Downloaded 55 times











![Advertorial
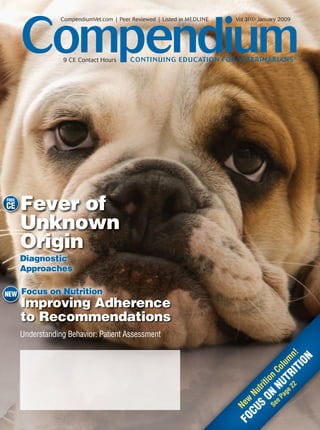
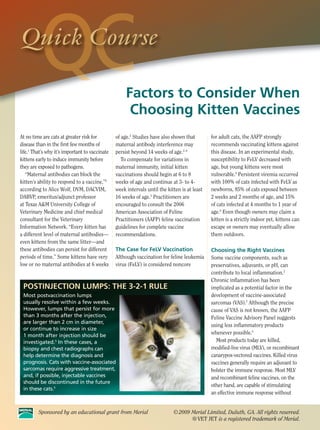
COLOSTRUM IN THE DIET
FOR CANINE INTESTINAL HEALTH AND IMMUNE SYSTEM SUPPORT
Arleigh Reynolds, DVM, PhD, DACVN COLOSTRUM BENEFITS SHOWN
Ebenezer Satyaraj, PhD Research shows dietary colostrum may benefit growing
While veterinarians have long recognized the connection puppies and adult dogs. Weaned puppies fed a bovine
between colostrum and enhanced immunity in newborns, colostrum–supplemented diet for 10 days after arrival at
recent research shows dogs of all ages can benefit from pet stores had significantly improved fecal quality compared
colostrum’s supportive effects on gastrointestinal (GI) health. to the control group.4 In a 40-week study, bovine colostrum
was fed to adult Alaskan sled dogs under exercise stress.5
The findings demonstrate that, while colostral antibodies Compared to controls, colostrum-supplemented dogs had:
are not absorbed by older puppies and adult dogs as in 1- or
2-day-old pups, the immunoglobulin-rich substance contains • Increased intestinal microflora diversity,5 which reduces
elements that support proper GI tract development, nutrient the risk of bacterial pathogens colonizing the GI tract.6
absorption, growth and healthy intestinal microflora.1 • More stable microbial populations following stress, which
GI TRACT KEY TO IMMUNE FUNCTION helps reduce risk of diarrhea and GI upset.5
The GI tract plays a vital role in protecting the body • Increased fecal IgA levels, indicating improved GI mucosal
from pathogens. With gut-associated lymphoid tissue immune status.5
(GALT), the intestinal tract is the body’s largest • Greater, persistent antibody levels following canine
immune organ.2,3 distemper virus (CDV) vaccination, suggesting enhanced
The intestinal mucosa provides a protective barrier and systemic immune status. The immune systems of
secretes immunoglobulin A (IgA), which helps neutralize colostrum-supplemented dogs were not hyperactive, based
potential pathogens and stabilize intestinal microflora. on normal C-reactive protein levels. 5
Measure of microflora stability
90
*
80
81.50
Percentage
70
60
50
40 46.00
30 Control
20 Colostrum
10
0 * <0.05
During stress, dogs fed a colostrum-supplemented
diet had more stable gut microflora.
1. Edwards, Christine. Interactions between nutrition and the intestinal microflora.
GI TRACT KEY TO IMMUNE FUNCTION Proc Nutr Soc. 1993;52(2):375–82.
2. Hall EJ. Mucosal immunity—Why it’s important [Internet]. In: The 32nd Congress of the
(1) Immunoglobulin (Ig) binds to an immune cell in the GI mucosa. World Small Animal Veterinary Association Proceedings Online; 2007 Aug 19–23; Sydney,
(2) Ig binding activates the immune cell. Australia. Available at: http://www.vin.com/proceedings/Proceedings.plx?CID=WSAVA
2007&PID=18137&Print=2986&O=Generic. Accessed April 25, 2008.
(3) Cytokines are secreted into the circulatory system, enabling 3. Tizard IR. Immunity at body surfaces. In: Tizard IR, ed. Veterinary Immunology: An
communication with other immune cells. Introduction. 7th ed. Philadelphia, Pa: Saunders; 2004:234–246.
(4a) Activated systemic immune cells release IgG into the 4. Giffard CJ, Seino MM, Markwell PJ, Bektash RM. Bene ts of bovine colostrum on fecal
quality in recently weaned puppies. J Nutr. 2004;134:2126S–2127S.
circulatory system in response to immune system challenges. 5. Data on le, 2006. Nestlé Purina PetCare Company.
(4b) Mucosal immune cells release IgA into the GI tract lumen, 6. Kuehl CJ, Wood HD, Marsh TL, et al. Colonization of the cecal mucosa by
Helicobacter hepaticus impacts the diversity of the indigenous microbiota. Infect Immun.
leading to increased levels of fecal IgA. 2005;73:6952–6961.](https://image.slidesharecdn.com/pv0109-091029165255-phpapp02/85/Pv0109-14-320.jpg)







![FREE
CE The Diagnostic Approach to FUO in Dogs
7. Battersby IA, Murphy KF, Tasker S, et al. Retrospective study of Disease. 5th ed. Philadelphia: Saunders; 1997:1077.
fever in dogs: laboratory testing, diagnoses and influence prior to 23. Lelièvre H, Gimenez M, Vandenesch F, et al. Multicenter clinical
treatment. J Small Anim Pract 2006;47:370-376. comparison of resin-containing bottles with standard aerobic and
8. Dunn KJ, Dunn JK. Diagnostic investigations in 101 dogs with anaerobic bottles for culture of microorganisms from blood. Eur J
pyrexia of unknown origin. J Small Anim Pract 1998;39:574-580. Clin Microbiol Infect Dis 1997;16(9):669-674.
9. Mourad O, Palda V, Detsky AS. A comprehensive evidence- 24. MacDonald KA, Chomel BB, Kittleson MD, et al. A prospective
based approach to fever of unknown origin. Arch Intern Med study of canine infective endocarditis in Northern California (1999–
2003;163:545-551. 2001): emergence of Bartonella as a prevalent etiologic agent. J Vet
10. Roth AR, Basello GM. Approach to the adult patient with fever Intern Med 2004;18:56-64.
of unknown origin. Am Fam Phys 2003;68:2223-2228. 25. Gebert S, Siegel D, Wellinghausen N. Rapid detection of patho-
11. Johnson DH, Cunha BA. Drug fever. Infect Dis Clin North Am gens in blood culture bottles by real-time PCR in conjunction with
1996;10:85-91. the pre-analytic tool MolYsis. J Infect 2008;57:307-316.
12. Wess G, Unterer S, Haller M, et al. Recurrent fever as the only 26. Greene CE, Budsberg SC. Musculoskeletal infections. In: Greene
or predominant clinical sign in four dogs and one cat with con- CE, ed. Infectious Diseases of the Dog and Cat. 3rd ed. St. Louis:
genital portosystemic vascular anomalies. Schweiz Arch Tierheilkd Elsevier Saunders; 2006:823-841.
2003;145(8):363-368. 27. Goldstein RE. Swollen joints and lameness. In: Ettinger SJ,
13. Mattoon JS, Nyland TG. Thorax. In: Nyland TG, Mattoon JS, Feldman EC, eds. Textbook of Veterinary Internal Medicine. Vol 1.
eds. Small Animal Diagnostic Ultrasound. 2nd ed. Philadelphia: 6th ed. St. Louis: Elsevier Saunders; 2005:83-87.
Saunders; 2002:325-353. 28. Houser G, Ayoob A, Greene CE. Laboratory testing for infec-
14. Samii VF, Long CD. Musculoskeletal system. In: Nyland TG, tious diseases of dogs and cats. Appendix 5. In: Greene CE, ed.
Mattoon JS, eds. Small Animal Diagnostic Ultrasound. 2nd ed. Infectious Diseases of the Dog and Cat. 3rd ed. St. Louis: Elsevier
Philadelphia: Saunders; 2002:267-284. Saunders; 2006:1139-1168.
15. Mattoon JS, Nyland TG. Eye. In: Nyland TG, Mattoon JS, eds. 29. Moon ML, Hinkle GN, Krakowka GS. Scintigraphic imaging
Small Animal Diagnostic Ultrasound. 2nd ed. Philadelphia: Saun- of technetium 99m-labeled neutrophils in the dog. Am J Vet Res
ders;2002:305-324. 1988;49(6):950-955.
16. Wisner ER, Mattoon JS, Nyland TG. Neck. In: Nyland TG, Mat- 30. Peremans K, DeWinter F, Janssens L, et al. An infected hip
toon JS, eds. Small Animal Diagnostic Ultrasound. 2nd ed. Philadel- prosthesis in a dog diagnosed with a 99mTC-ciprofloxacin (infec-
phia: Saunders; 2002:285-304. tion) scan. Vet Radiol Ultrasound 2002;43(2):178-182.
17. MacDonald KA. Infective endocarditis. In: Bonagura JD, Twedt 31. Berry CR, DeGrado TR, Nutter F, et al. Imaging of pheochromo-
DC, eds. Kirk’s Current Veterinary Therapy XIV (Small Animal Prac- cytoma in 2 dogs using p-[18F]fluorobenzylguanidine. Vet Radiol
tice). St. Louis: Elsevier Saunders; 2009:786-791. Ultrasound 2002;43(2):183-186.
18. Hirsh DC, Jang SS, Biberstein EL. Blood culture of the canine 32. Ballegeer EA, Forrest LJ, Jeraj R, et al. PET/CT following inten-
patient. JAVMA 1984;184(2):175-178. sity-modulated radiation therapy for primary lung tumor in a dog.
19. Haggstrom J, Kvart C, Pedersen HD. Acquired valvular heart Vet Radiol Ultrasound 2006;47(2):228-233.
disease. In: Ettinger SJ, Feldman EC, eds. Textbook of Veterinary 33. LeBlanc AK, Jakoby B, Townsend DW, et al. Thoracic and ab-
Internal Medicine. Vol 2. 6th ed. St. Louis: Elsevier Saunders; dominal organ uptake of 2-deoxy-2-[18F]fluoro-D-glucose (18FDG)
2005:1022-1039. with positron emission tomography in the normal dog. Vet Radiol
20. Calvert CA, Wall M. Cardiovascular infections. In: Greene CE, Ultrasound 2008;49(2):182-188.
ed. Infectious Diseases of the Dog and Cat. 3rd ed. St. Louis: El- 34. Lappin MR. Practical antimicrobial chemotherapy. In: Nelson
sevier Saunders; 2006:841-865. RW, Couto CG, eds. Small Animal Internal Medicine. 4th ed. St.
21. Li J, Plorde JJ, Carlson LG. Effects of volume and periodicity on Louis: Elsevier; 2009:1291-1301.
blood cultures. J Clin Microbiol 1994;32(11):2829-2831. 35. Klein NC, Cunha BA. Treatment of fever. Infect Dis Clin North
22. Karchmer A. Infective endocarditis. In: Braunwald E, ed. Heart Am 1996;10(1):211-216.
3 CE
CREDITS CE TEST 1 This article qualifies for 3 contact hours of continuing education credit from the Auburn University College of
Veterinary Medicine. Subscribers may take individual CE tests online and get real-time scores at CompendiumVet.com.
Those who wish to apply this credit to fulfill state relicensure requirements should consult their respective state authorities
regarding the applicability of this program.
1. Which statement regarding the investi- 2. What is the correct definition of a true 3. Which statement regarding fever in dogs
gation of FUO in dogs is false? fever? is true?
a. Two-view abdominal and three-view a. increase in body temperature due to an a. The cause of fever in most dogs is
thoracic radiographs are recommended. elevation of the thermal set point in the neoplasia.
b. Joint radiographs can aid in the diag- anterior hypothalamus b. Most FUOs in dogs are caused by a
nosis of an erosive immune-based b. increase in body temperature due to an common disease presenting in an
polyarthritis. elevation of the thermal set point in the obscure fashion.
c. Thoracic ultrasonography should anterior pituitary gland c. Dogs with true fevers commonly
always be conducted, especially if c. a marked, rapid rise in body tempera- have prolonged body temperatures
abnormalities are not detected on tho- ture without adjustment of the thermal above 106°F.
racic radiographs. set point in the anterior hypothalamus d. Prolonged body temperatures
d. Dogs with infective endocarditis are d. a marked, rapid rise in body tempera- above 106°F are not dangerous.
usually medium to large breeds that ture without adjustment of the
do not tend to have myxomatous valve thermal set point in the anterior
degeneration. pituitary gland
20 Compendium: Continuing Education for Veterinarians® | January 2009 | CompendiumVet.com](https://image.slidesharecdn.com/pv0109-091029165255-phpapp02/85/Pv0109-22-320.jpg)



![Letters
The Curious Case of
the Cat with the Munchies
We found the article “Five Common Toxins
Ingested by Dogs and Cats” extremely in-
teresting and practical. We recently treated
a 5-month-old domestic shorthaired cat for CE Article #1
Five Common Toxins Ingested
marijuana toxicity following ingestion of a by Dogs and Cats
Julie Ann Luiz, DVM
“hash brownie.” The cat presented with per- University of Hawaii at Hilo
Johanna Heseltine, DVM, MS, DACVIM
Oklahoma State University
plexing sudden-onset neurologic signs and ABSTRACT: Substances that are toxic to pets are present in most households. Early identification of
intoxication is crucial to preventing or minimizing gastrointestinal absorption of toxins.The history,
clinical signs, and laboratory test results can be used to make a presumptive diagnosis and begin therapy.
hypothermia (temperature 94.5°F [34.7°C]). O
nce absorbed from the gastrointestinal
(GI) tract, many toxins lack a specific
antidote and are associated with severe
systemic effects that are difficult to treat.
in veterinary medicine are derived from the
human medical literature. Decontamination and
treatment strategies for the toxins discussed in
this article are summarized in Table 1.
Therefore, prompt decontamination is the first
With gentle coaxing, the owners admitted step in managing patients that have ingested
toxic materials. If the toxin ingested is known,
therapy should be initiated before clinical signs
develop. This article discusses the general prin-
Emesis Induction
If the owner suspects toxicosis and calls the
clinic before presenting the animal, the veteri-
narian must consider the risks and benefits
ciples for minimizing GI absorption of ingested of instructing the owner to administer an
the source of the problem. (The brownie had toxins and the clinical presentation and man-
agement of toxicosis caused by five commonly
ingested household substances: anticoagulant
rodenticides, ethylene glycol (EG), marijuana,
emetic.1 Productive emesis requires the pres-
ence of food or liquid in the stomach, espe-
cially for retrieval of small volumes of toxin.2
Removal of the poison from the stomach is
chocolate, and metaldehyde. most effective within 1 hour of ingestion, is
been carefully wrapped in plastic film and
useful up to 2 hours after ingestion, and is of
DECONTAMINATION STRATEGIES limited benefit more than 4 hours after inges-
FOR ORALLY INGESTED TOXINS tion.2,3 Early emesis may remove up to 80% of
GI decontamination techniques are used to pre- the ingested material.3
vent or limit the absorption of ingested toxins. Induction of emesis is contraindicated for
Because many toxins lack a specific antidote, corrosive and caustic materials, as well as for
hidden but had disappeared while the patient • Take CE tests
decreasing the amount of
toxin absorbed may be life -
saving, and decontamination
strategies should begin as soon
petroleum distillates and other volatile materials
that may result in aspiration pneumonia. 2,3
Vomiting should not be induced in patients
that are depressed or have decreased conscious-
• See full-text articles as possible after ingestion of a ness or those that have seizures or are likely to
was alone in the house. Clawed plastic and CompendiumVet.com
toxic substance. Most decont-
amination methods practiced
seizure.2,3 Emetics should not be administered if
the patient has already vomited.2
COMPENDIUM 578 November 2008
crumbs were found at the scene.)
At the time, we found little informa- Drs. Luiz and Heseltine mentioned are rare and—when they do occur—
tion in the literature specifically on drug testing as a means of confirming carry a good prognosis. Nonetheless, we
cases of feline marijuana ingestion. To the diagnosis. We did not do this at the encourage colleagues treating known or
our knowledge (and anecdotally), mari- outset due to the client’s financial con- strongly suspected cases of marijuana
juana toxicity in cats is more likely to straints. When we undertook a detailed toxicity to submit samples for toxicol-
occur via inhalation when owners blow literature search and realized so little ogy screening and to share their data.
smoke in the cat’s face, rather than via was known about feline toxicity due to Drs. Anne Fawcett
dietary indiscretion, as is more com- Cannabis sativa, we offered to cover and Angela Phillips
mon in dogs. In this case, we did not the cost of toxicology testing. The own- Sydney Animal Hospitals Inner West
ascertain the ingested dose and did not ers allowed us to collect a urine sample Stanmore, NSW
know how long the patient would take from the patient via cystocentesis; how- Australia
to recover. ever, the sample, collected 14 days after
Hypothermia persisted for approxi- ingestion, returned a negative result.
mately 24 hours. One of the signs not THC may be detectable in human urine DO YOU HAVE
mentioned in the article by Drs. Luiz samples for 4 to 6 weeks, but the time
SOMETHING TO SAY?
and Heseltine was marked polyphagia. frame in which it remains detectable
During hospitalization, our patient ate in samples from companion animal Send your letters, suggestions,
ravenously. At one point, the patient species is not known, according to the comments, or questions to
defecated, passing a piece of a shoelace. pathologist at the laboratory to which E-MAIL editor@
This may have been ingested as a result we submitted the sample (Dr. Bruce CompendiumVet.com
of the cat’s marijuana-enhanced appetite Duff at Symbion Vetnostics). The recom- FAX 800-556-3288
before hospitalization, suggesting that mended time frame for submission of
WRITE Compendium,
gastrointestinal foreign bodies are a samples is within 48 hours of exposure
Veterinary Learning Systems
potential side effect of marijuana toxic- to the toxin.
780 Township Line Road,
ity (as is chocolate toxicity, if marijuana In this case, we are confident the
Yardley, PA 19067
is ingested in a brownie). The patient patient was suffering from marijuana
was discharged 3 days later when the toxicity. The negative urinalysis result More letters are online at
neurologic signs resolved, although the may be due to the fact that a young, CompendiumVet.com
owner reported that the cat had a “lazy lean cat can metabolize marijuana rela-
eye” for 2 weeks after discharge. tively rapidly. Fortunately, these cases
CompendiumVet.com | January 2009 | Compendium: Continuing Education for Veterinarians® 25](https://image.slidesharecdn.com/pv0109-091029165255-phpapp02/85/Pv0109-27-320.jpg)



![FREE
The Diagnostic Approach to FUO in Cats CE
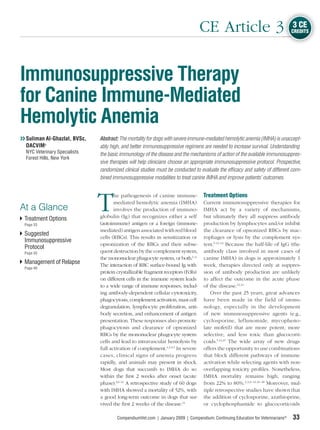
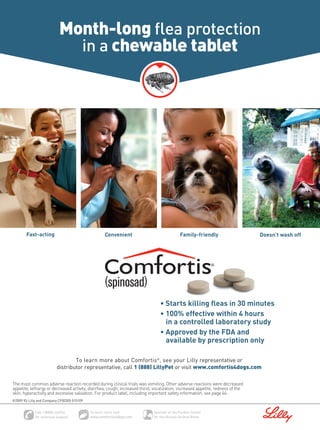
so testing for this disease may not be war- FIGURE 1
ranted.19 Serology for feline foamy virus (pre-
viously known as feline syncytium-forming
virus) can be conducted for cats with FUO
and suspected joint disease.20
Courtesy of Dr.Ty McSherry
Blood Cultures
Blood culture should be conducted for cats
with FUO and suspected bacteremia. Typical
signs of bacteremia in cats include anorexia,
pyrex ia, and shi f ti ng leg lameness. 21,22
Vegetative endocarditis is uncommon in cats, HISTOPLASMA ORGANISMS found in a pulmo-
but these animals typically have heart mur- nary fine-needle aspirate from a cat. The organisms
murs.21,22 Underlying predisposing causes for are located predominately in the macrophages.
which patients should be evaluated include
pyothorax, septic peritonitis, gastrointestinal are all associated with polyarthritis in cats.24–27
tract disease, pneumonia, endocarditis, pyelo- Other infective arthritides include fungal, rick-
nephritis, osteomyelitis, pyometra, and bite ettsial, and protozoal diseases.28
wounds.21 In a recent study,23 bacteremia was
diagnosed in 66 cats over a 9-year period. Immunodiagnostic Screening Panels
Immune panels (antinuclear antibody, rheuma-
Radiography toid factor [RF], Coombs) are thought to be unre-
Two-view abdominal and three-view thoracic warding in cats with FUO, but in a recent study, QuickNotes
radiographs should be obtained if the mini- 10 of 12 cats definitively diagnosed with rheu-
Urine culture should
mum database does not reveal the cause of matoid arthritis were strongly seropositive for
the FUO. Cats with lower respiratory disease RF.2,8,29,30 Therefore, although RF is not specific
be conducted for
are frequently asymptomatic, so care must be for rheumatoid arthritis, it may be an important every cat with fever
taken to rule out primary or secondary respi- diagnostic test in cats. The study also stated that of unknown origin
ratory problems. four cats diagnosed with periosteal proliferative regardless of the
polyarthritis were negative for RF.30 Antiplatelet appearance of the
Ultrasonography antibody tests and serum protein electrophore- urine sediment.
Abdominal ultrasonography can be valuable sis can be conducted if thrombocytopenia or
in detecting lesions not seen on radiographs. hyperglobulinemia, respectively, is present.
It can also assist with fine-needle aspiration
or biopsy if needed. Thoracic ultrasonogra- Other Diagnostic Testing
phy is not rewarding unless there are radio- Other diagnostic tests, such as cerebrospinal
graphic changes. fluid analysis and bronchoscopy with broncho-
alveolar lavage or transtracheal wash, should
Bone Marrow Evaluation
Bone marrow aspiration should be performed FIGURE 2
early in the evaluation of cats with FUO if
CBC abnormalities consistent with bone mar-
row disease are present (FIGURE 2). It should
be considered later if no definitive diagnosis
Courtesy of Dr. Robin Allison
has been made, even if the CBC is normal,
because neoplasia and infectious disease can
cause FUO in cats.2
Arthrocentesis
Arthrocentesis should be conducted on cats
even if there is no obvious evidence of joint dis-
ease. Calicivirus, mycoplasmosis, L-form bacte- HISTOPLASMA ORGANISMS in a bone marrow
rial infection, and FeLV with feline foamy virus aspirate from a cat.
CompendiumVet.com | January 2009 | Compendium: Continuing Education for Veterinarians® 29](https://image.slidesharecdn.com/pv0109-091029165255-phpapp02/85/Pv0109-31-320.jpg)

















This document provides information about an upcoming issue of the veterinary continuing education journal Compendium, including: - The cover article will discuss diagnostic approaches for fever of unknown origin. - Another article will focus on improving adherence to nutrition recommendations by understanding patient behavior assessments. - An advertisement approves a lymphocyte T-cell immunomodulator as a treatment aid for FeLV/FIV infections and associated symptoms.



































































