Download to read offline

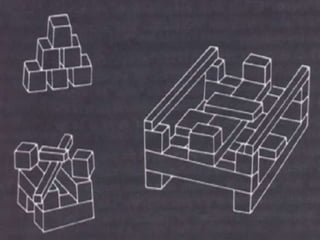
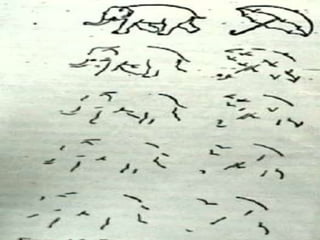
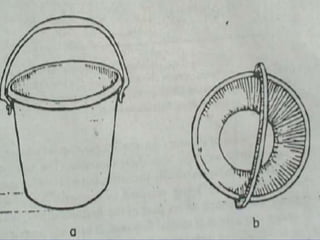
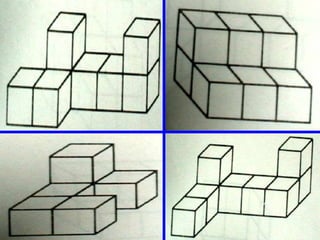
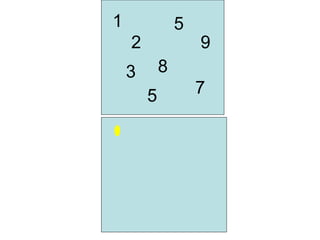
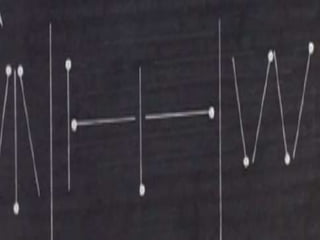
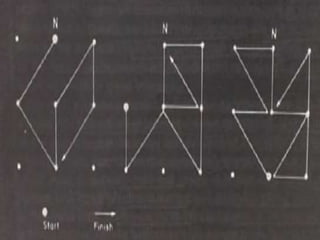
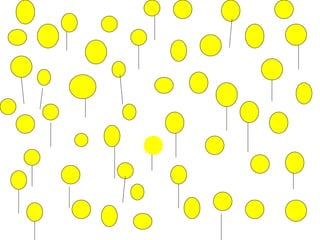
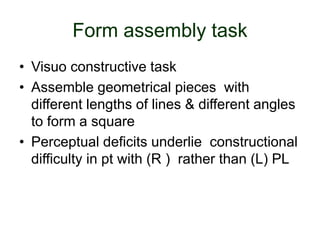
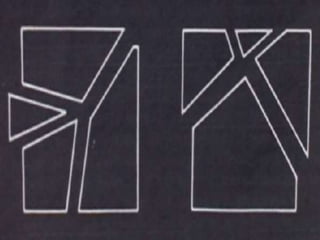

This document discusses tests and assessments used to evaluate functions of the parietal lobe, including: - Koh's block design task to evaluate constructional apraxia - Tests for visual object agnosia like the Gollin figures test - Assessments of symbolic synthesis like acalculia tests - Tests of complex spatial relations like the multiple choice Benton test - Route finding tasks like following maps between points on the floor - The interlocking finger test as a screening for parietal lobe dysfunction - Syndromes associated with parietal lesions are discussed, including Gerstmann syndrome and Balint syndrome.















































