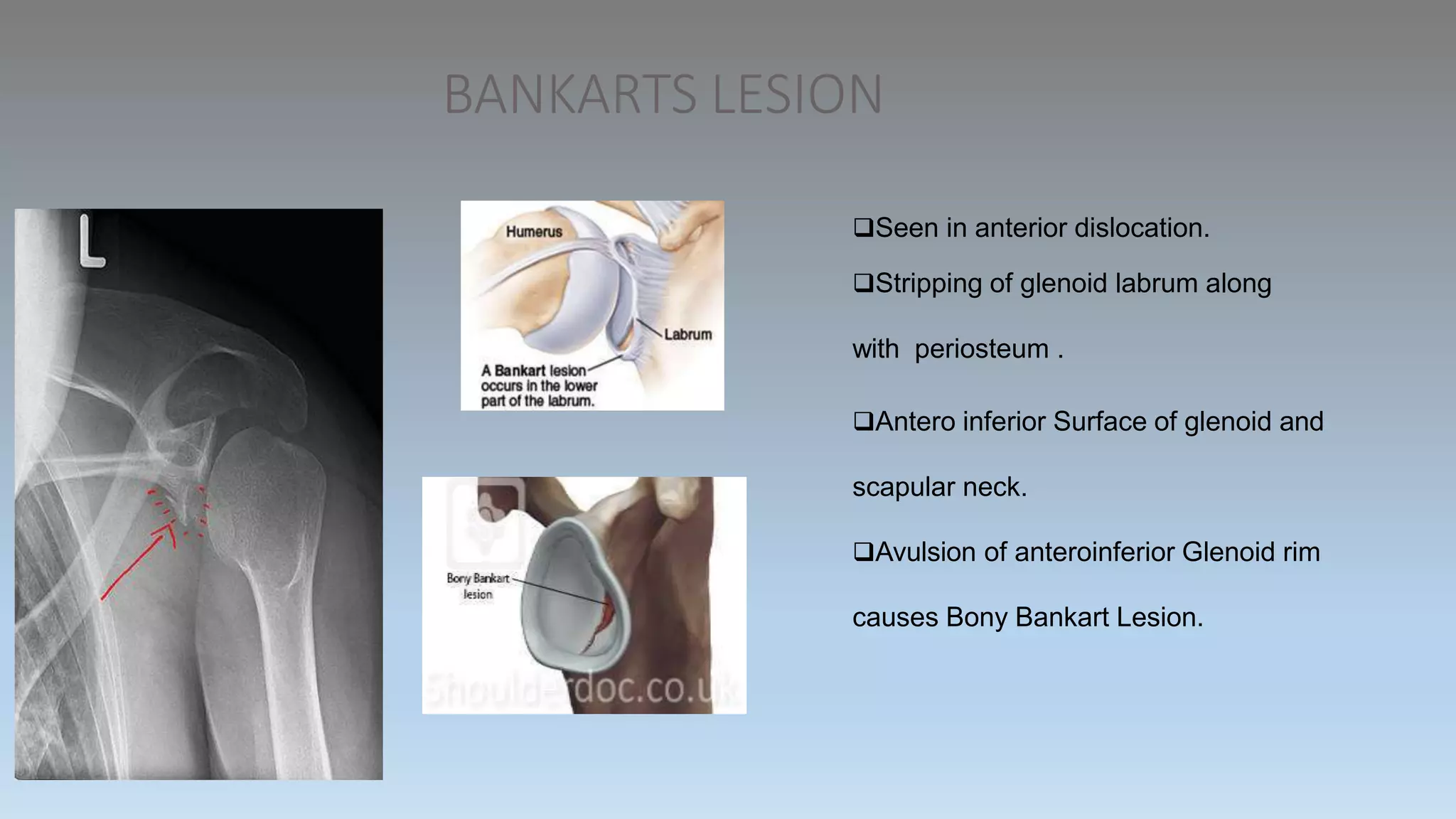
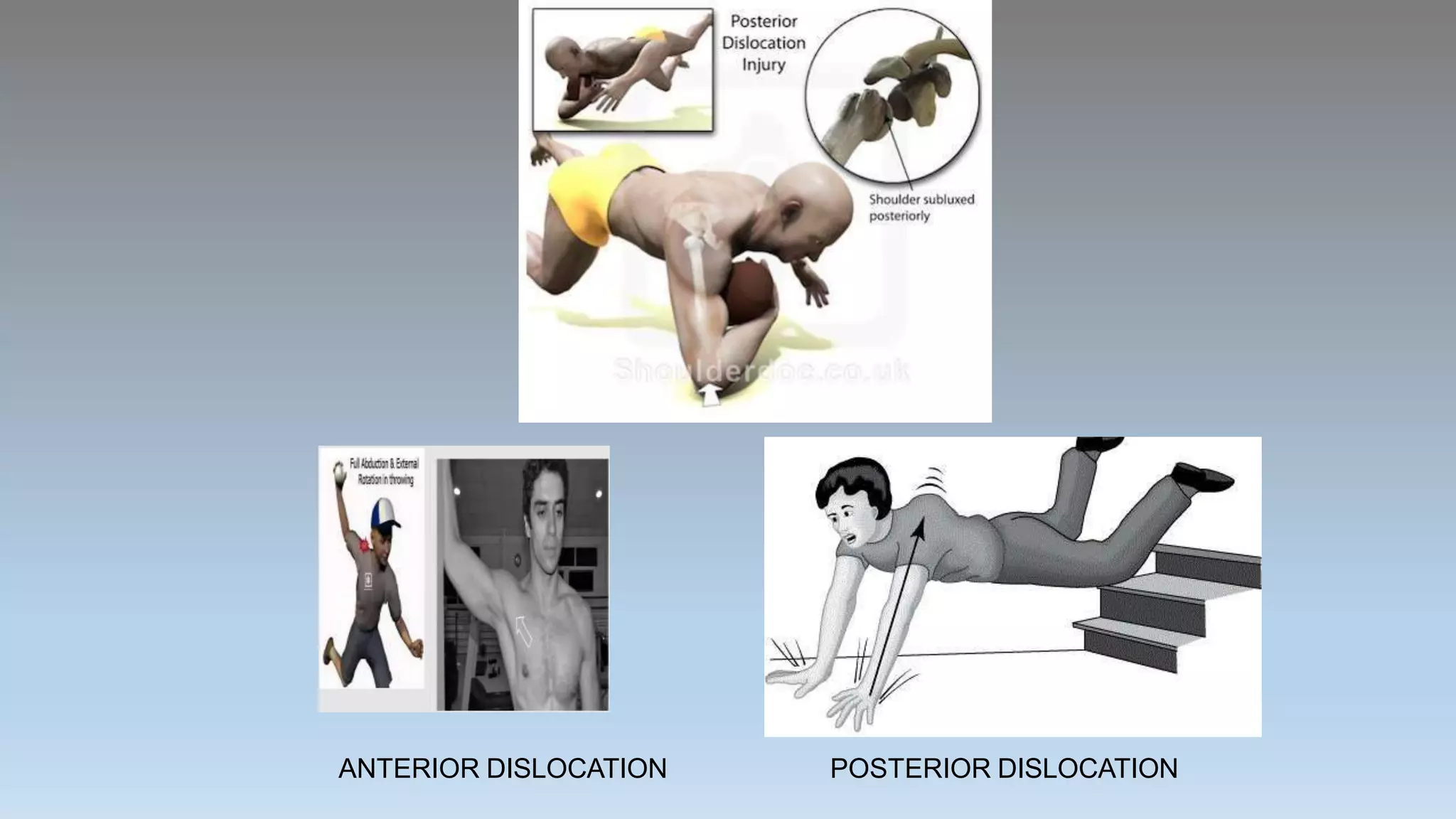
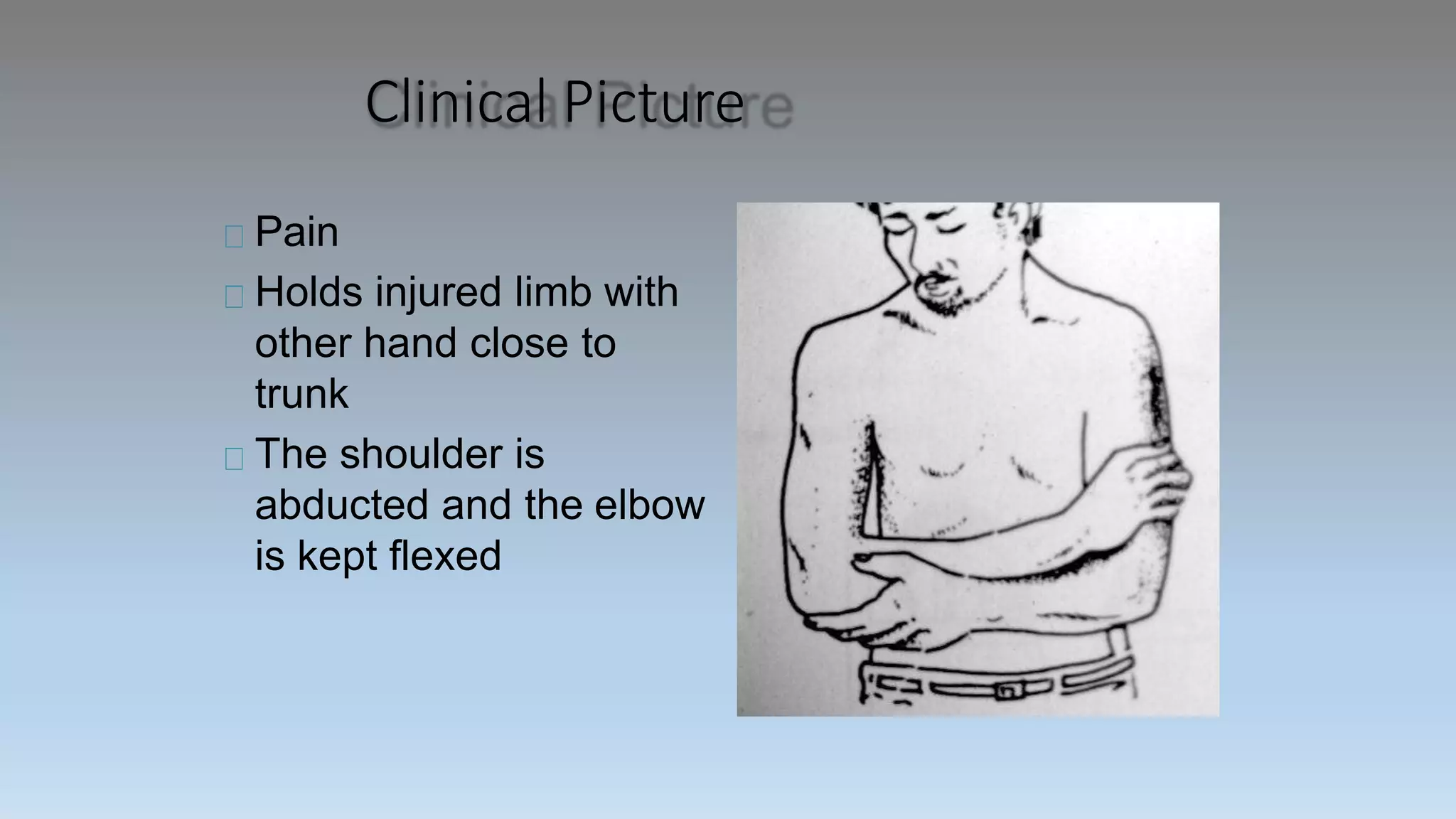
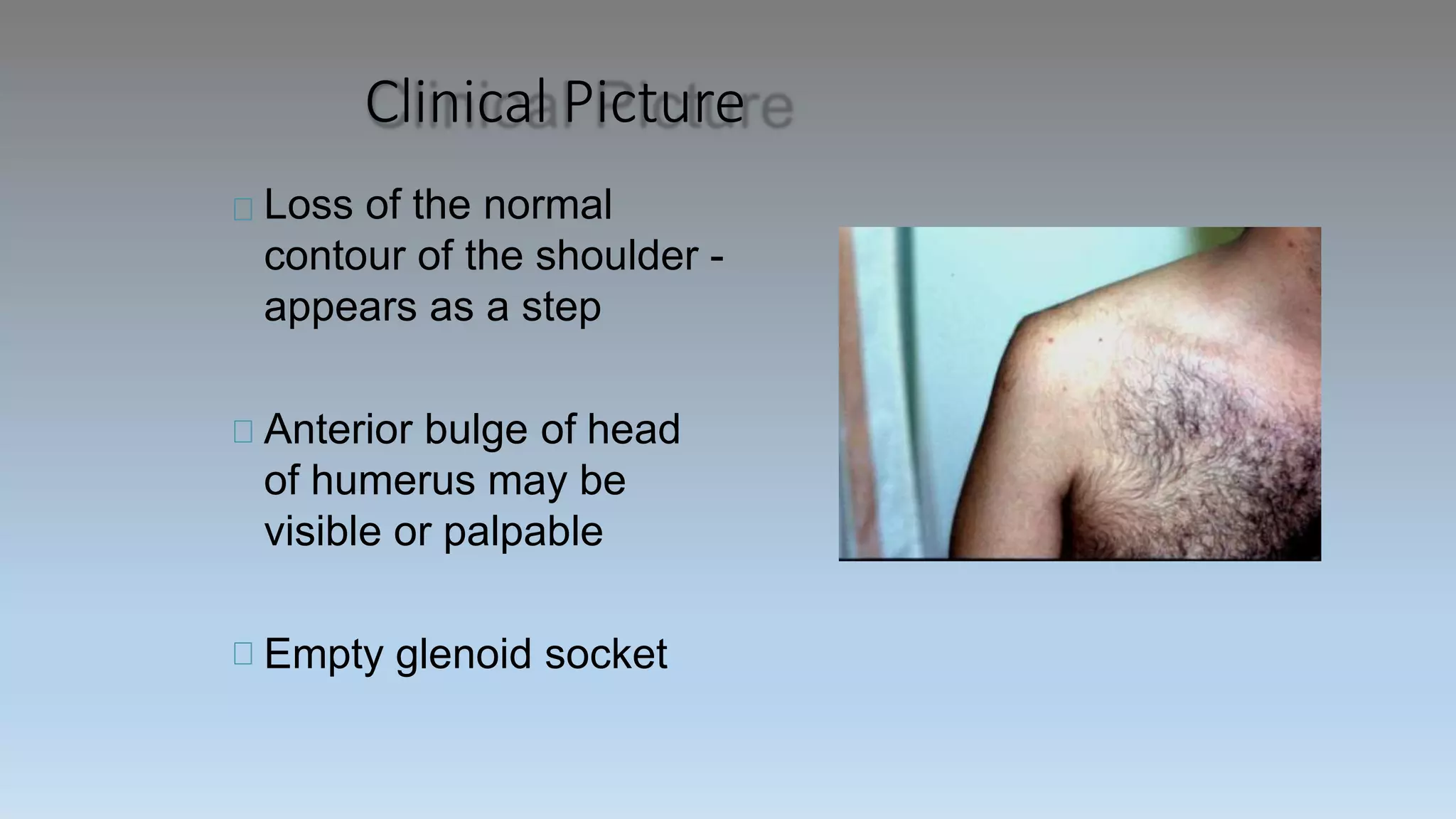
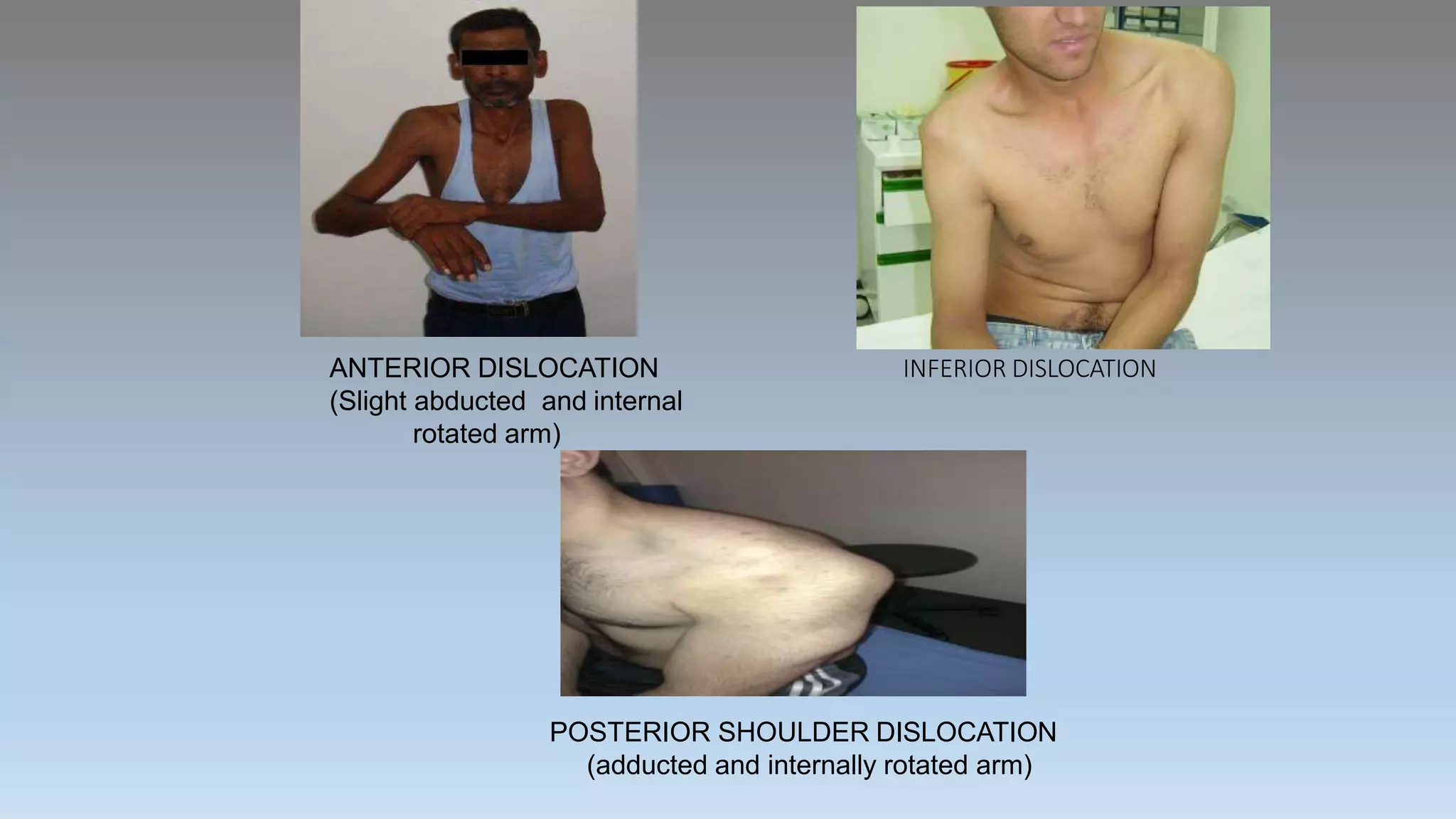
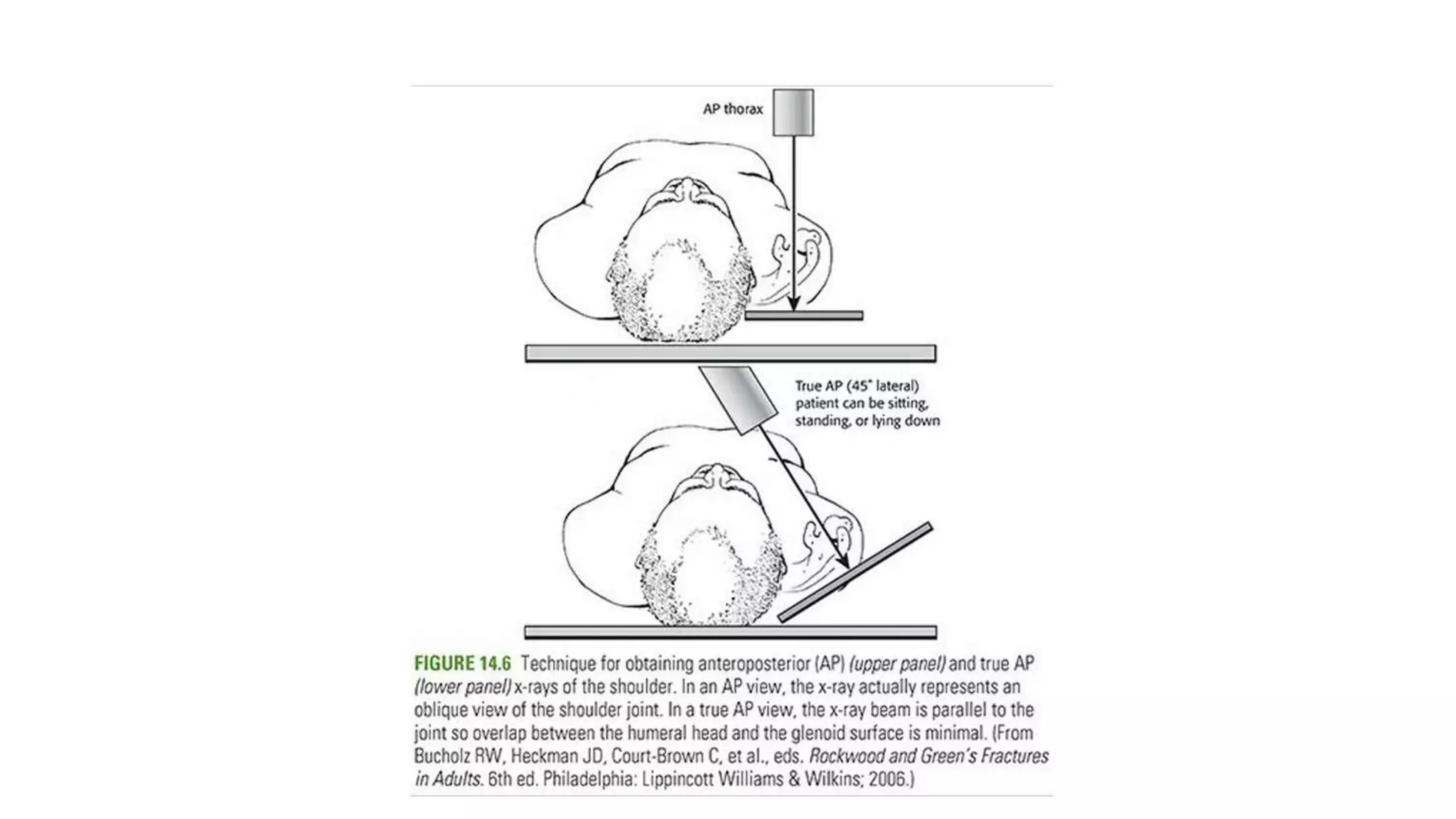
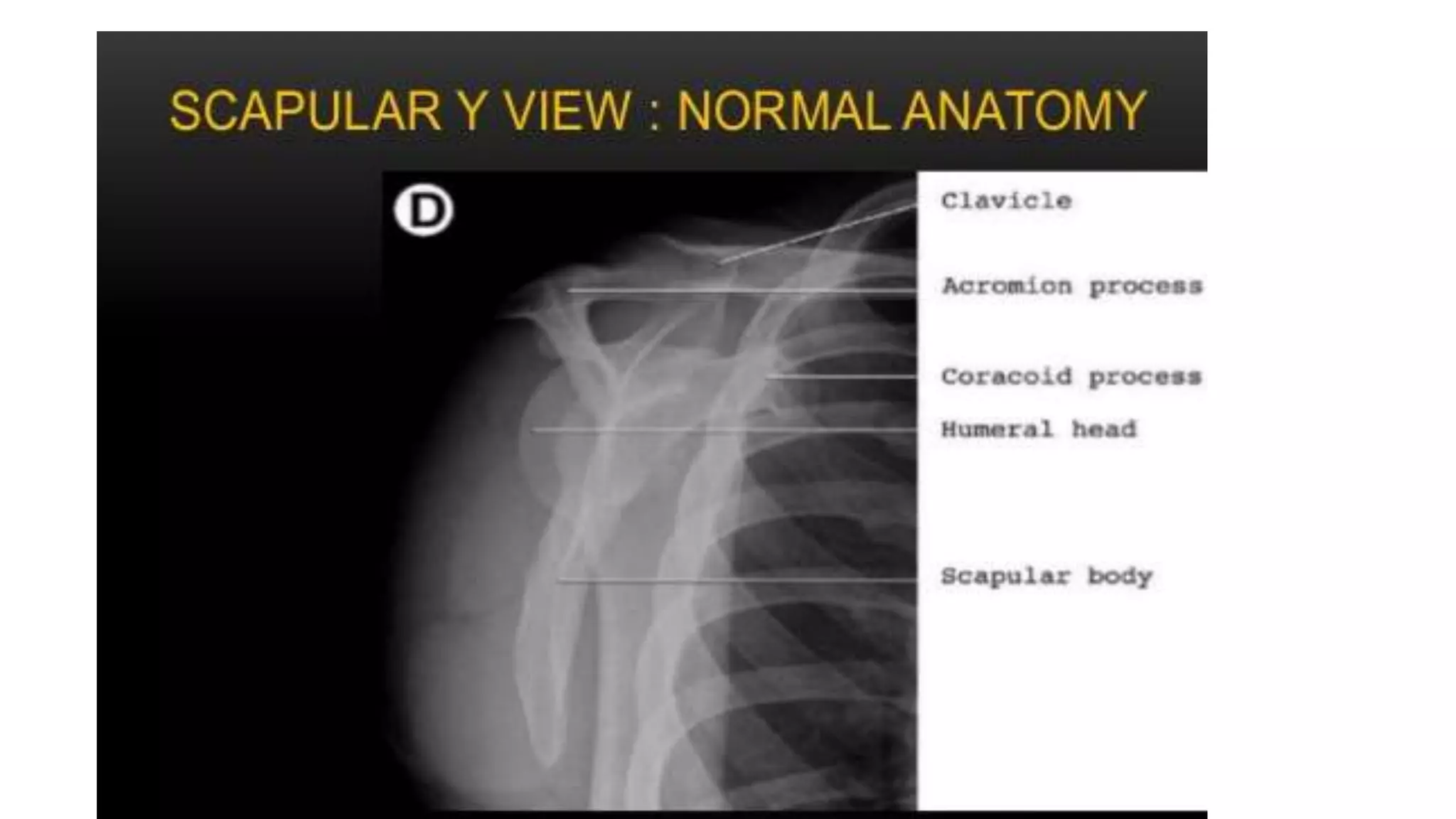
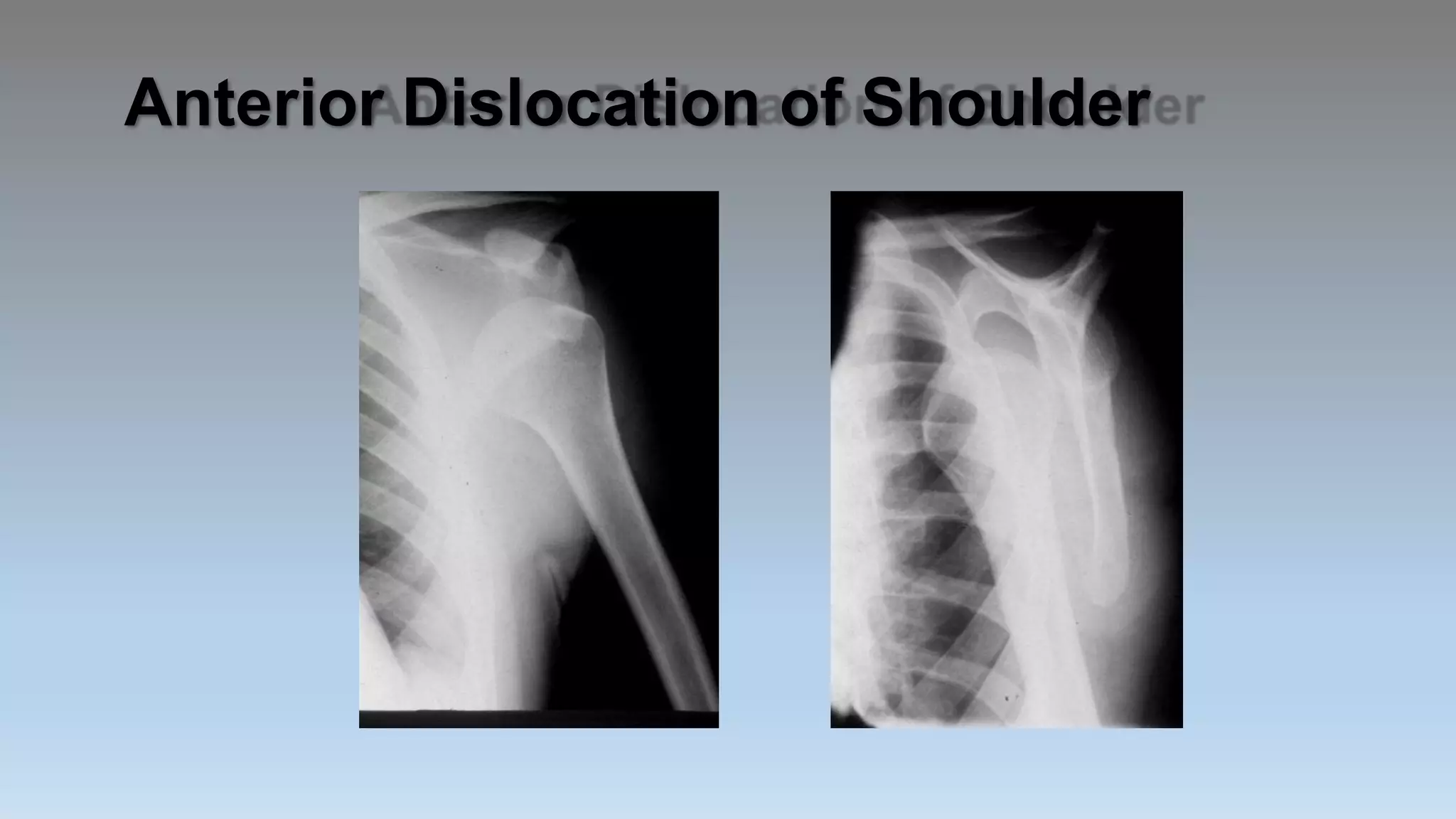
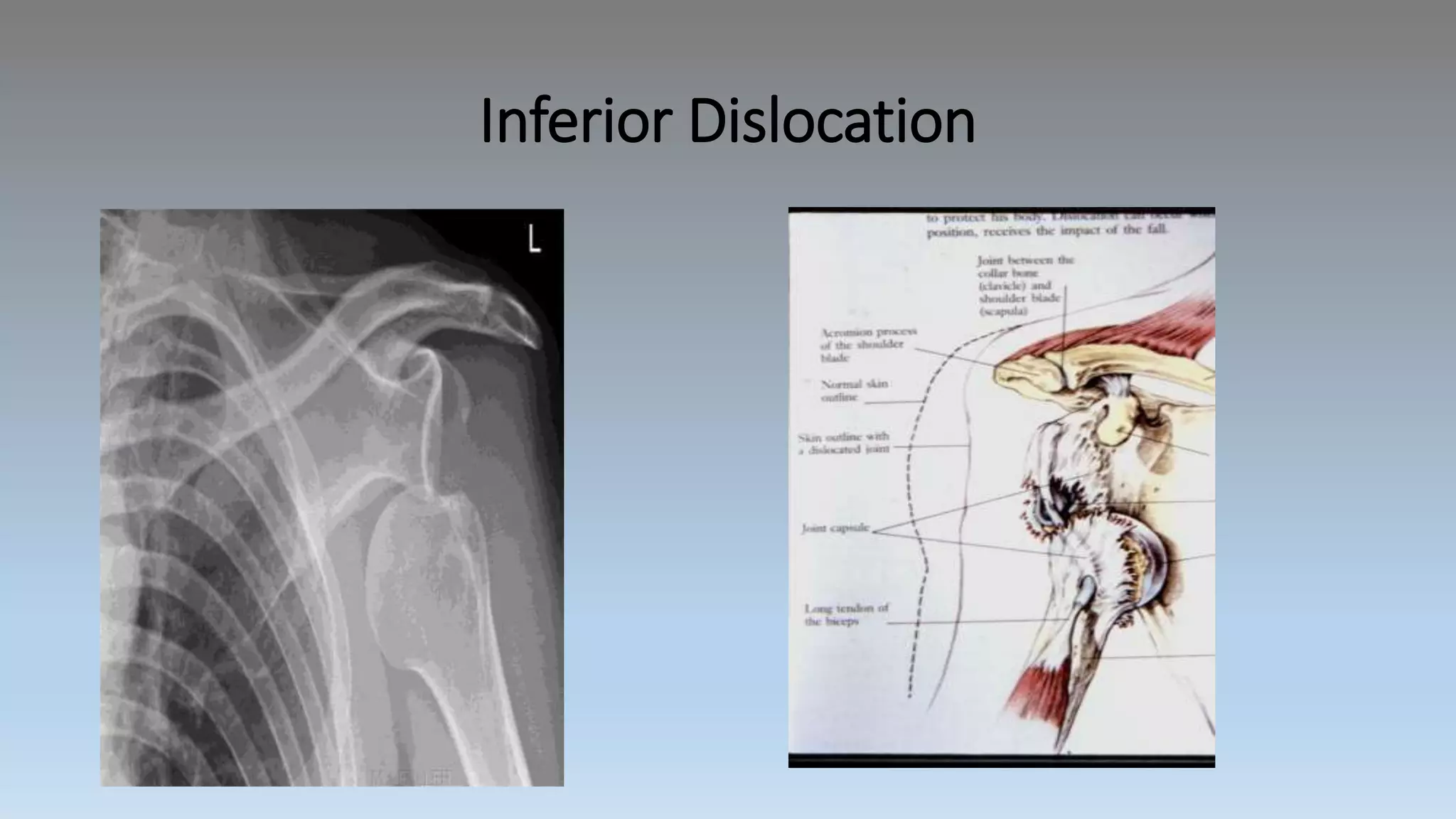
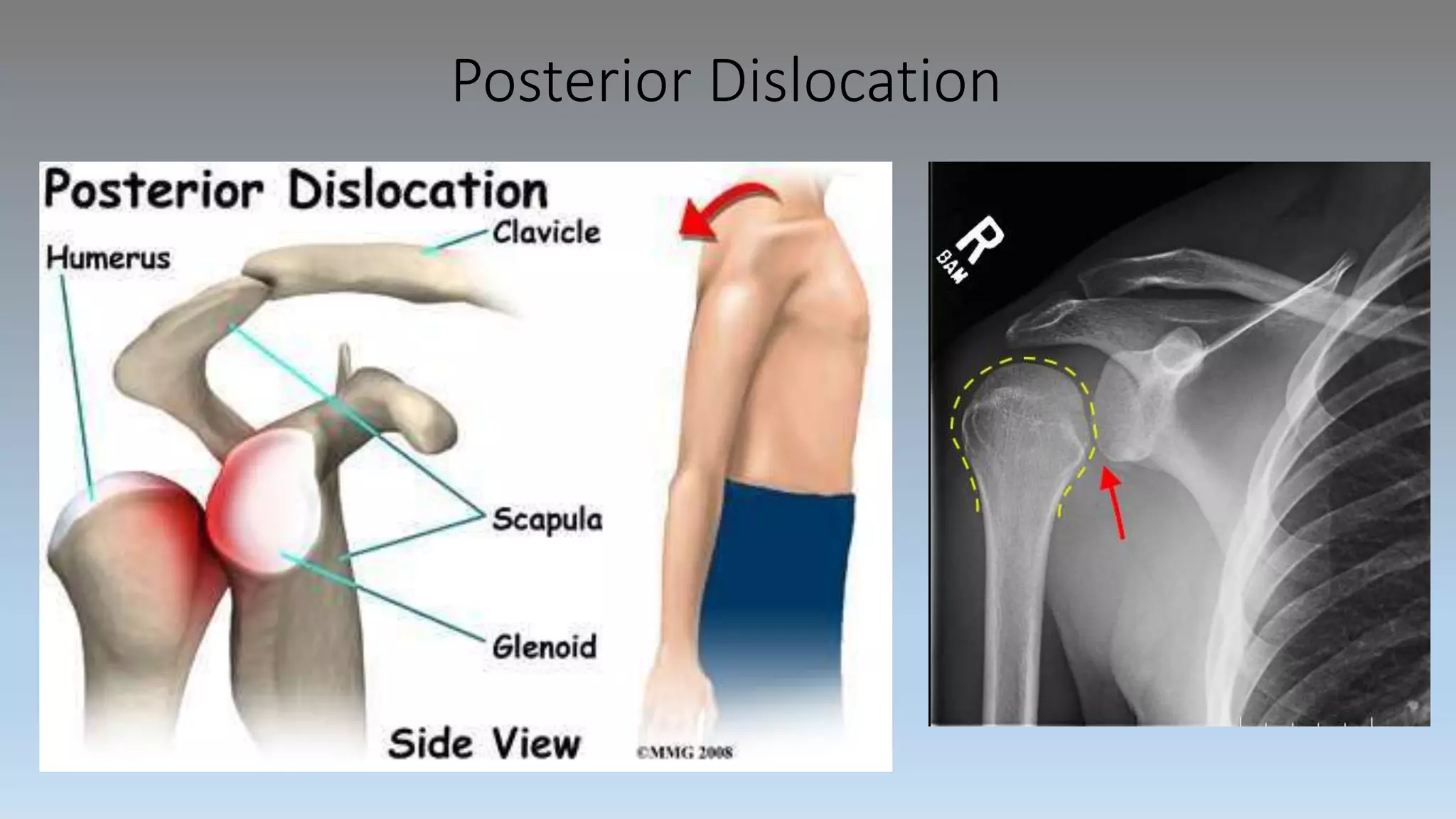
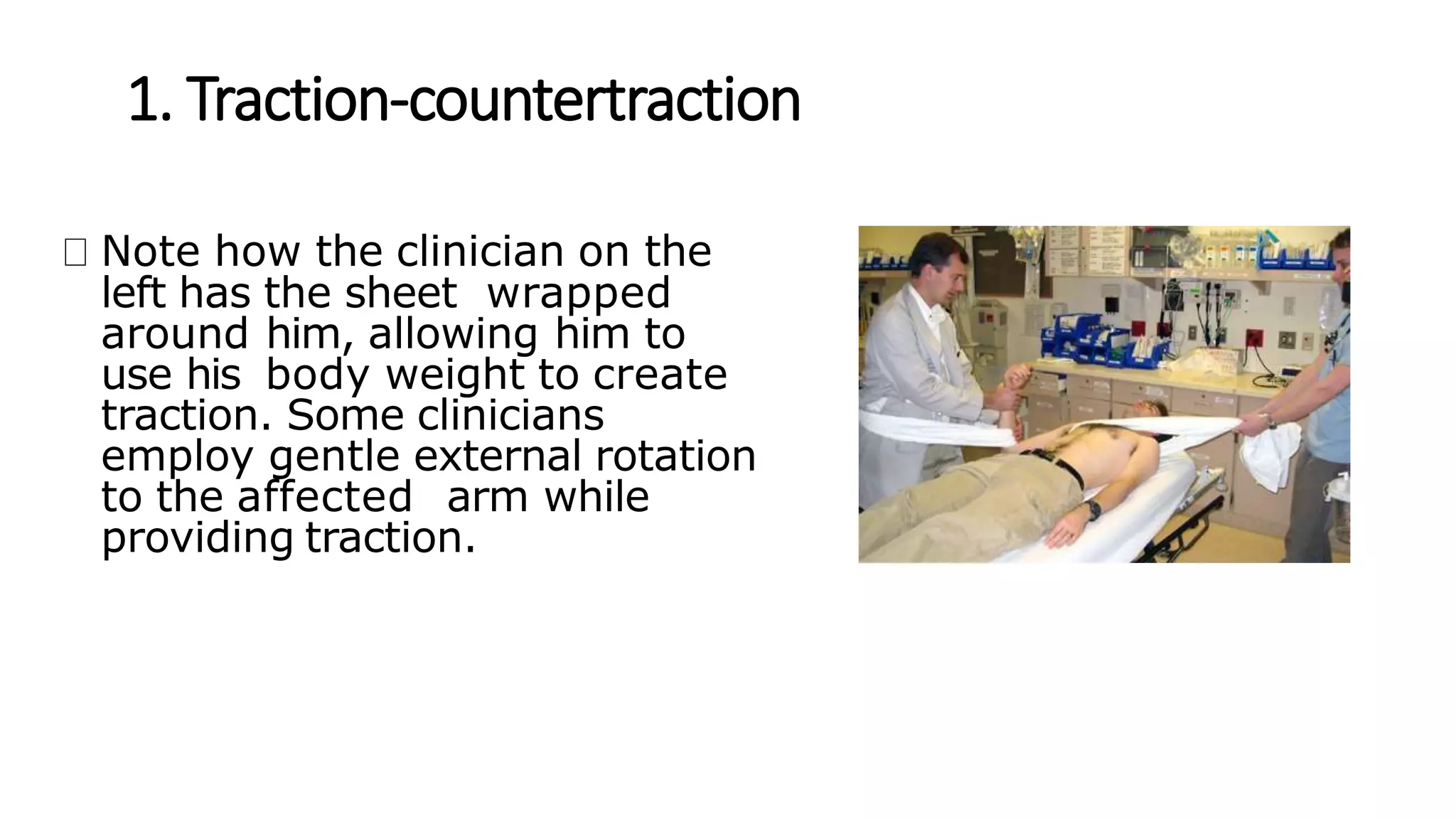
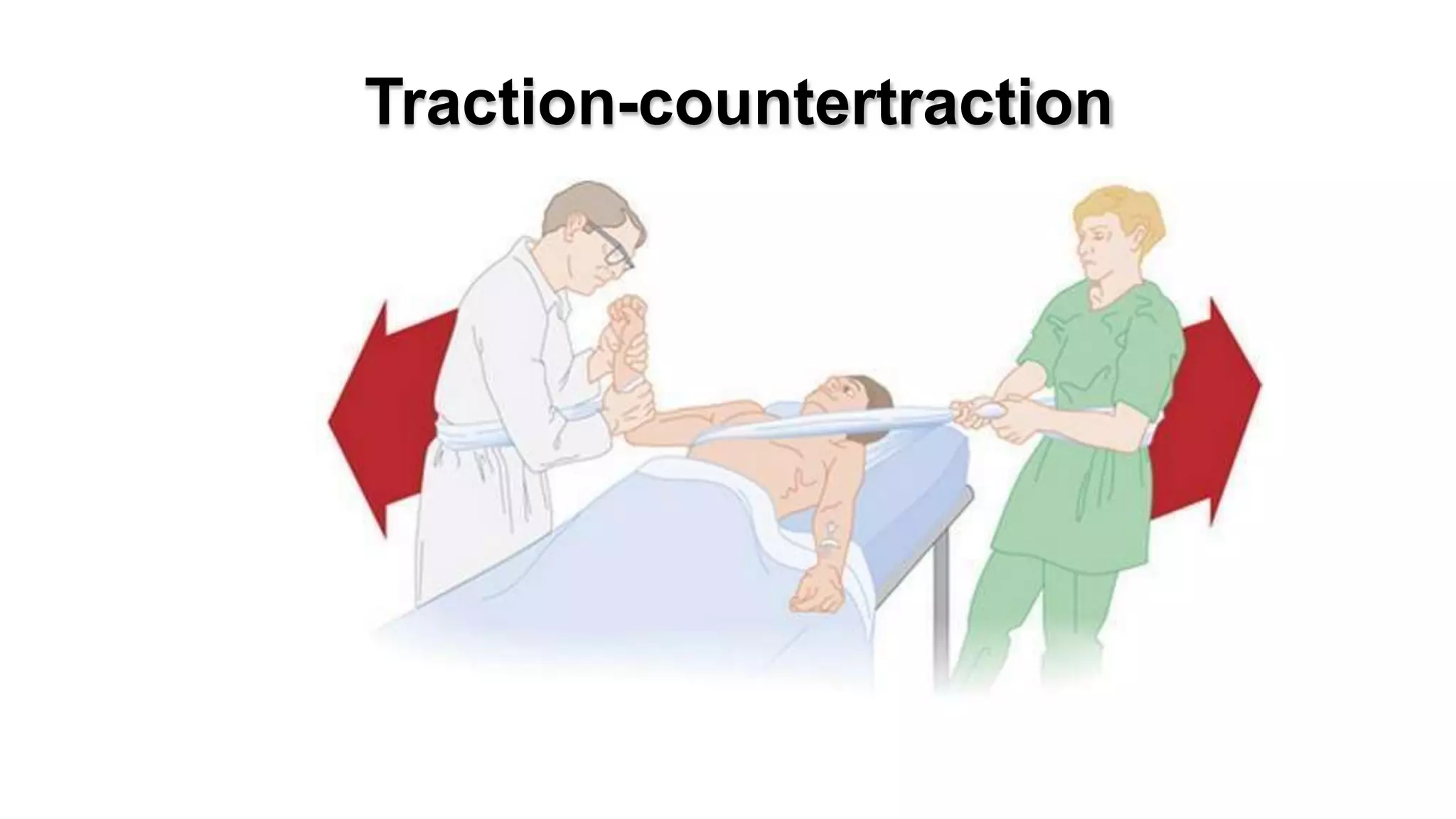
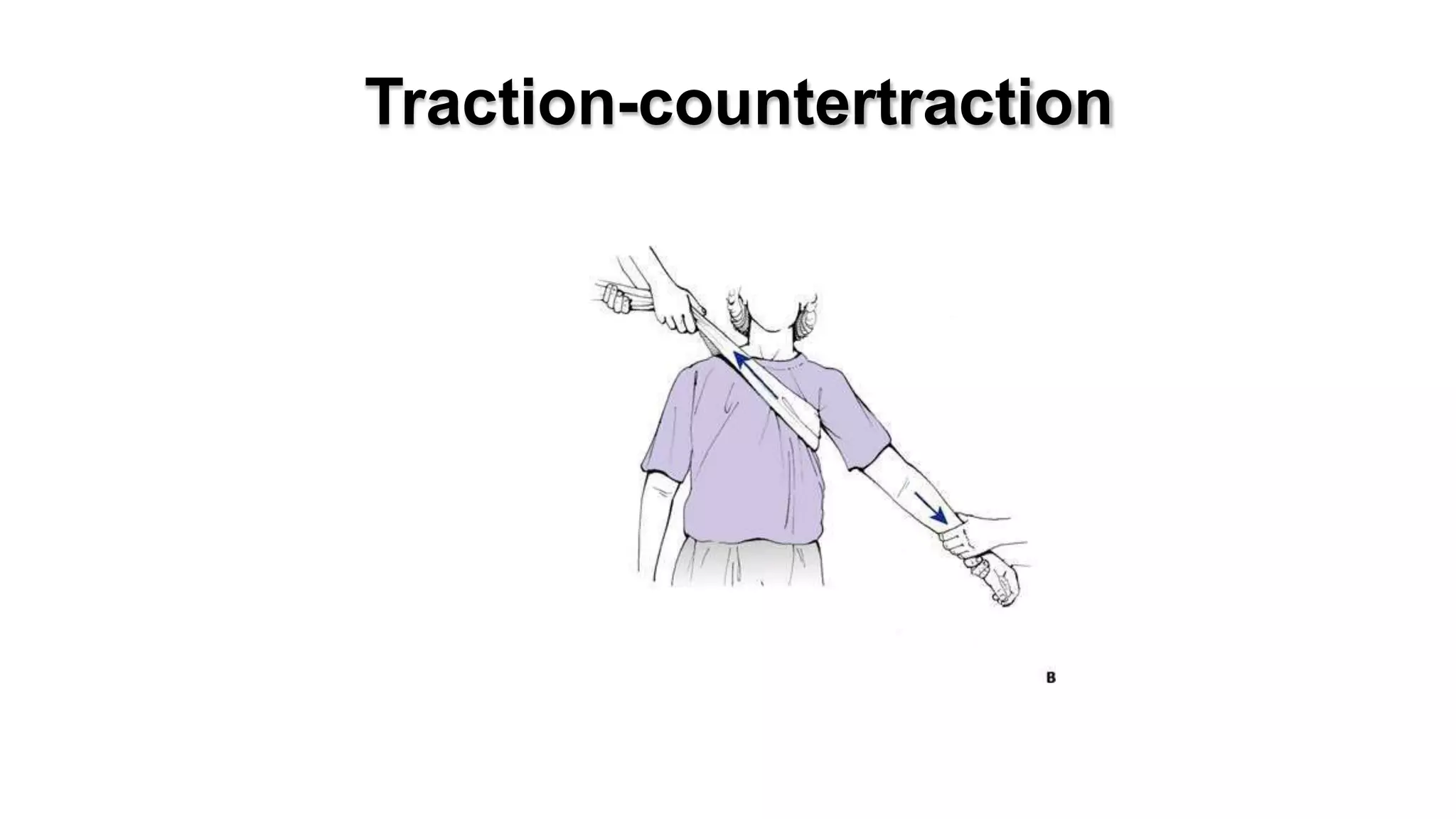
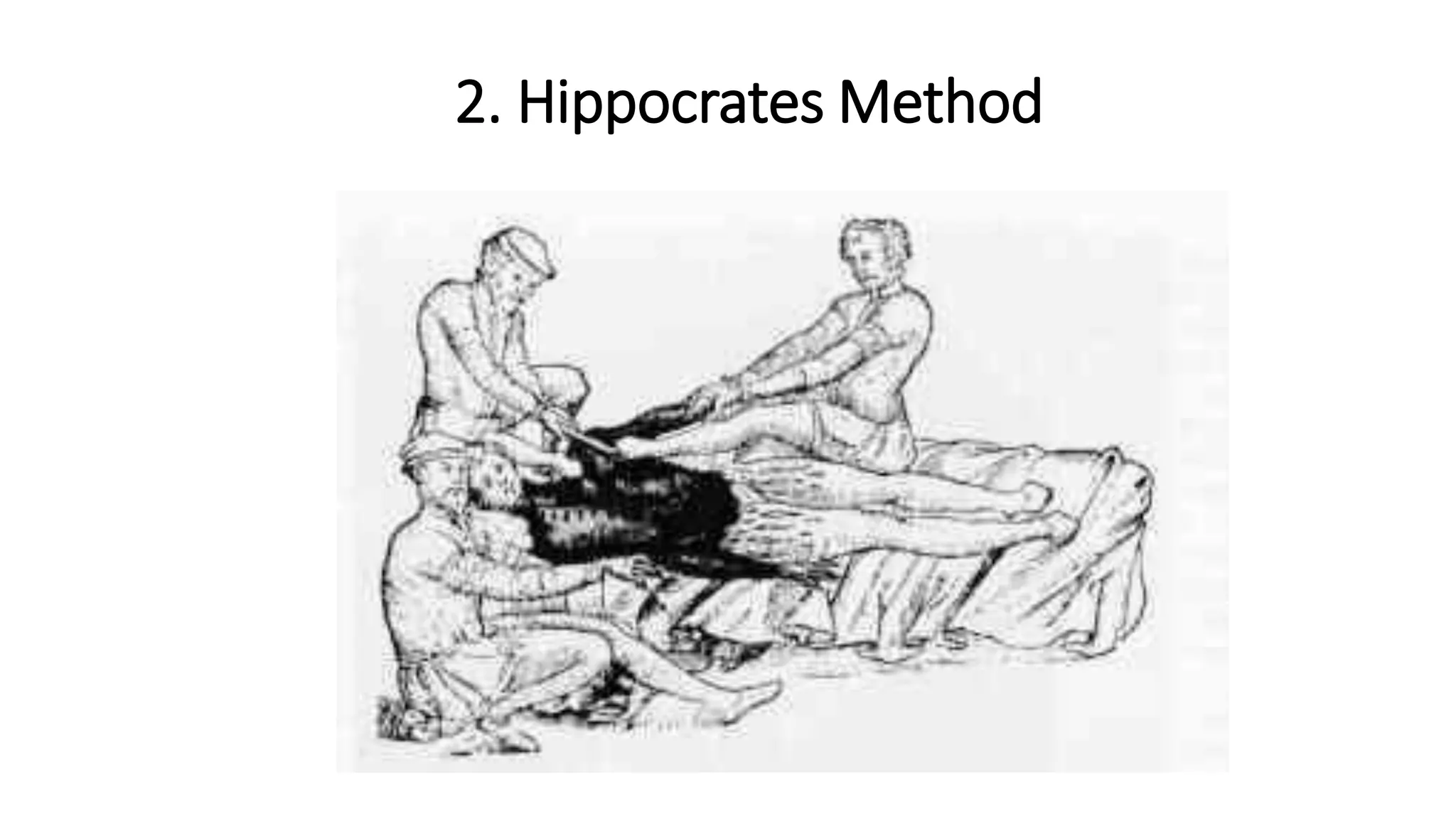
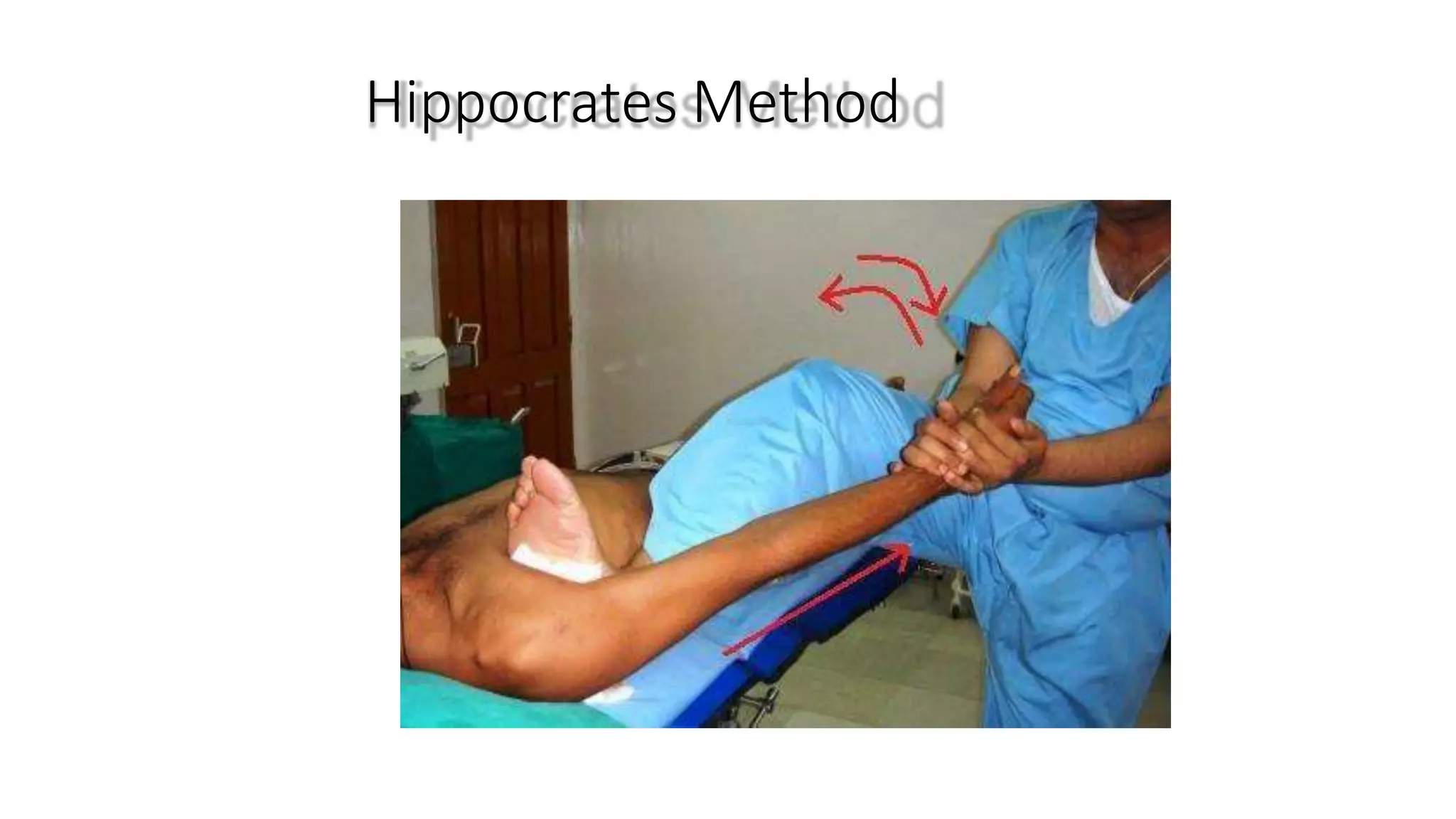
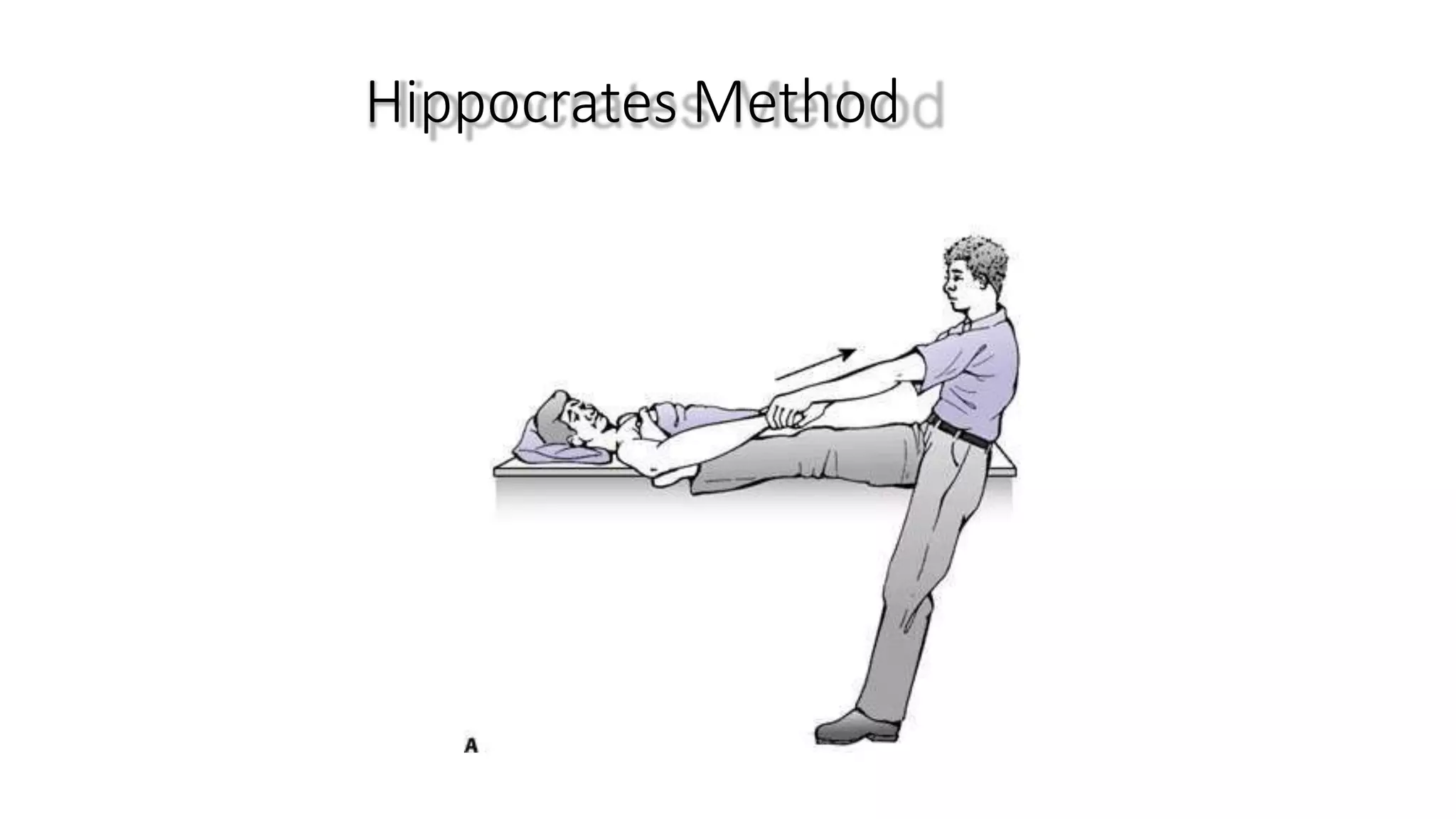
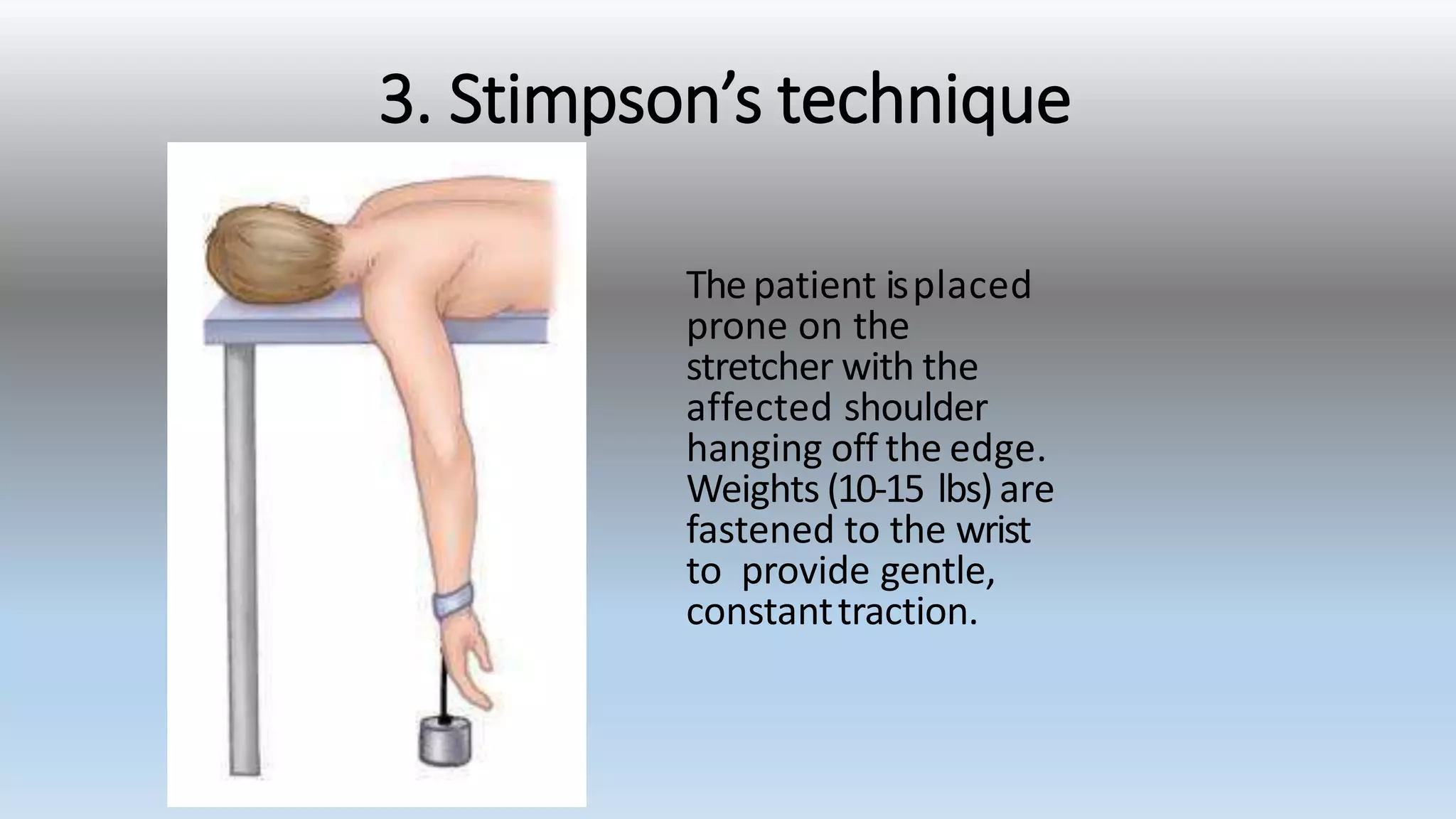
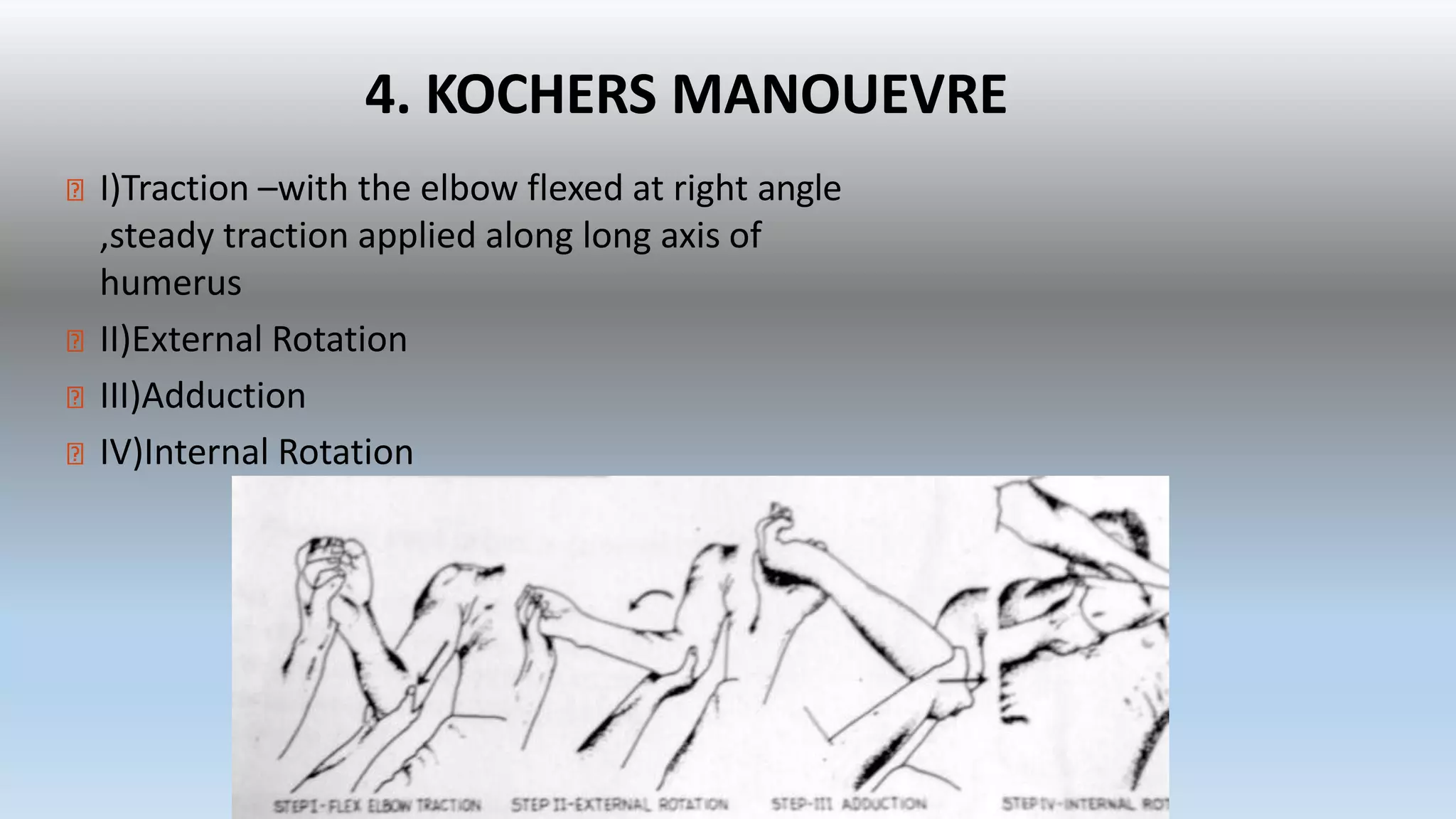
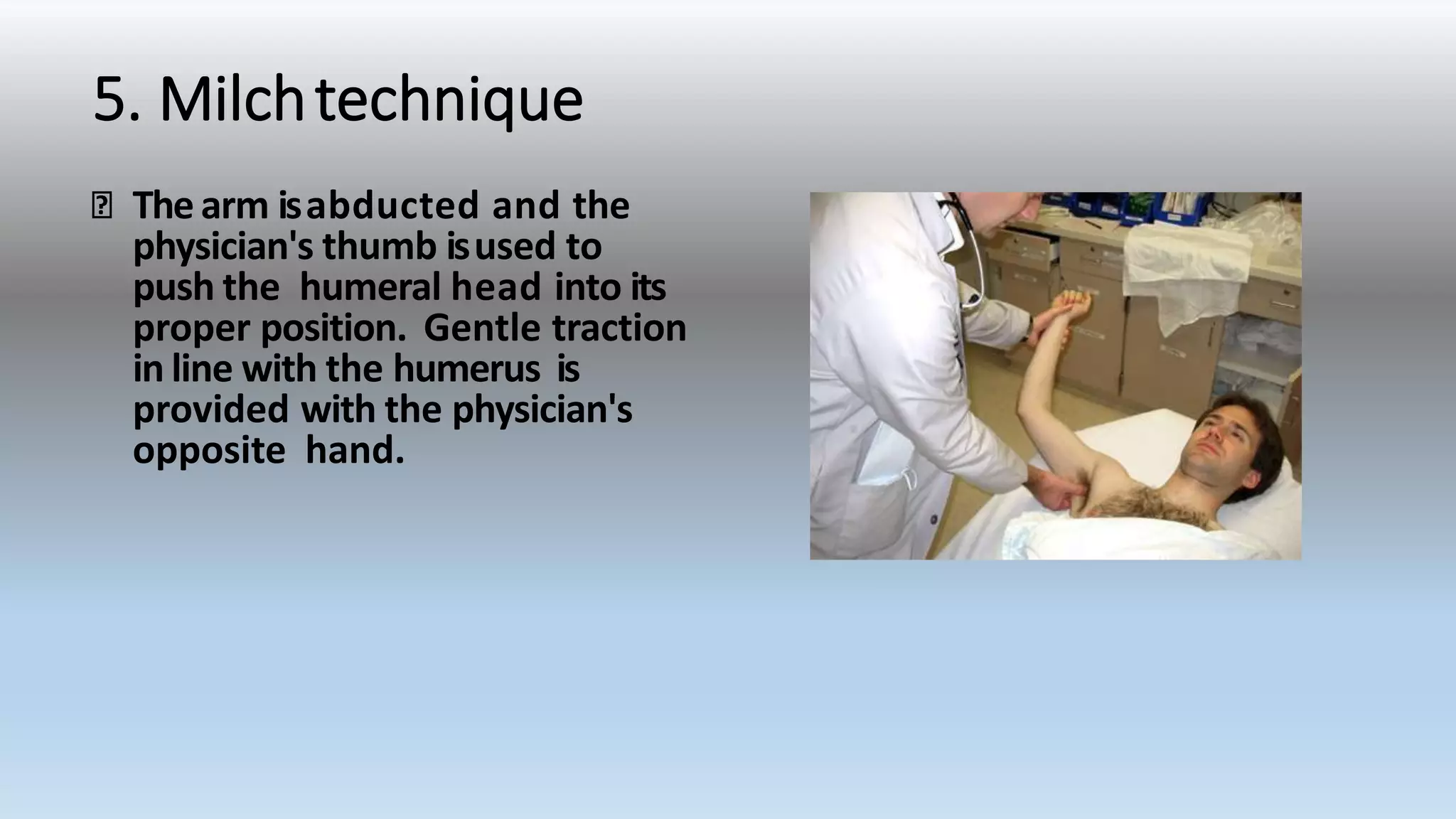
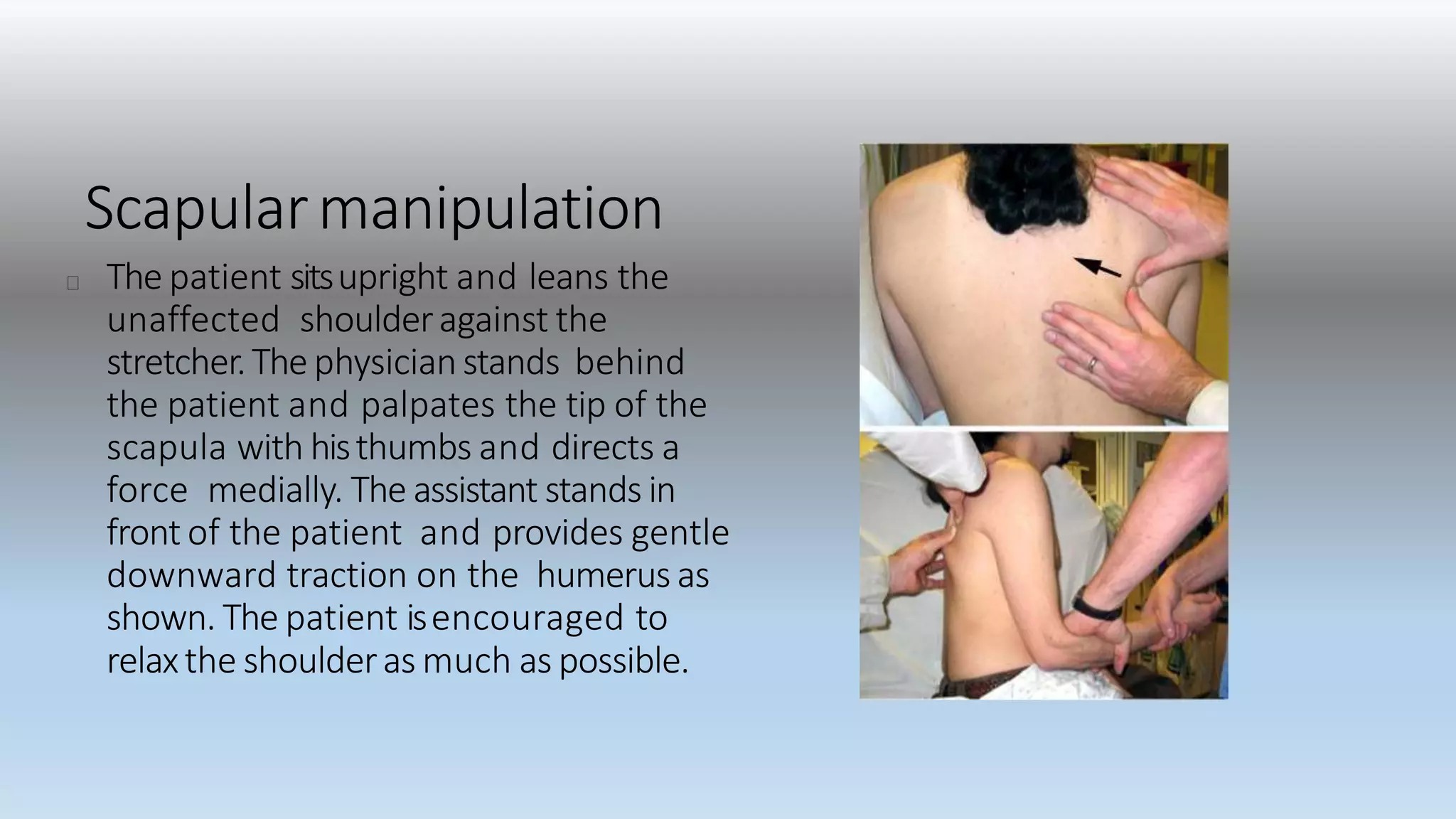


Shoulder dislocations have been depicted in Egyptian tomb art from 3000 BC. There are different types of shoulder dislocations including anterior, posterior, and inferior. Anterior dislocations are the most common. Clinical signs include pain, inability to contour the shoulder, and an anterior bulge. Radiographs can confirm and classify the dislocation. Reduction maneuvers include traction-countertraction, Hippocrates, Kocher, and scapular manipulation methods. Post-reduction, patients are immobilized and followed up to prevent recurrent dislocations, which occur in 50-90% of young patients.



































































