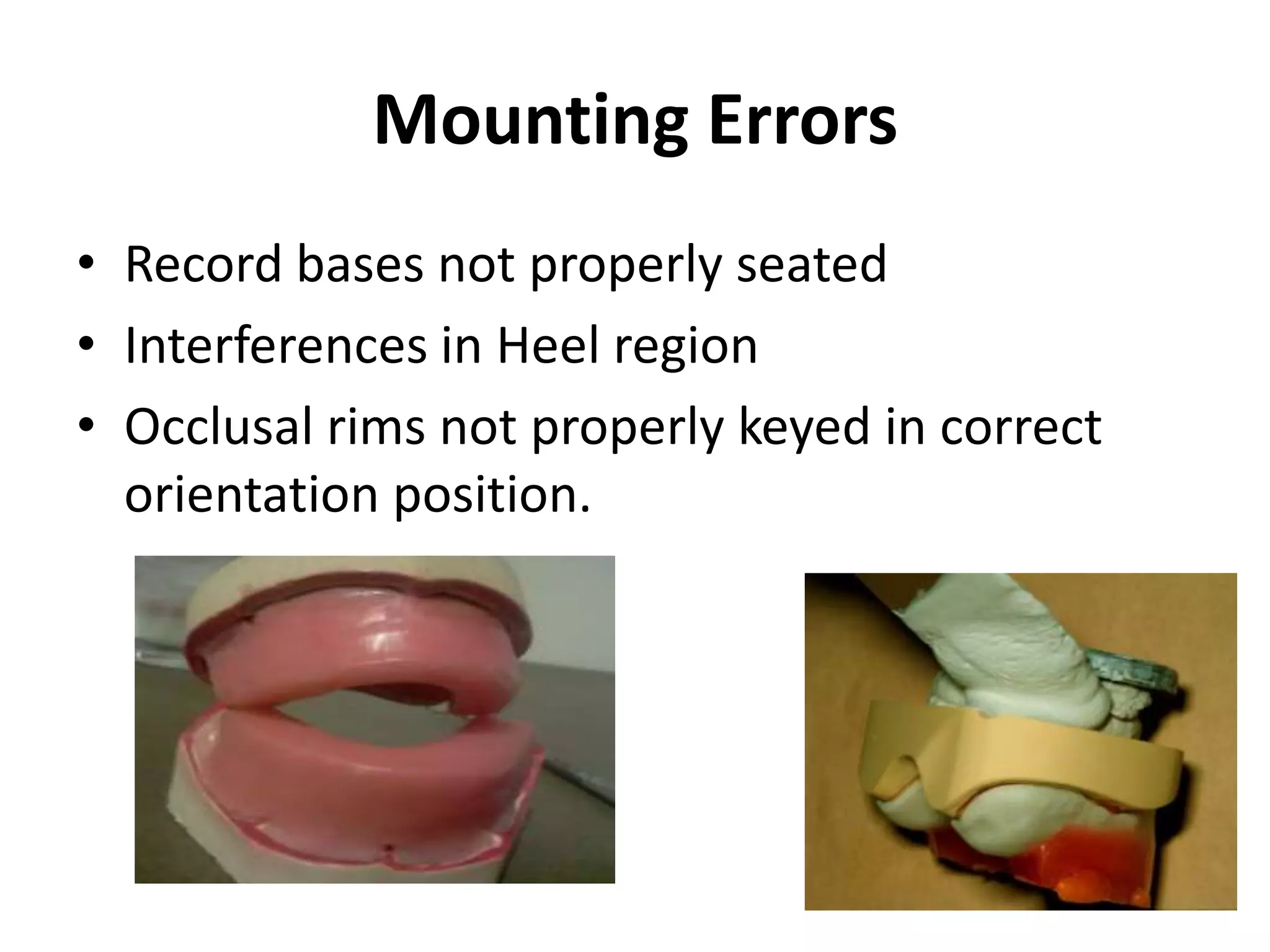
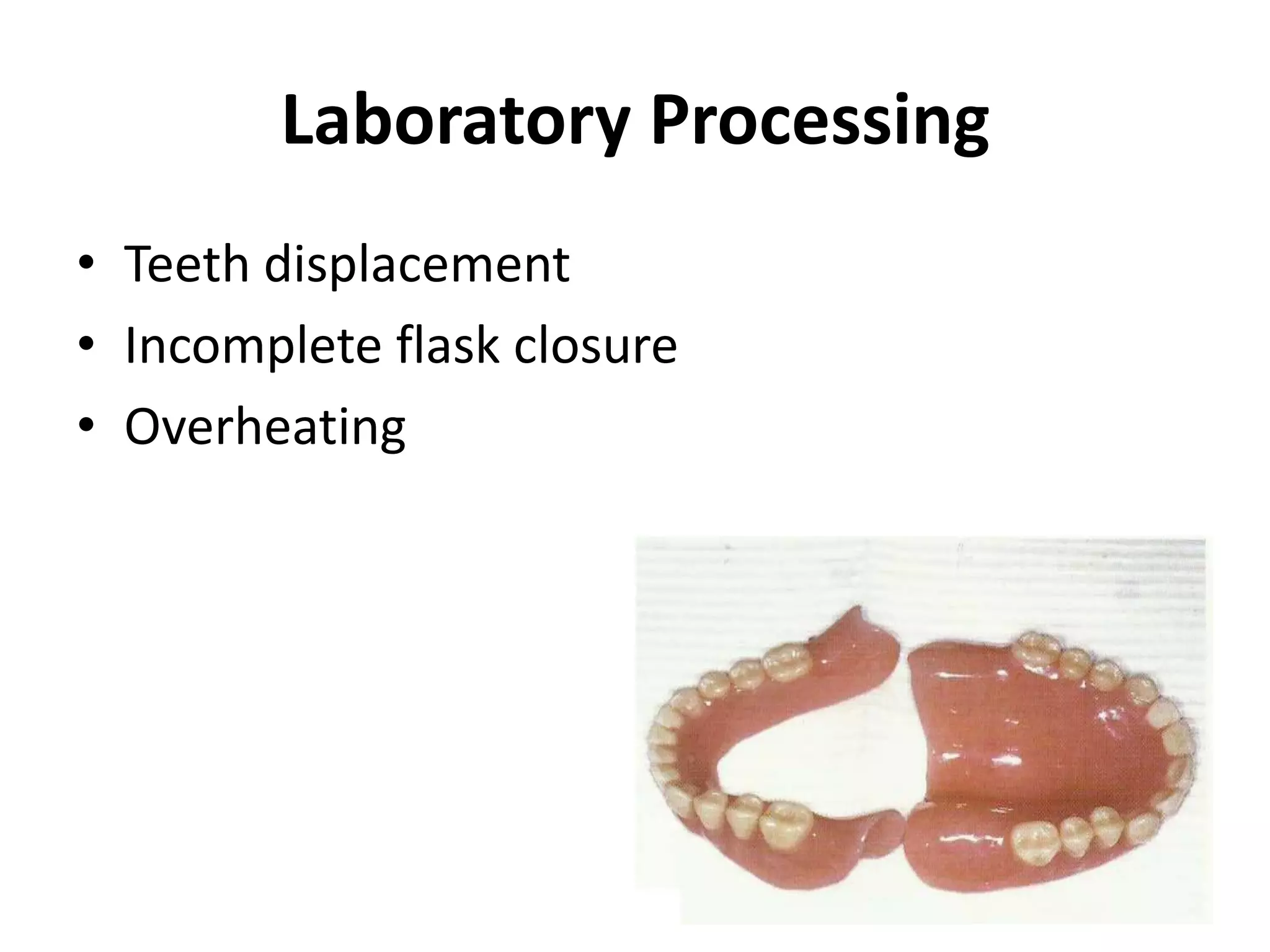
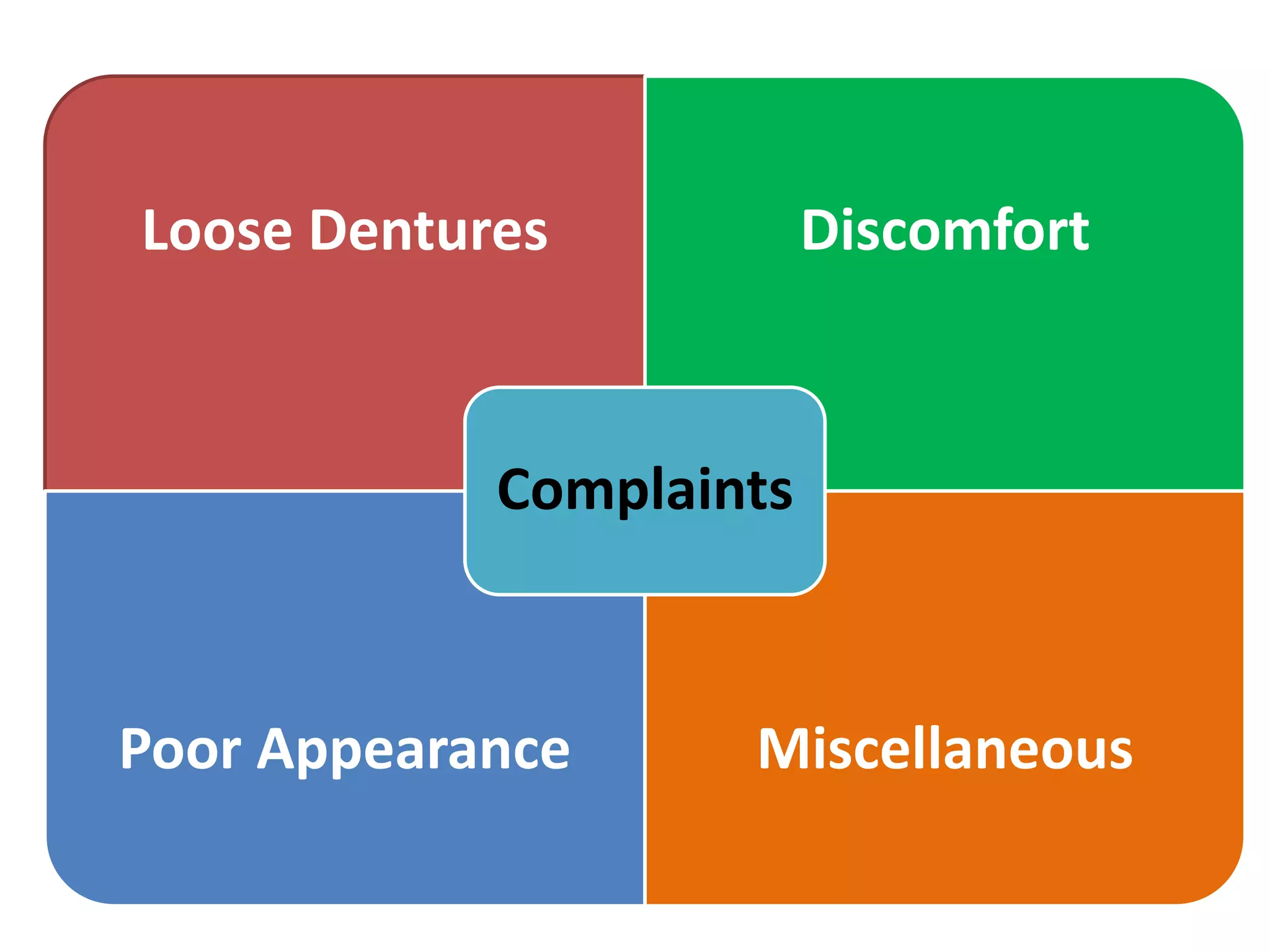
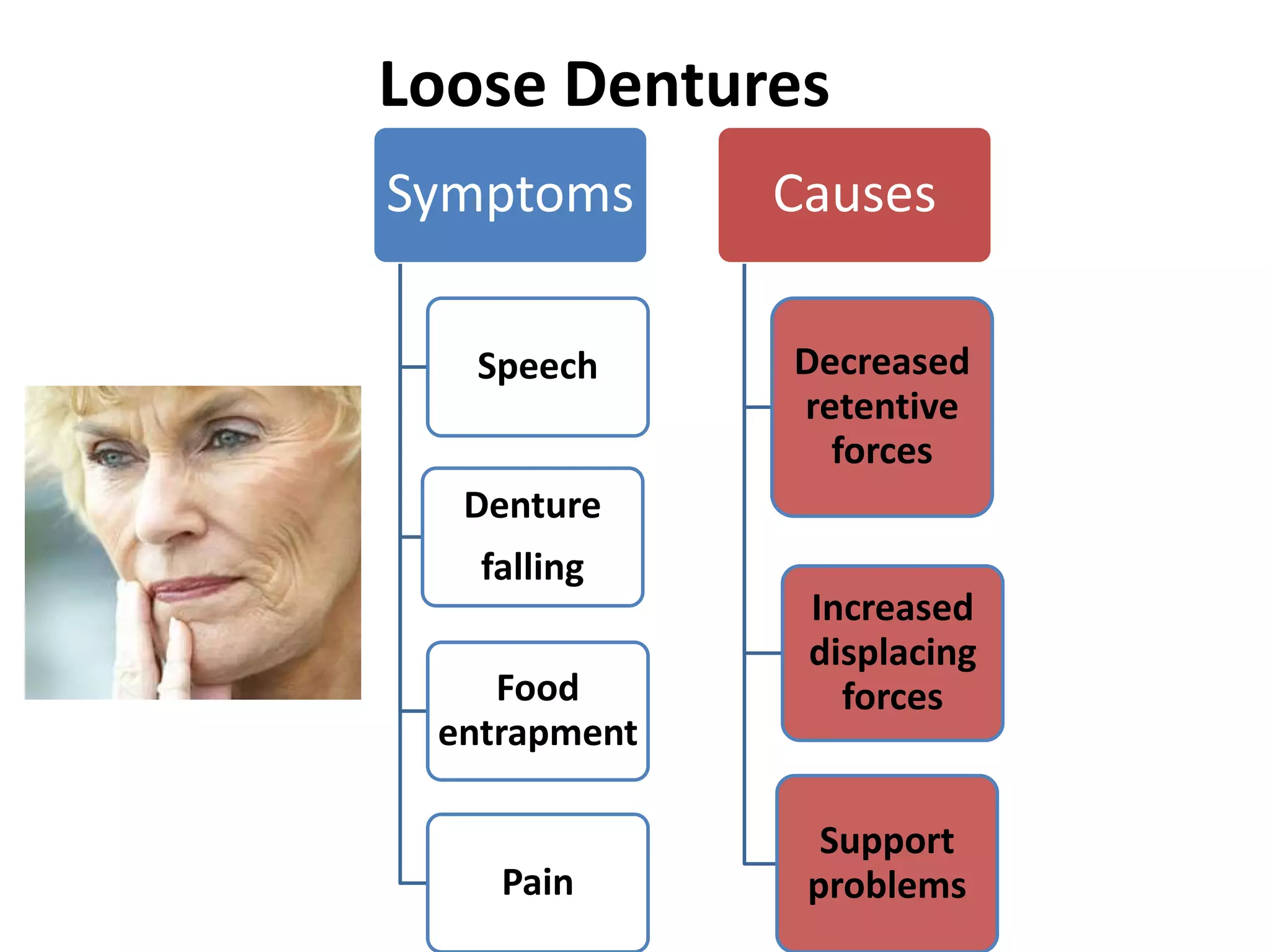
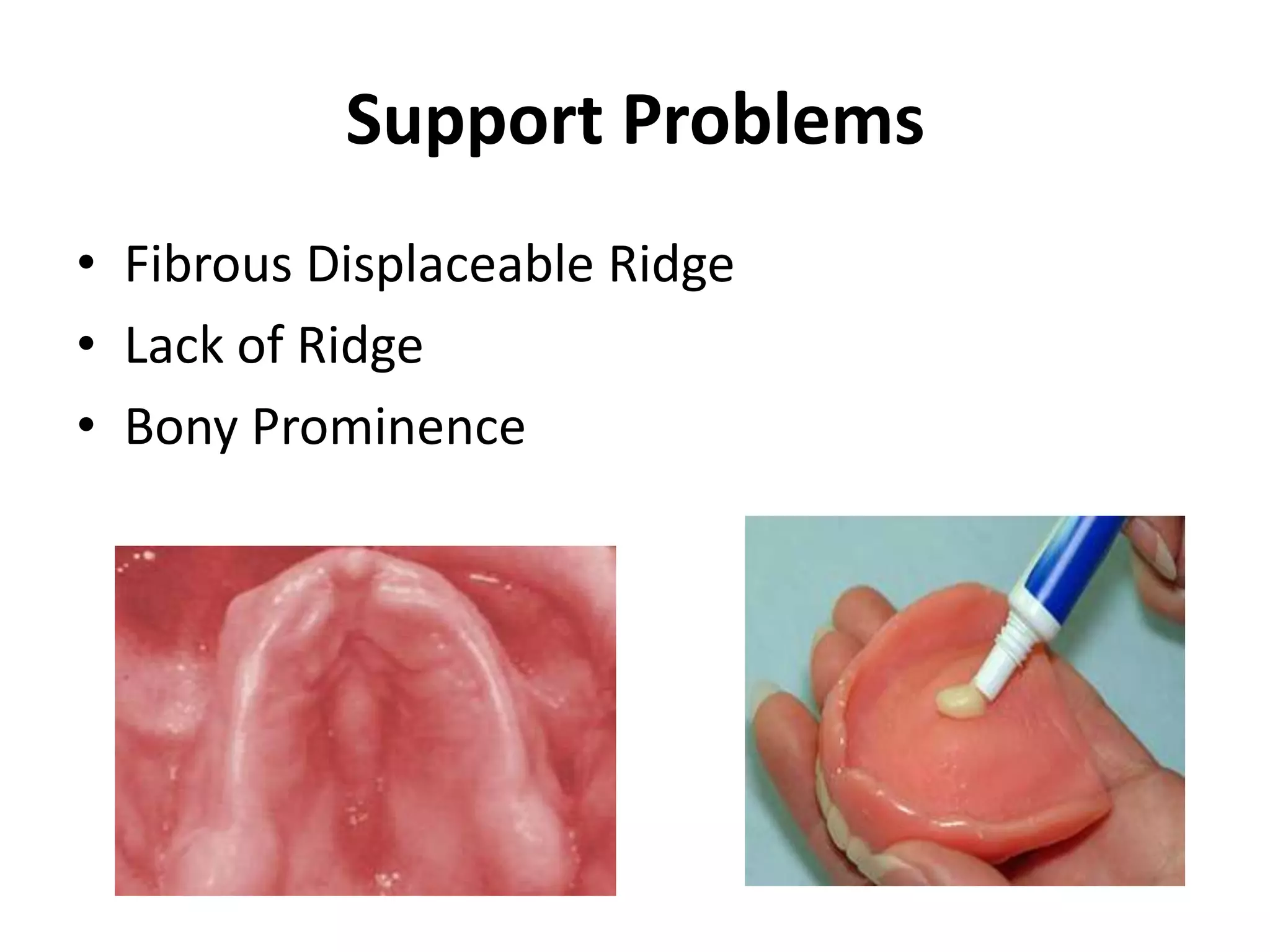
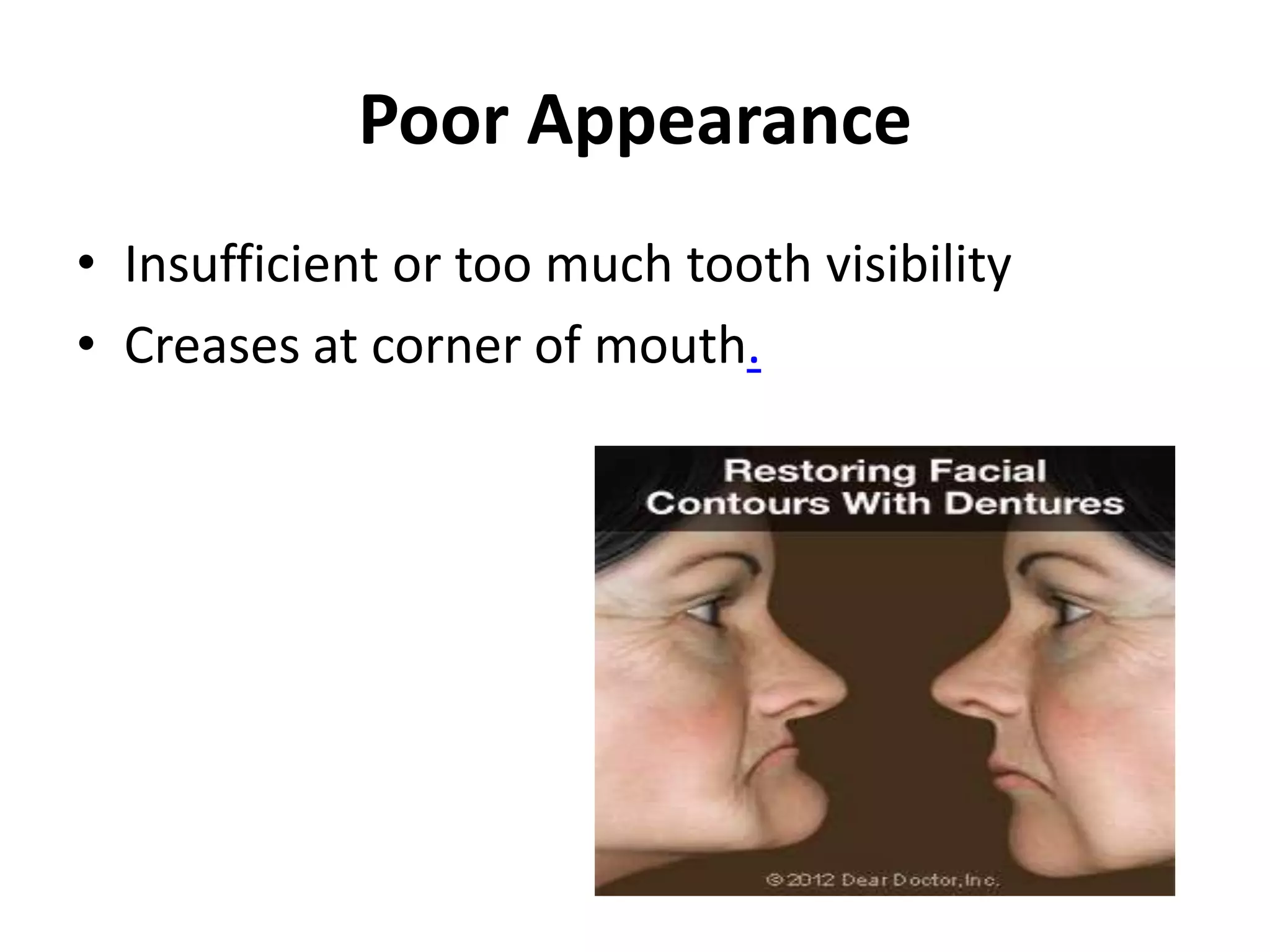
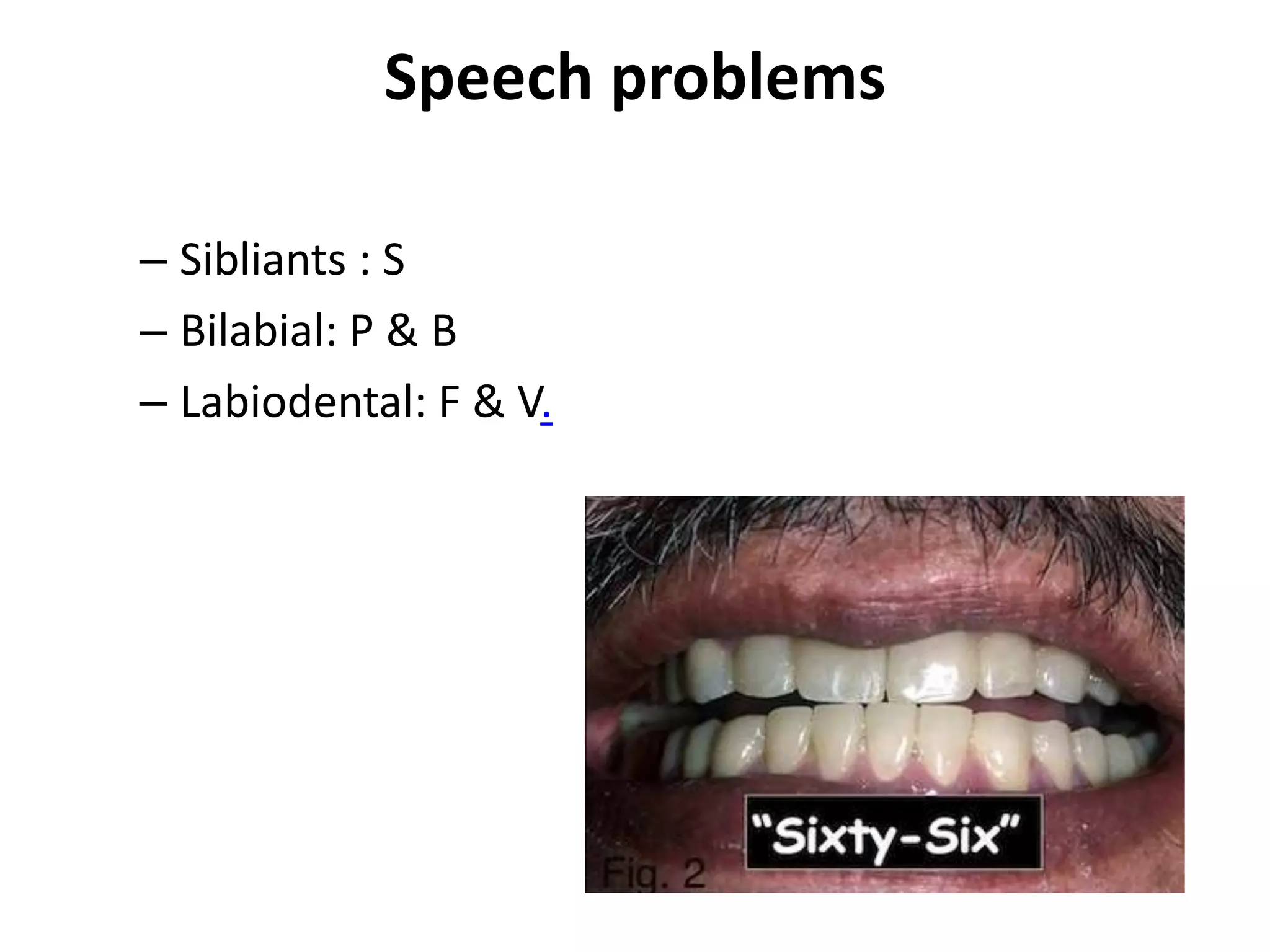
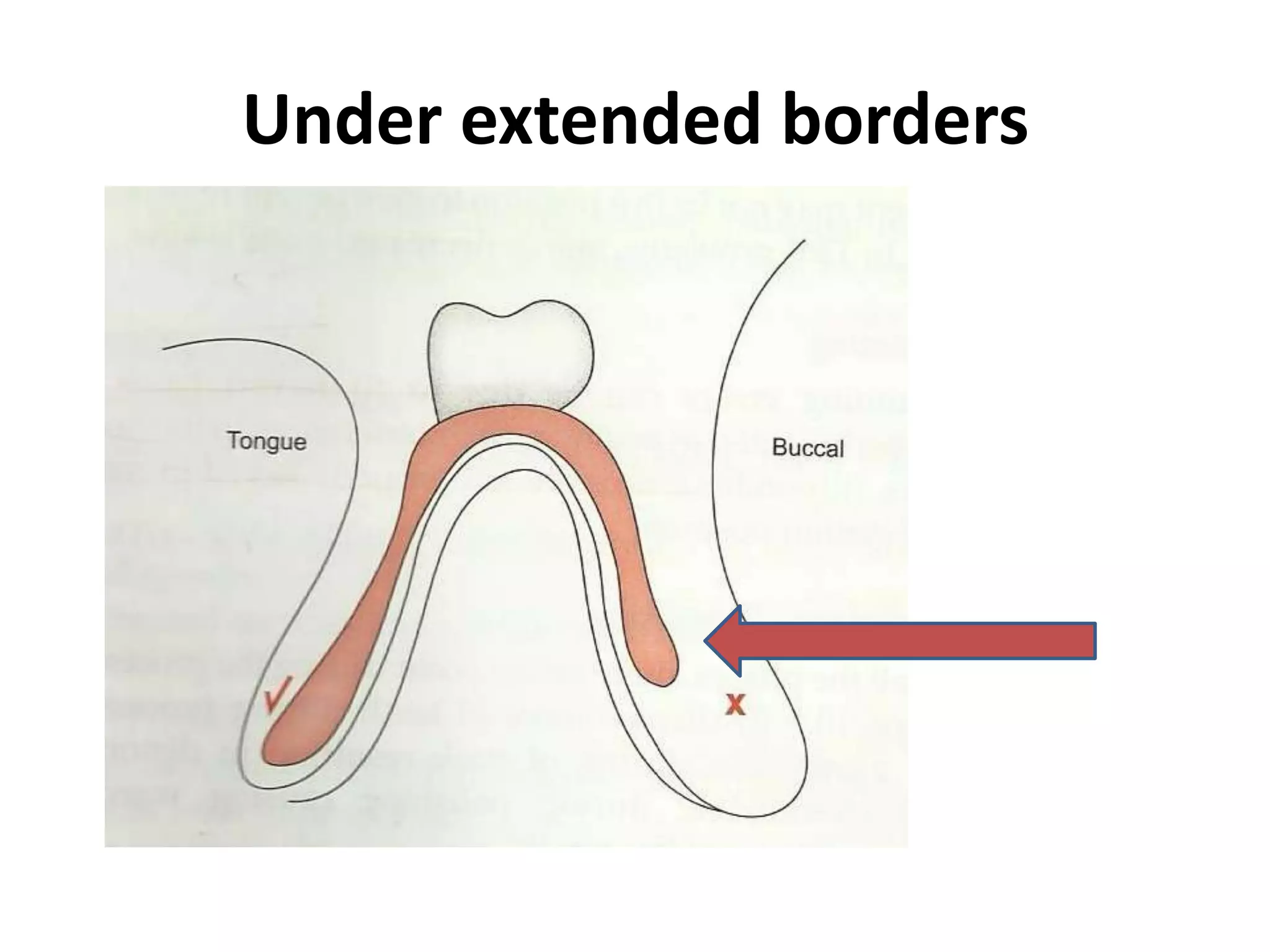
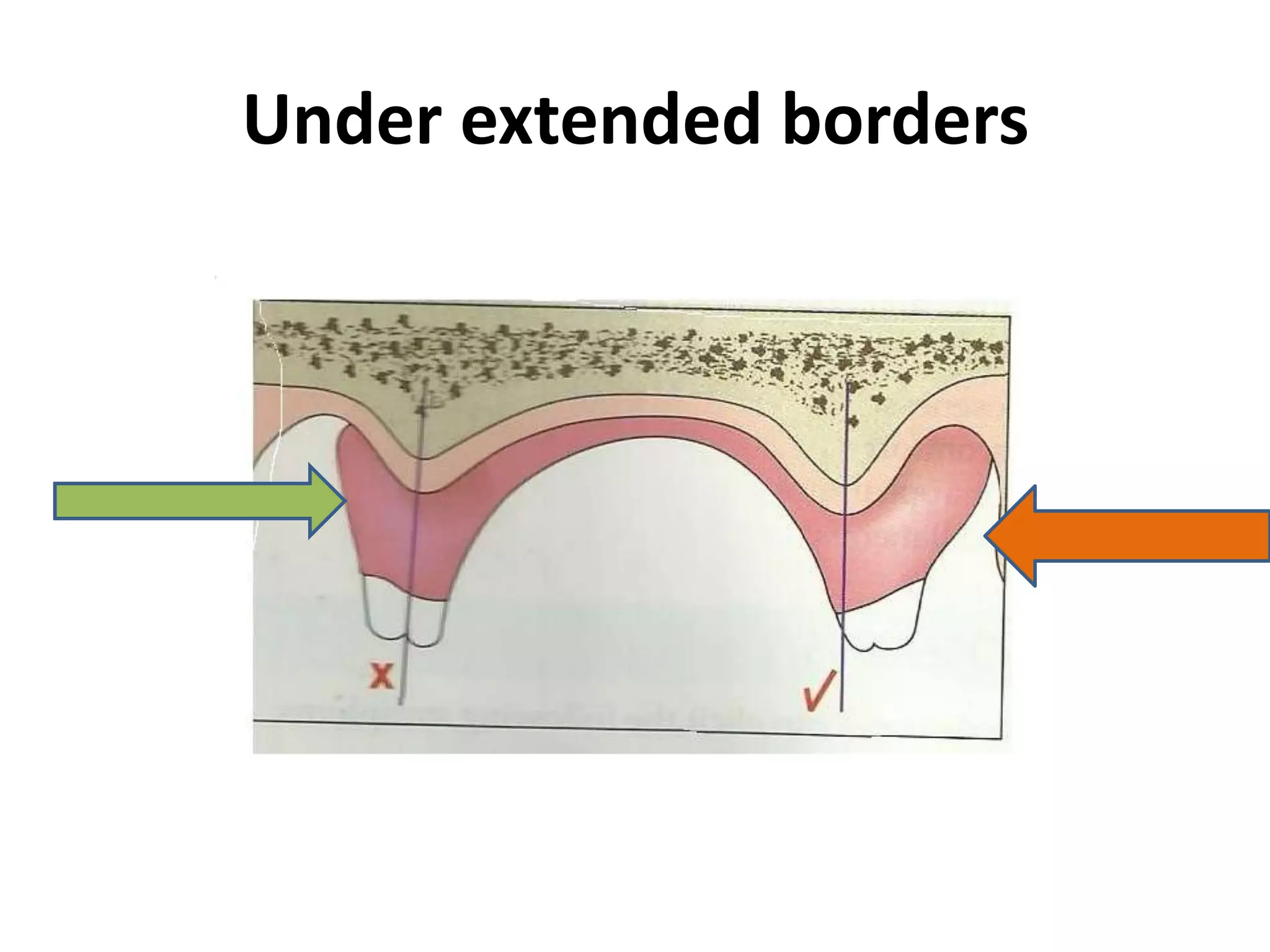
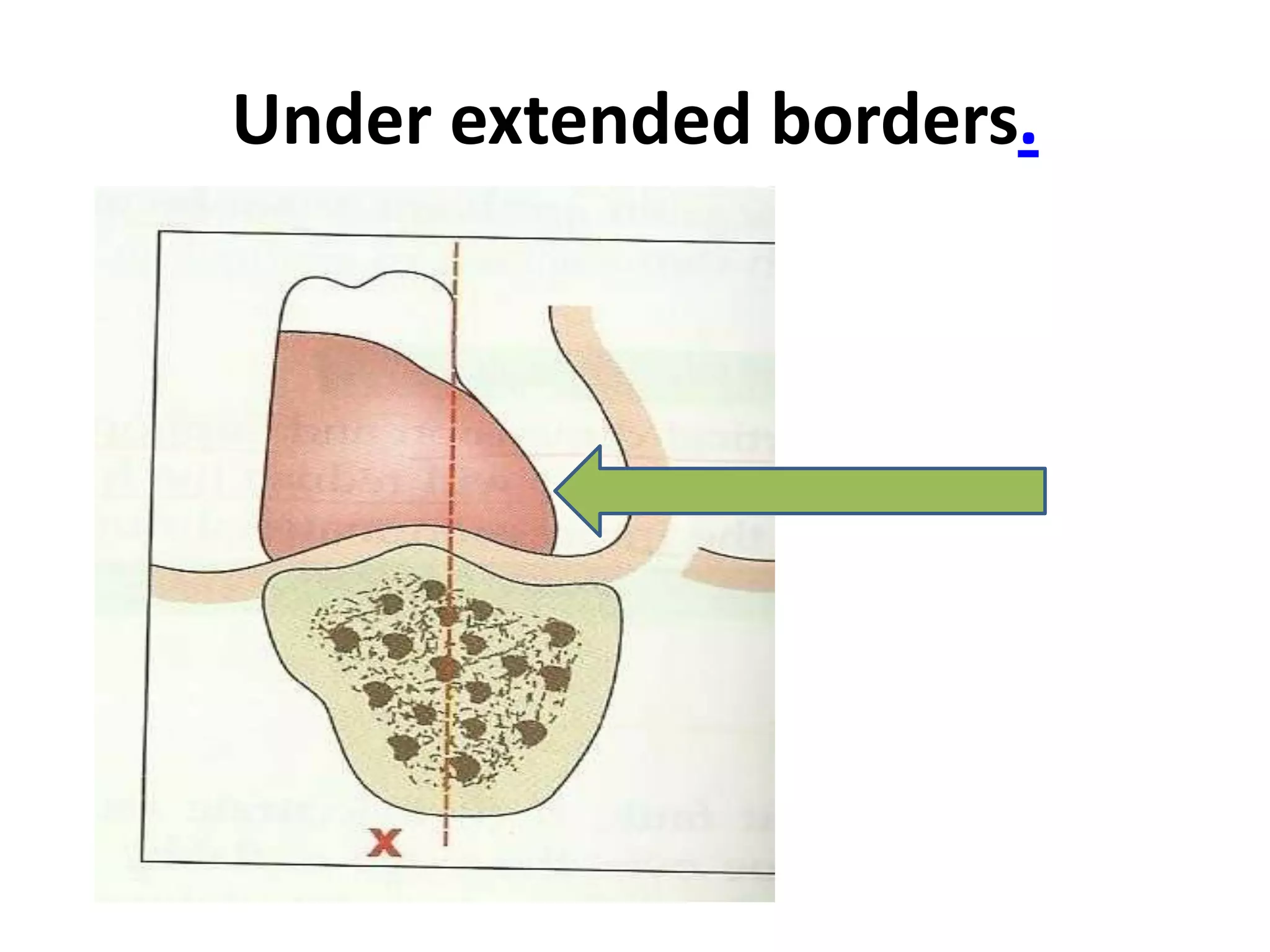
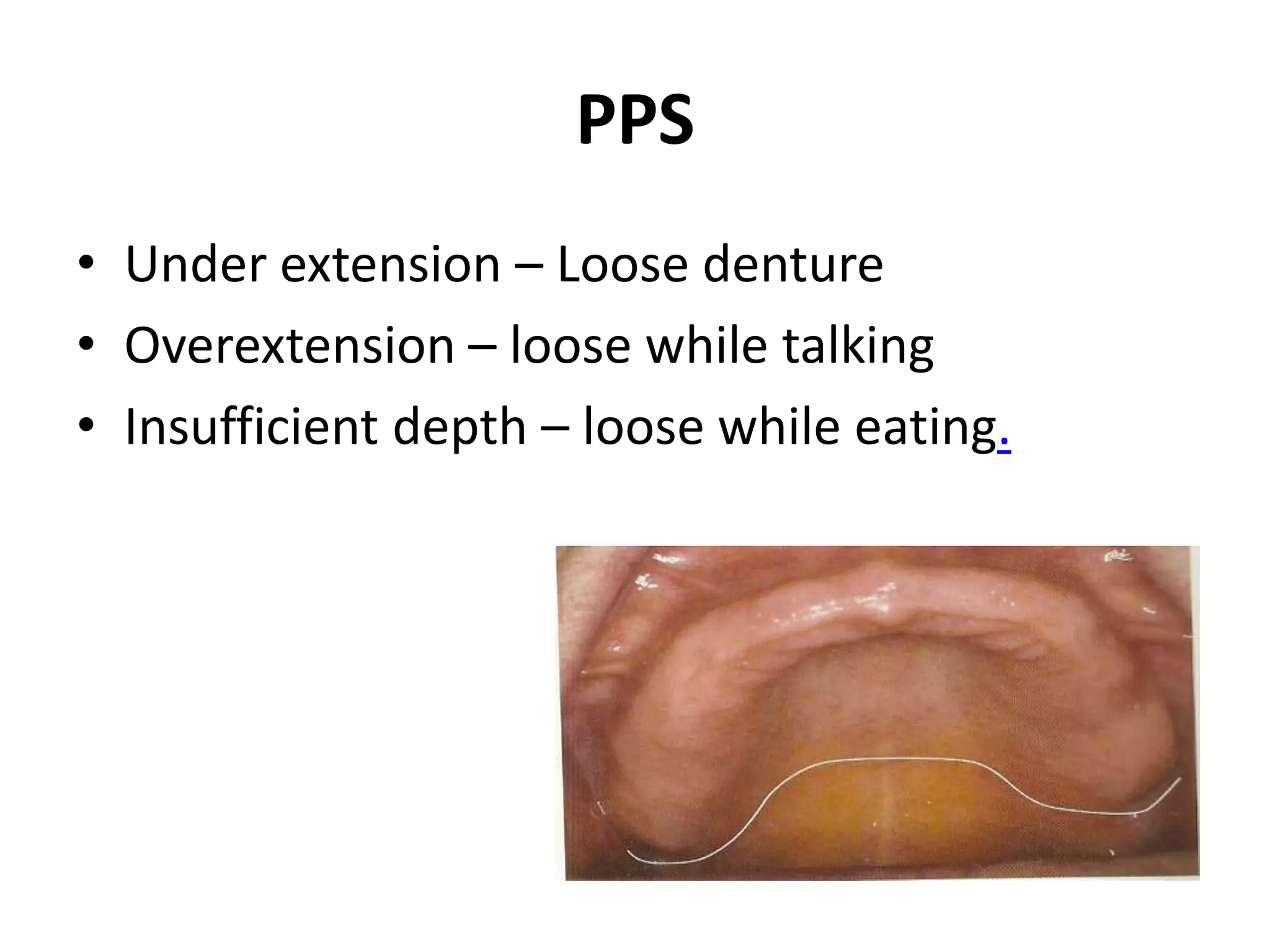
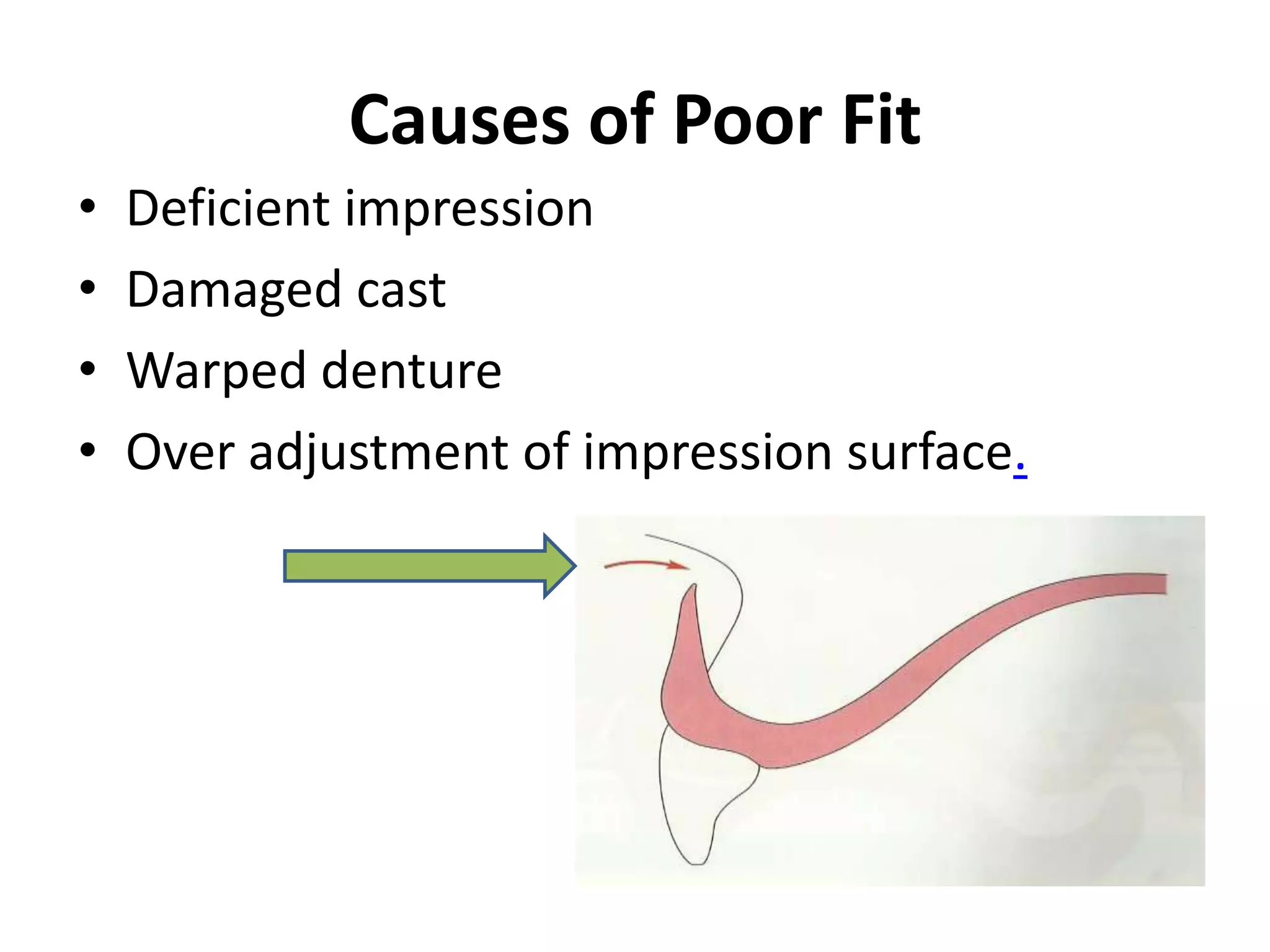
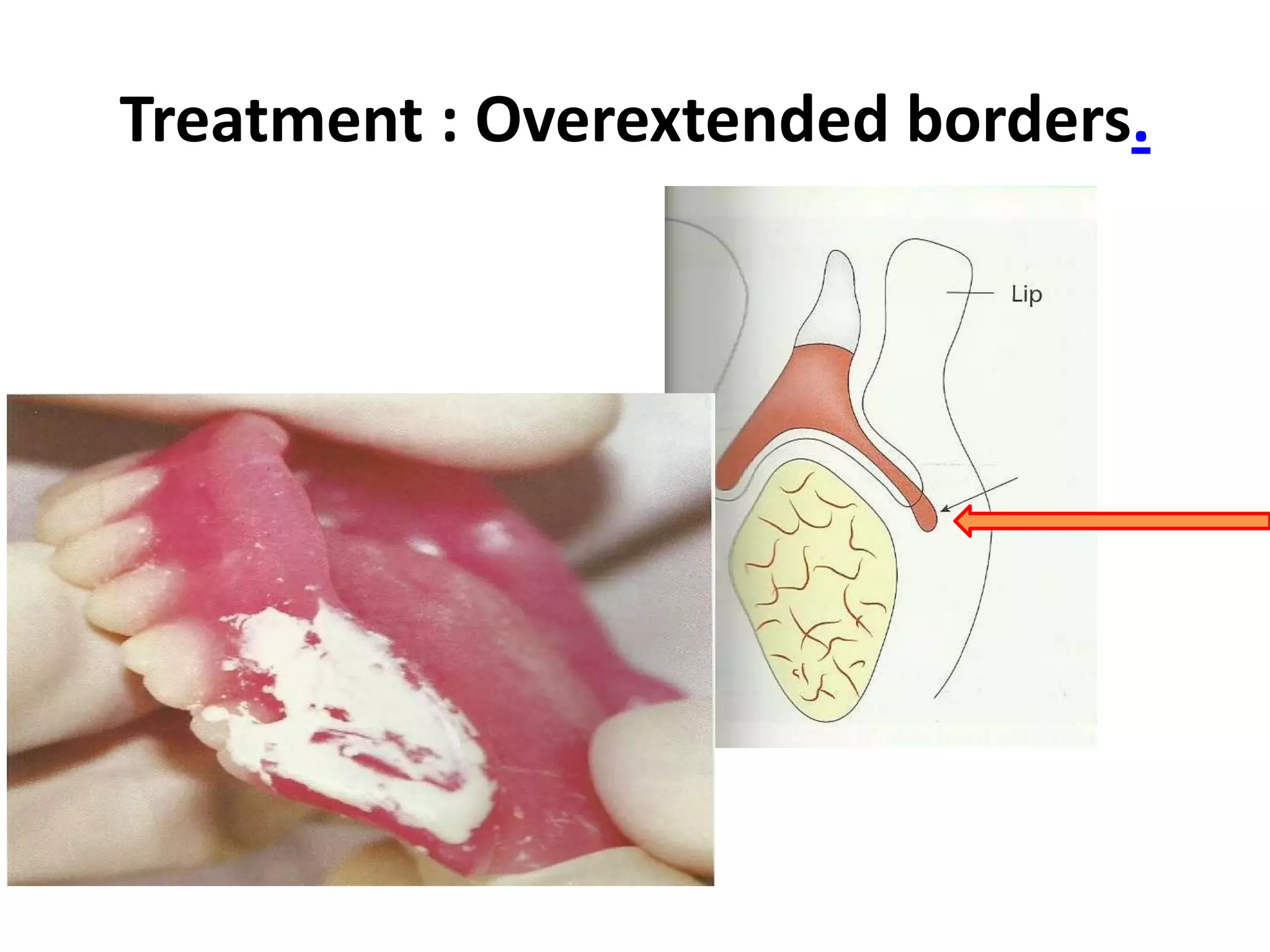
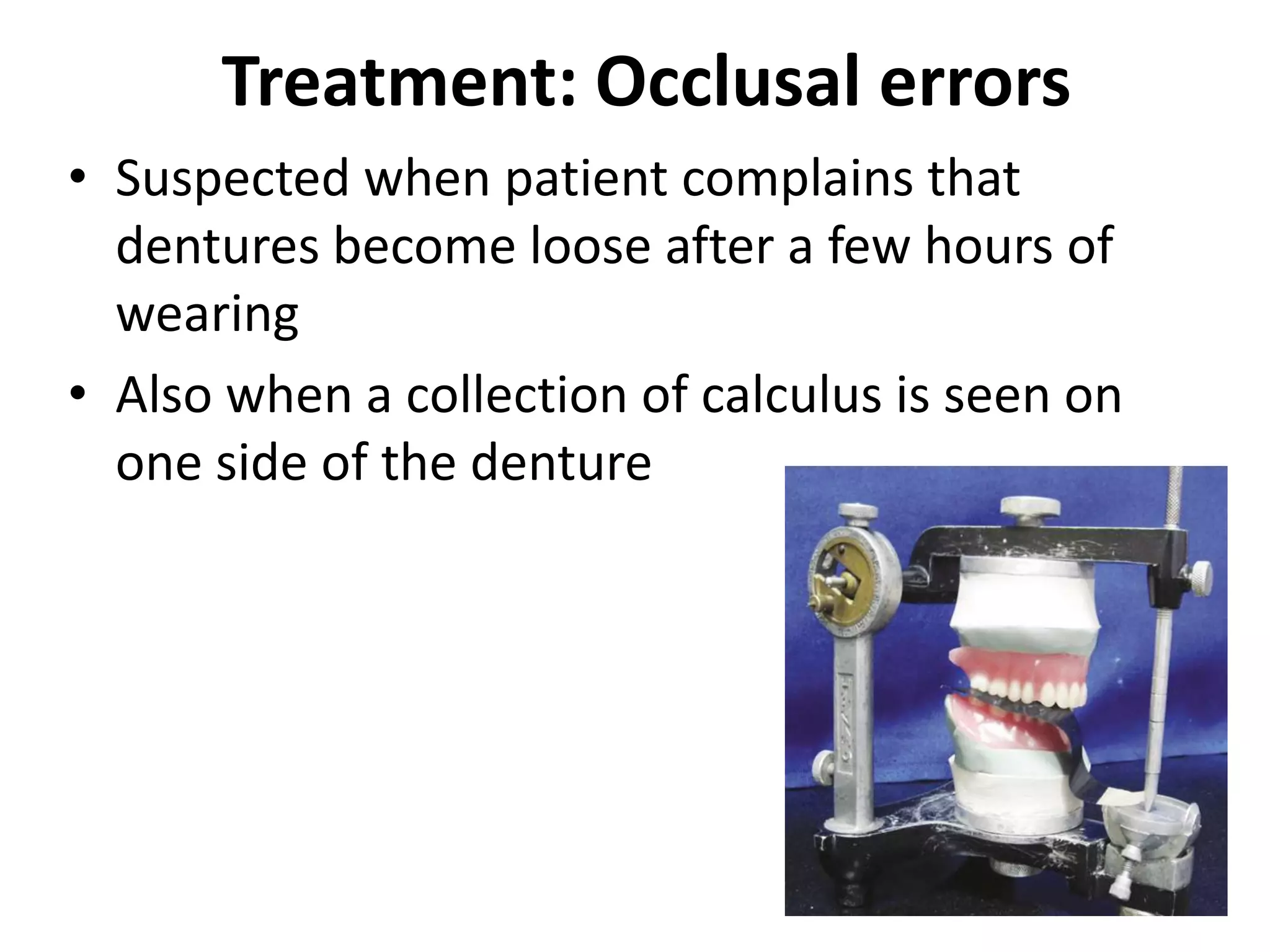
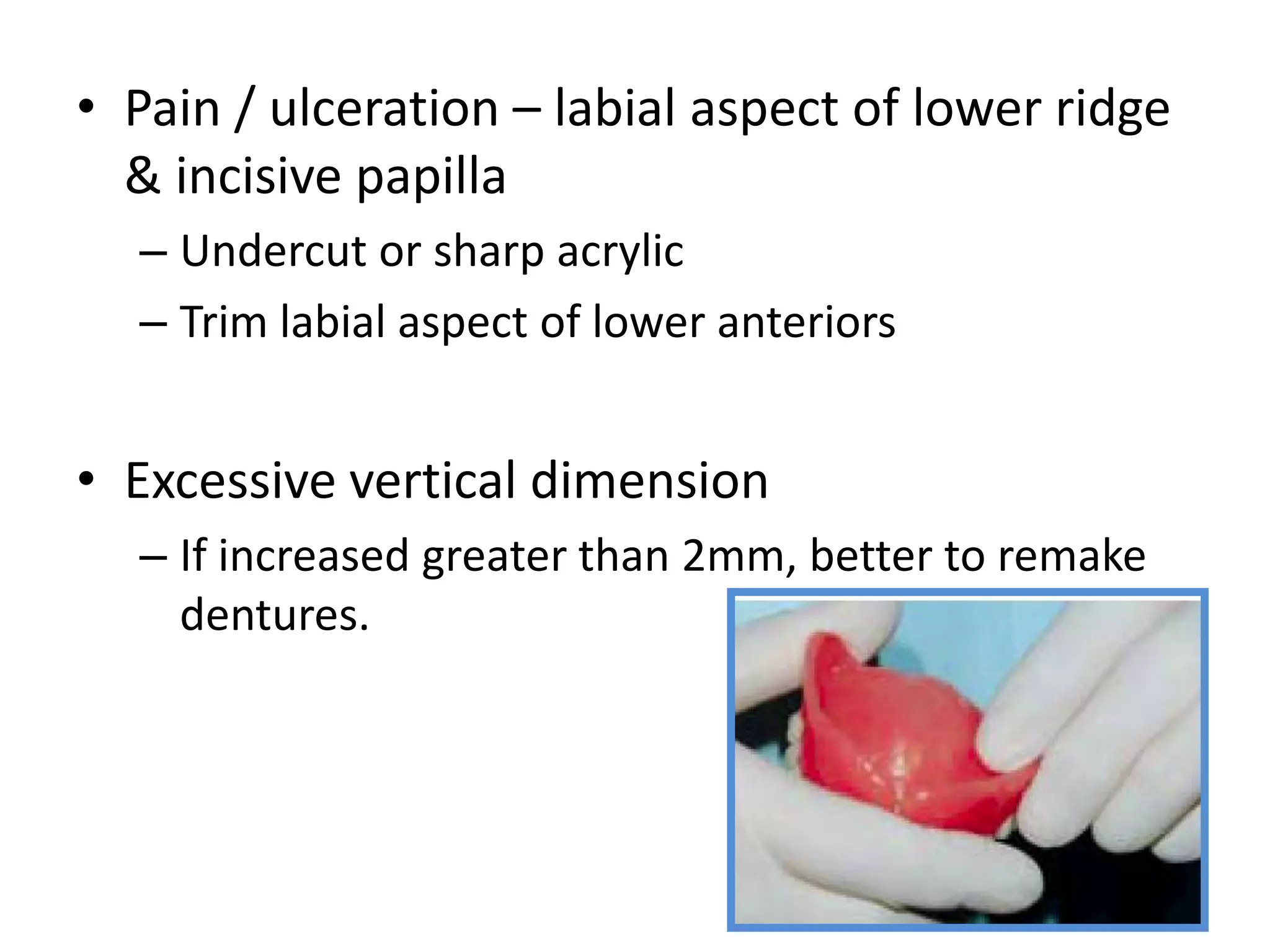
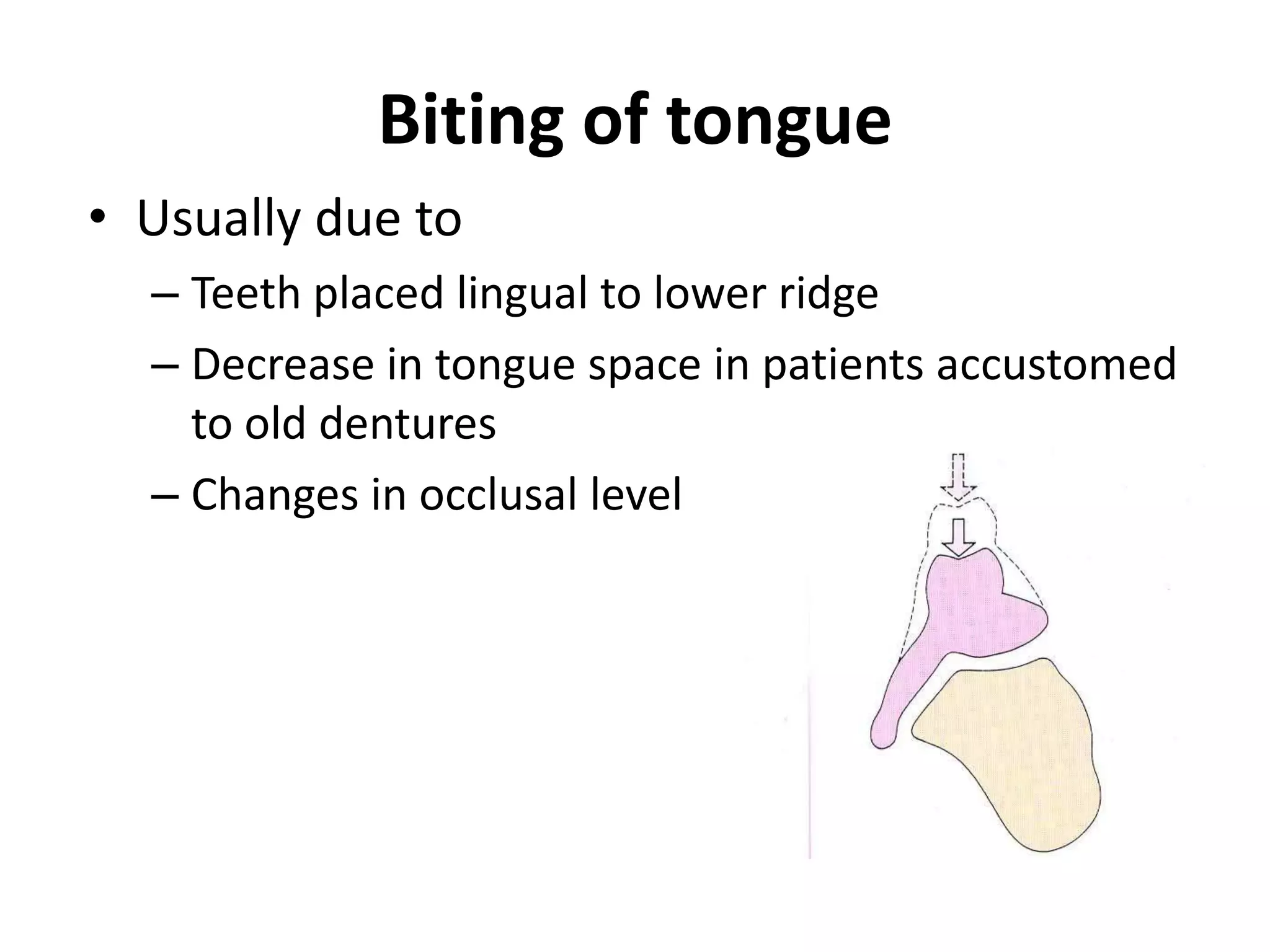
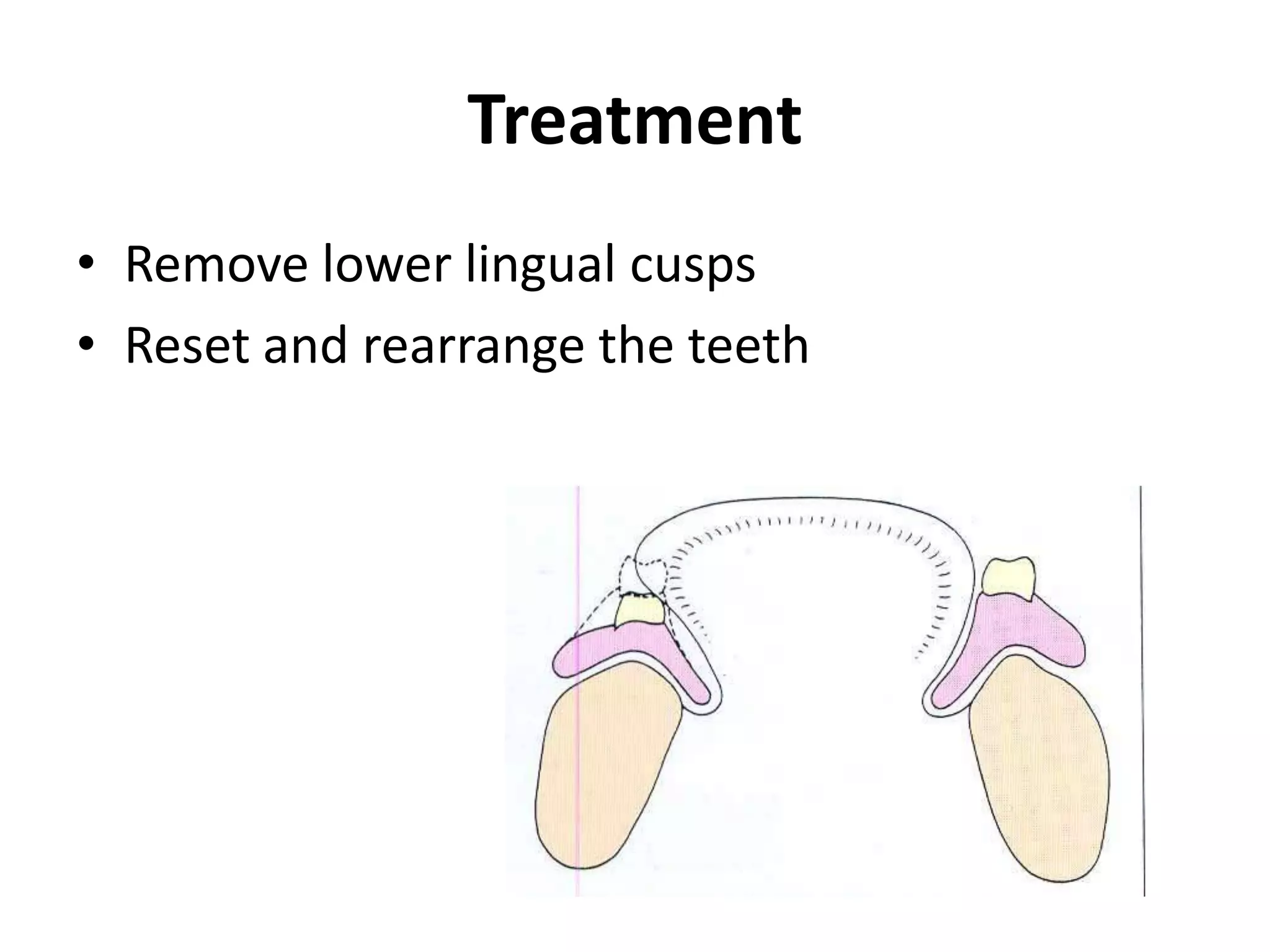
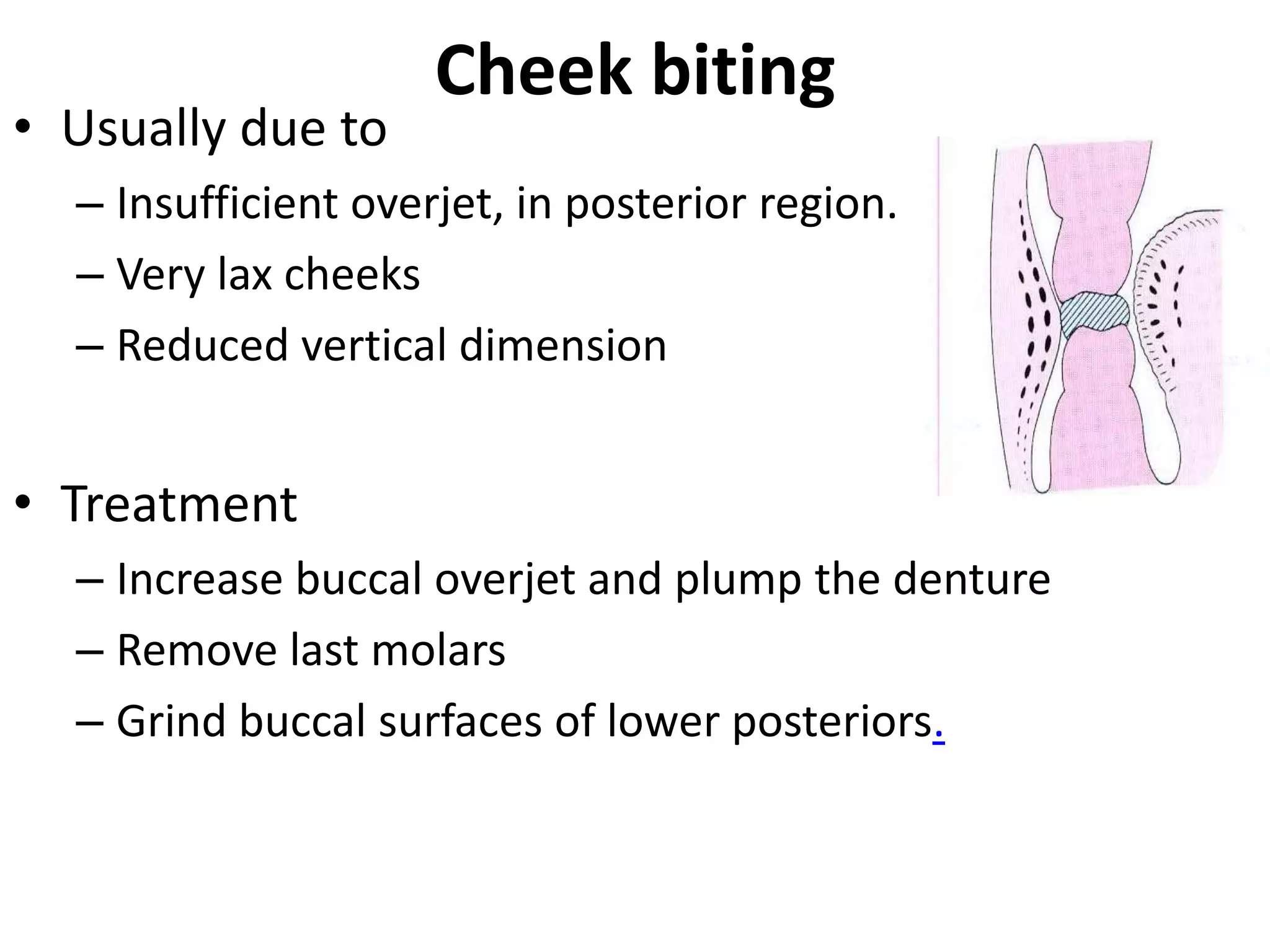
Post insertion problems in complete dentures can arise from inaccuracies during the denture construction process. Common complaints include loose dentures, discomfort, poor appearance, and speech problems. Loose dentures may be caused by decreased retention forces or increased displacing forces, and can be addressed by relining or remaking the dentures to improve the fit. Discomfort issues like pain can stem from occlusal errors or poor border extensions, and may be resolved through adjustments like selective grinding. Appearance complaints regarding tooth visibility or lip creasing could require remaking the dentures to correct.













































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)
















