Downloaded 40 times
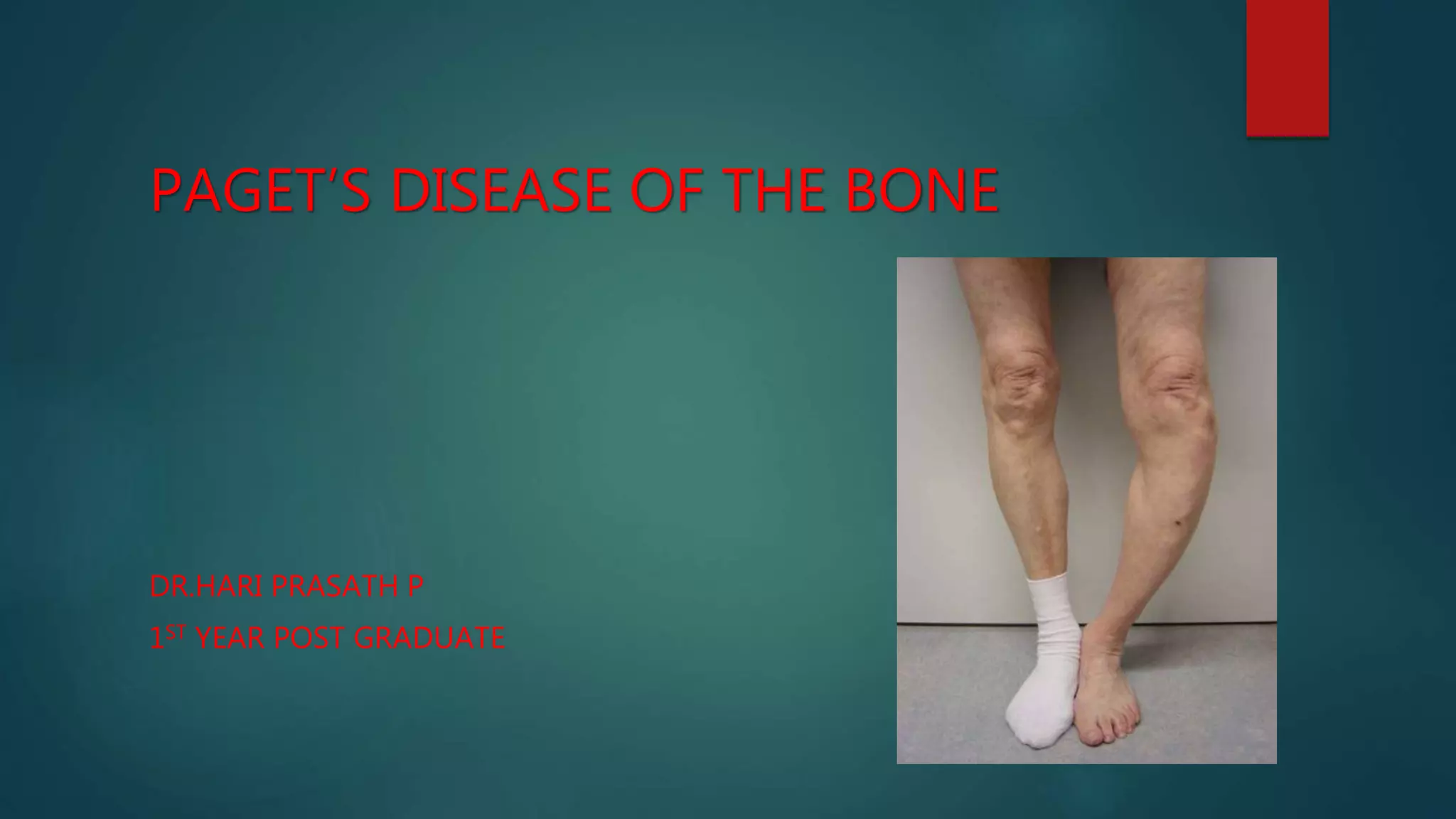


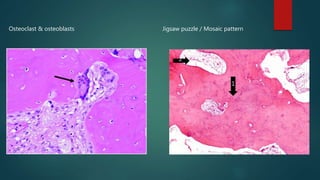

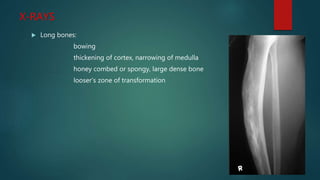

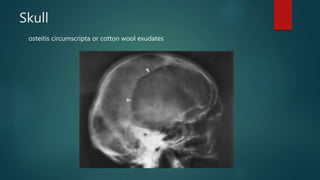

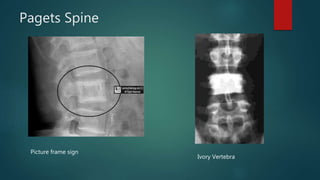
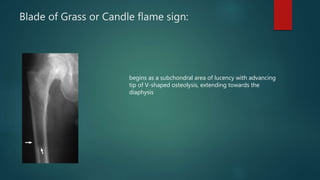

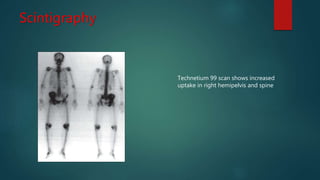





Paget's disease is a condition where there is excessive and disorganized bone remodeling, leading to thickened and deformed bones. It was first described in 1877 and typically involves the pelvis, femur, skull and spine. The cause is unknown but genetic and viral factors may play a role. It progresses through lytic, mixed, and sclerotic phases with abnormal osteoclast and osteoblast activity. Complications include fractures, arthritis, and neurological or vascular issues. Diagnosis involves elevated alkaline phosphatase and imaging showing thickened bones. Treatment focuses on suppressing active disease with bisphosphonates or calcitonin to reduce pain, deformity, and complications.

















































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
















![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)