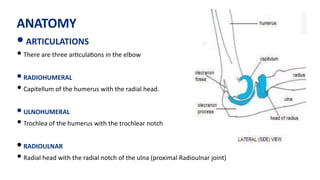
ANATOMY
• ARTICULATIONS
• Thereare three ar)cula)ons in the elbow
• RADIOHUMERAL
• Capitellum of the humerus with the radial head.
• ULNOHUMERAL
• Trochlea of the humerus with the trochlear notch
• RADIOULNAR
• Radial head with the radial notch of the ulna (proximal Radioulnar joint)
3.
MOVEMENTS
Flexion and Extensionat the elbow joint.
•Prona)on and Supina)on at superior radio-ulnar joint.
•Flexors Muscles :
•Brachialis
•Biceps
•Brachio-radialis
•Extensors Muscles :
•Triceps
•Anconeus
•
Pronator :
•Pronator teres
•Pronator quadratus
• Supinators :
•Biceps
•Supinator.
4.
LIGAMENTS
• Elbow stabilityis provided by the soJ )ssue structures surrounding the joint as well as by
bony ar)cula)ons.
• The soJ )ssue restraints can be divided into both sta)c and dynamic stabilizers.
• The sta)c stabilizers
• Joint capsule
• the LCLs and MCLs.
•
5.
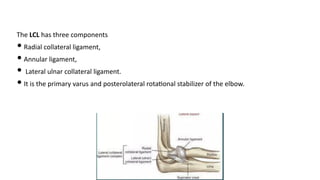
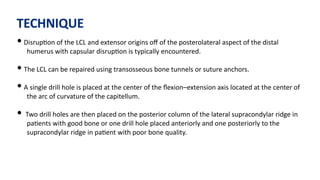
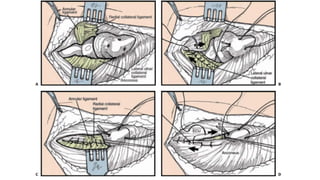
The LCL hasthree components
• Radial collateral ligament,
• Annular ligament,
• Lateral ulnar collateral ligament.
• It is the primary varus and posterolateral rota)onal stabilizer of the elbow.
6.
• The radialhead is surrounded by the annular ligament which aQaches to the anterior and
posterior margins of the radial notch of the proximal ulna.
• The radial collateral ligament arises from the lateral epicondyle and blends with the annular
ligament.
• The lateral ulnar collateral ligament is posterior to the radial collateral ligament and aQaches
to the crista supinatoris of the proximal ulna, just distal to the annular ligament.
7.
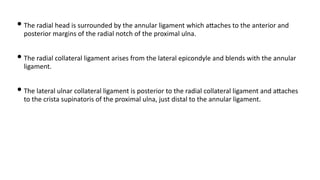
• The MEDIALCOLLATERAL LIGAMENT consists of the anterior and posterior bundles.
• The anterior bundle is the key valgus stabilizer of the elbow, arising from the anteriorinferior
aspect of the medial epicondyle to insert on the sublime tubercle of the proximal ulna.
• The posterior bundle provides a secondary restraint to valgus load and also resists ulnar
rota)on.
8.
• The dynamicrestraints include the biceps, brachialis, and triceps which provide compressive
stability to the elbow due to their joint reac)ve forces and are par)cularly important when
the sta)c stabilizers have been injured.
• The common extensor muscles provide varus stability and the common flexor muscles
provide valgus stability.
• Prona)on will stabilize the LCL-deficient elbow while supina)on decreases stability in this
seUng.
9.
• Pa)ents withsimple elbow disloca)ons rou)nely have disrup)on of both the MCL and LCL
and the elbow capsule.
• The muscular origins may be disrupted as well; typically the injury to the lateral common
extensor origin is more extensive than the medial common flexor origin.
• The radial head may cause impression fracture of the posterior capitellum which can
contribute to recurrent instability.
10.
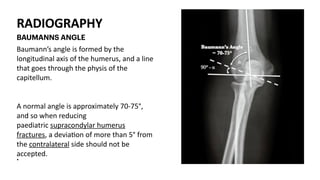
RADIOGRAPHY
Baumann’s angle isformed by the
longitudinal axis of the humerus, and a line
that goes through the physis of the
capitellum.
A normal angle is approximately 70-75°,
and so when reducing
paediatric supracondylar humerus
fractures, a devia)on of more than 5° from
the contralateral side should not be
accepted.
•
BAUMANNS ANGLE
11.
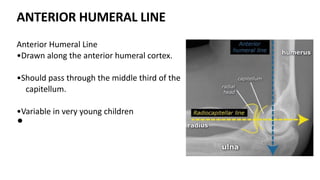
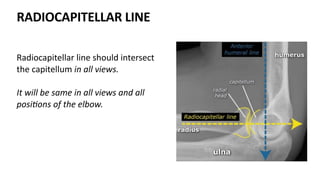
ANTERIOR HUMERAL LINE
AnteriorHumeral Line
•Drawn along the anterior humeral cortex.
•Should pass through the middle third of the
capitellum.
•Variable in very young children
•
INTRODUCTION
• A simpleelbow disloca)on is one in which there are no associated fractures.
• The elbow joint is the second most commonly dislocated joint in the adult popula)on.
• Adolescent males are the highest-risk group.
14.
MECHANISMOFINJURY
• Most common- Fall of outstretched hand.
• posterolateral dislocaGon - Valgus, axial, and posterolateral force .
• Less commonly - varus, axial, and posteromedial force where the injury proceeds from
medial to lateral, but this mechanism typically results in a small anteromedial coronoid
fracture
15.
ASSOCIATED INJURIES
• Disrup)onof the collateral ligaments,
• elbow capsule,
• forearm flexor
• extensor muscle origins.
• Rarely brachial artery injury .
• The ulnar nerve is the most commonly injured nerve following elbow disloca)on, but median
nerve is entrapped in the joint aJer reduc)on.
16.
SIGNS AND SYMPTOMS
•Pain
•Swelling
•Ecchymosis
In many cases
•Instability
•Crepita)on
•Deformity
17.
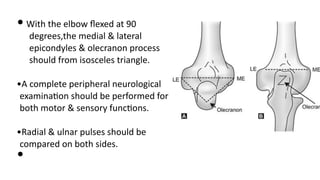
• With theelbow flexed at 90
degrees,the medial & lateral
epicondyles & olecranon process
should from isosceles triangle.
•A complete peripheral neurological
examina)on should be performed for
both motor & sensory func)ons.
•Radial & ulnar pulses should be
compared on both sides.
•
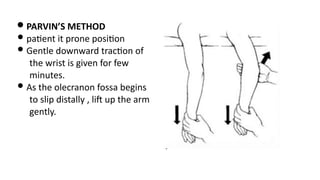
• PARVIN’S METHOD
•pa)ent it prone posi)on
• Gentle downward trac)on of
the wrist is given for few
minutes.
• As the olecranon fossa begins
to slip distally , liJ up the arm
gently.
22.
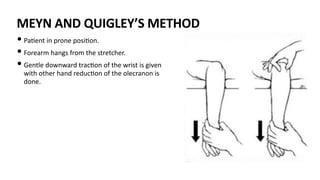
MEYN AND QUIGLEY’SMETHOD
• Pa)ent in prone posi)on.
• Forearm hangs from the stretcher.
• Gentle downward trac)on of the wrist is given
with other hand reduc)on of the olecranon is
done.
23.
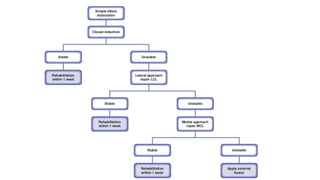
• Acute simpledisloca)on should undergo Closed Reduc)on with
pa)ent under seda)on with appropriate relaxa)on and monitoring
of vitals.
•The medial and lateral epicondyles are palpated and their
rela)onship to the olecranon is determined in order to first correct
and medial/lateral displacement in the coronal plane.
•Elbow flexed to 30 degrees and trac)on is placed through forearm
while stabilizing the humerus.
24.
• Direct pressureover olecranon may glide over distal humerus into
joint , supina)on of forearm is helpful for reduc)on.
•AJer reduc)on, the elbow is taken through an arc of flexion–
extension in prona)on, neutral, and supina)on in order to evaluate
for residual instability.
•Splint at 90 flexion for 1 week but not more than 3 week.
•
25.
• If theelbow redislocates when flexed to less than 30 degrees,
opera)ve treatment should be considered.
•Most pa)ents will have varus–valgus instability, but this plane of
instability alone is not an indicaGon for operaGve treatment.
26.
• Radiographs areperformed to ensure reduc)on has been achieved
and to evaluate for the presence of fractures not visualized on the
prereduc)on radiographs.
•The pa)ent is seen within a week to ensure maintenance of the
reduc)on and to begin ac)ve range of mo)on of the elbow.
27.
• AJer 1week the splint is removed. The pa)ent is examined for stability again and
asked to ac)vely extend and flex the elbow. Pa)ents will typically move only
within their stable arc and are unlikely to redislocate if they had a stable
reduc)on.
• The pa)ent is seen weekly for the first 3 weeks to decrease the extension block by
10 degrees per week. Radiographs are performed to confirm concentric
reduc)on at each visit.
• The pa)ent is then seen again at 6 weeks and may resume most normal ac)vi)es
and start a light strengthening program, avoiding varus or valgus loading un)l 12
weeks.
28.
• Immobiliza)on greaterthan 3 weeks should be avoided as this has been
demonstrated to cause an increased incidence of s)ffness and poorer func)onal
outcomes.
29.
STABILITY
ANTERIOR-POSTERIOR
Trochlea-olecranon fossa(extension),coronoid fossa,radiocapitellarjoint, biceps-
triceps-brachialis (flexion)
•VALGUS
The medial collateral ligament complex:
the anterior bundle is primary stabilizer in flexion & extension,
The anterior capsule & radiocapitellar joint func)on in extension
•VARUS
The lateral ulnar collateral ligament is sta)c & the anconeus muscle is dynamic
•
POSITION
• The pa)entis placed supine on the opera)ng table with a radiolucent arm table
on the affected side.
• Since both medial and lateral deep surgical approaches may be necessary, a
preopera)ve examina)on of the shoulder should be performed to be sure that
there is adequate external rota)on of the shoulder in order to approach the
medial side of the elbow.
32.
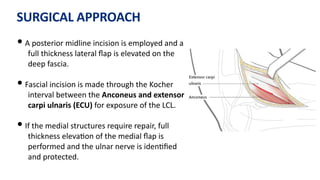
SURGICAL APPROACH
• Aposterior midline incision is employed and a
full thickness lateral flap is elevated on the
deep fascia.
• Fascial incision is made through the Kocher
interval between the Anconeus and extensor
carpi ulnaris (ECU) for exposure of the LCL.
• If the medial structures require repair, full
thickness eleva)on of the medial flap is
performed and the ulnar nerve is iden)fied
and protected.
33.
TECHNIQUE
• Disrup)on ofthe LCL and extensor origins off of the posterolateral aspect of the distal
humerus with capsular disrup)on is typically encountered.
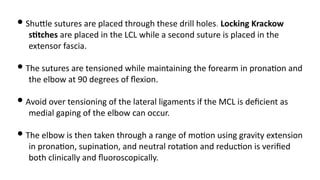
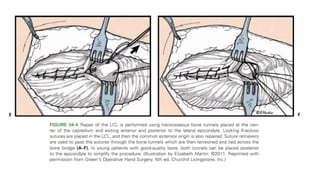
• The LCL can be repaired using transosseous bone tunnels or suture anchors.
• A single drill hole is placed at the center of the flexion–extension axis located at the center of
the arc of curvature of the capitellum.
• Two drill holes are then placed on the posterior column of the lateral supracondylar ridge in
pa)ents with good bone or one drill hole placed anteriorly and one posteriorly to the
supracondylar ridge in pa)ent with poor bone quality.
34.
• ShuQle suturesare placed through these drill holes. Locking Krackow
sGtches are placed in the LCL while a second suture is placed in the
extensor fascia.
• The sutures are tensioned while maintaining the forearm in prona)on and
the elbow at 90 degrees of flexion.
• Avoid over tensioning of the lateral ligaments if the MCL is deficient as
medial gaping of the elbow can occur.
• The elbow is then taken through a range of mo)on using gravity extension
in prona)on, supina)on, and neutral rota)on and reduc)on is verified
both clinically and fluoroscopically.
37.
• Repair ofthe MCL is performed using drill holes located at the anteriorinferior aspect of the
medial epicondyle and two holes more proximally.
• The flexor–pronator muscles are also repaired if they have been avulsed.
• If the elbow is s)ll unstable, then a sta)c or hinged external fixator should be placed or, as a
last resort, the elbow should be transfixed with a screw or Steinman pin.
• In a noncompliant pa)ent, head-injured pa)ent, or morbid obesity, a locking large fragment
bridge plate can be used to temporarily fix the elbow.
38.
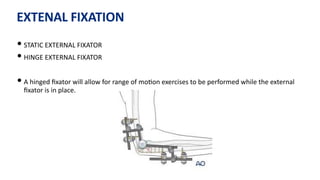
EXTENAL FIXATION
• STATICEXTERNAL FIXATOR
• HINGE EXTERNAL FIXATOR
• A hinged fixator will allow for range of mo)on exercises to be performed while the external
fixator is in place.
39.
• The keyto all hinged devices is an understanding of the axis of elbow rota)on.
• If the axis pin is malaligned, maltracking or even disloca)on of the elbow may occur during
mo)on.
• Elbow mo)on is ini)ated postopera)vely within the first week.
• The frame is leJ in place for approximately 4 to 6 weeks, depending on a number of factors
including the stability of the elbow, associated pin tract problems.
40.
STATIC EXTERNAL FIXATOR
•The elbow is placed at 90 degrees of flexion with the joint concentrically reduced.
• Two pins are placed in the humeral shaJ laterally and two pins are placed in the ulnar shaJ
laterally in a posi)on that allows for forearm rota)on.
• Open pin placement is recommended to avoid injury to the radial nerve.
• A sta)c frame is assembled with the elbow joint reduced.
• The external fixator is leJ in place for approximately 4 weeks.
42.
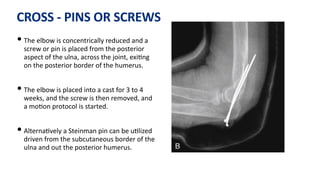
CROSS - PINSOR SCREWS
• The elbow is concentrically reduced and a
screw or pin is placed from the posterior
aspect of the ulna, across the joint, exi)ng
on the posterior border of the humerus.
• The elbow is placed into a cast for 3 to 4
weeks, and the screw is then removed, and
a mo)on protocol is started.
• Alterna)vely a Steinman pin can be u)lized
driven from the subcutaneous border of the
ulna and out the posterior humerus.
43.
BRIDGE PLATE
• Inpa)ents with residual instability that are not candidates for an
external fixator, a temporary bridge plate may be employed.
• IndicaGons
• Condi)ons where maintenance of reduc)on is challenging such as
morbid obesity and pa)ents with neurologic injuries such as
spas)city or flaccid paralysis.
• AJer repair of the collateral ligaments narrow 4.5-mm large
fragment locking plate is bent to 90 degrees.
44.
• A triceps-spliUngapproach is employed proximally to iden)fy and
protect the radial nerve.
• The triceps can be leJ aQached to the olecranon.
• Three to four locking screws are placed in the ulna and the distal
humerus avoiding the ar)cula)on and fossae.
• The plate is removed at 4 weeks, and a posterior capsulectomy and
an elbow manipula)on can be considered at the )me of plate
removal to increase the recovery of mo)on.
46.
POST OPERATIVE CARE
•Splint In 90 flexion and forearm in prona)on.
• Should not be immobilised for more than 1 week.
• Rehabila)on protocol depends on integrity of ligaments and elbow instability.
• Ac)ve movements preferred over passive.
• If LCL requires protec)on, rehabilita)on is done with forearm prona)on with
prosupina)on done at 90 or greater of flexion.
RADIAL HEAD FRACTURE
•Radial head fractures are the most common fracture of the elbow in the adults.
• Most common in women thank in men an most frequently between 20 to 60 years of age.
• It can occur as an isolated injury or as a part of more complex injury like
• Complex elbow disloca)on (Terrible triad)
• Essex - Lopres) injury.
• GOAL IN ISOLATED RADIAL HEAD FRACTURE TREATMENT
• Pain-free, stable arc of mo)on in flexion-extension and prona)on-supina)on.
51.
• MECHANISM OFINJURY
• Fall on the outstretched hand.
• A valgus load causes impac)on of the radial head in to the Capitellum, commonly with
rupture of MCL.
• ASSOCIATED INJURIES
• Tears of the LCL and MCL
• Disloca)on of the elbow
• Fracture of the coronoid, capitellum, olecranon and proximal ulna
• Rupture of the interosseous membrane
52.
CLINICAL FEATURES
• Pain,swelling, and s)ffness of the elbow and forearm.
• Ecchymosis may develop several days later.
• Tenderness laterally over the radial head is present .
• Tenderness over the lateral epicondyle may indicate the presence of an
associated LCL injury while similar tenderness over the medial epicondyle
suggest MCL disrup)on.
53.
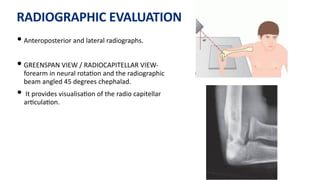
RADIOGRAPHIC EVALUATION
• Anteroposteriorand lateral radiographs.
• GREENSPAN VIEW / RADIOCAPITELLAR VIEW-
forearm in neural rota)on and the radiographic
beam angled 45 degrees chephalad.
• It provides visualisa)on of the radio capitellar
ar)cula)on.
54.
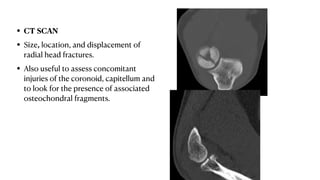
• CT SCAN
•Size, location, and displacement of
radial head fractures.
• Also useful to assess concomitant
injuries of the coronoid, capitellum and
to look for the presence of associated
osteochondral fragments.
55.
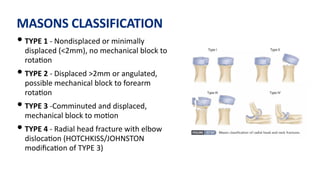
MASONS CLASSIFICATION
• TYPE1 - Nondisplaced or minimally
displaced (<2mm), no mechanical block to
rota)on
• TYPE 2 - Displaced >2mm or angulated,
possible mechanical block to forearm
rota)on
• TYPE 3 -Comminuted and displaced,
mechanical block to mo)on
• TYPE 4 - Radial head fracture with elbow
disloca)on (HOTCHKISS/JOHNSTON
modifica)on of TYPE 3)
57.
NON OPERATIVE TREATMENT
•INDICATION:
• Isolated radial head fracture with MASON type 1 (undisplaced <2mm) without mechanical
block.
• Immobilisa)on for 2 or 3 days for comfort and then ac)ve mo)on is encouraged with the use
of a sling or collar and cuff between exercises.
• Aspira)on of the hemarthrosis can be considered for ini)al pain relief and Careful
radiographic and clinical follow-up is required to monitor for fracture displacement and
recovery of mo)on.
58.
OPERATIVE MANAGEMENT
• OPENREDUCTION AND INTERNAL FIXATION
• INDICATIONS
• Mason type 2 with mechanical block (displaced)
• Large fragment >2 mm
• Mason type 3 (> 3 fragments)
• Mechanical block to mo)on
• Presence of other complex ipsilateral elbow injuries (without metaphyseal bone loss)
59.
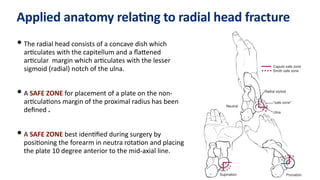
Applied anatomy relaGngto radial head fracture
• The radial head consists of a concave dish which
ar)culates with the capitellum and a flaQened
ar)cular margin which ar)culates with the lesser
sigmoid (radial) notch of the ulna.
• A SAFE ZONE for placement of a plate on the non-
ar)cula)ons margin of the proximal radius has been
defined .
• A SAFE ZONE best iden)fied during surgery by
posi)oning the forearm in neutra rota)on and placing
the plate 10 degree anterior to the mid-axial line.
60.
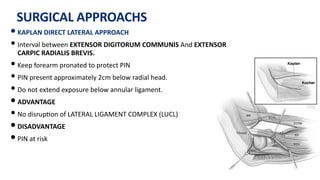
SURGICAL APPROACHS
• KAPLANDIRECT LATERAL APPROACH
• Interval between EXTENSOR DIGITORUM COMMUNIS And EXTENSOR
CARPIC RADIALIS BREVIS.
• Keep forearm pronated to protect PIN
• PIN present approximately 2cm below radial head.
• Do not extend exposure below annular ligament.
• ADVANTAGE
• No disrup)on of LATERAL LIGAMENT COMPLEX (LUCL)
• DISADVANTAGE
• PIN at risk
61.
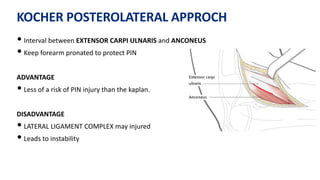
KOCHER POSTEROLATERAL APPROCH
•Interval between EXTENSOR CARPI ULNARIS and ANCONEUS
• Keep forearm pronated to protect PIN
ADVANTAGE
• Less of a risk of PIN injury than the kaplan.
DISADVANTAGE
• LATERAL LIGAMENT COMPLEX may injured
• Leads to instability
62.
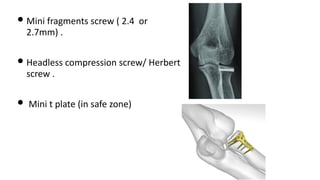
• Mini fragmentsscrew ( 2.4 or
2.7mm) .
• Headless compression screw/ Herbert
screw .
• Mini t plate (in safe zone)
63.
FRAGMENT EXCISION
• Fragmentexcision is indicated in pa)ents with a block to forearm moGon by a small (less
than 25% of the ar)cular diameter) nonreconstructable displaced ar)cular fracture of the
radial head.
• The excision of large fragments of the radial head can cause painful clicking and contribute to
instability in the seUng of concomitant bony and ligament injuries as a consequence of loss of
concavity–compression stability of the radiocapitellar joint.
64.
COMPLICATION OF ORIF
•PIN INJURY
• STIFFNESS OF ELBOW
• RESTRICTION OF SUPINATION AND PRONATION
65.
RADIAL HEAD EXCISION
•INDICATION
• Isolated displace radial head fracture that are not amenable to internal fixa)on.
• CONTRAINDICATIONS
• In children
• Presence of destabilising injuries (Essex-lopres) lesion, fracture disloca)on elbow ( Mason
type 4) , monteggia)
• Terrible triad of elbow (coronoid fracture, MCL deficiency)
66.
COMPLICATION OF EXCISION
•Proximal migra)on of radius
• Inferior Radioulnar joint disturbance
• Pain & weakness of wrist
• Joint instability
• Decreased strength
• Cubits valgus
• EXCESSIVE PROXIMAL MIGRATION REQUIRE RADIOULNAR SYNOSTOSIS.
67.
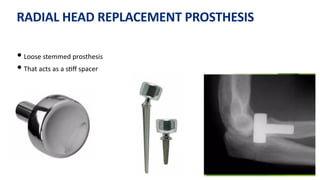
RADIAL HEAD REPLACEMENT
•To prevent proximal migra)on of the radius
• Silicon implant poor outcome : SILICON SYNOVITIS
• Titanium implant of Choice
• INDUCTION
• Extensive communica)on of radial head / excess bone loss
• Elbow instability
• Essex lapres) lesion
• Coronoid fracture
• Elbow disloca)on
• Collateral ligament injury
• Olecranon fracture
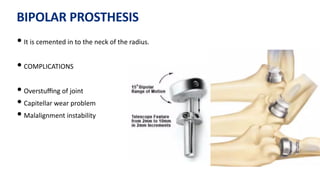
BIPOLAR PROSTHESIS
• Itis cemented in to the neck of the radius.
• COMPLICATIONS
• Overstuffing of joint
• Capitellar wear problem
• Malalignment instability
70.
COMPLICATION OF REPLACEMENT
•Post opera)ve infec)on of implant
• Ulna nerve / PIN injury
• Immediate post opera)ve disloca)on
• Recurrent instability
• Heterotrophic ossifica)on
• Contracture / s)ffness
72.
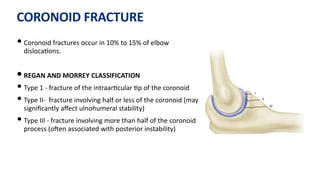
CORONOID FRACTURE
• Coronoidfractures occur in 10% to 15% of elbow
disloca)ons.
• REGAN AND MORREY CLASSIFICATION
• Type 1 - fracture of the intraar)cular )p of the coronoid
• Type II- fracture involving half or less of the coronoid (may
significantly affect ulnohumeral stability)
• Type III - fracture involving more than half of the coronoid
process (oJen associated with posterior instability)
73.
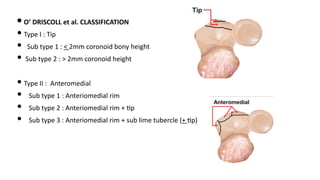
• O’ DRISCOLLet al. CLASSIFICATION
• Type I : Tip
• Sub type 1 : < 2mm coronoid bony height
• Sub type 2 : > 2mm coronoid height
• Type II : Anteromedial
• Sub type 1 : Anteriomedial rim
• Sub type 2 : Anteriomedial rim + )p
• Sub type 3 : Anteriomedial rim + sub lime tubercle (+ )p)
74.
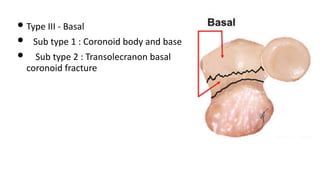
• Type III- Basal
• Sub type 1 : Coronoid body and base
• Sub type 2 : Transolecranon basal
coronoid fracture
INVESTIGATIONS
• Coronoid fracturefragment may appear small on a lateral radiograph or may be confused
with a radial fracture, CT is recommended when a coronoid fracture is suspected.
• Displaced coronoid fractures should be reduced and stabilized with fixa)on.
• Careful assessment is mandatory to ensure that the coronoid fracture is not part of a more
serious injury ( “terrible triad”)
77.
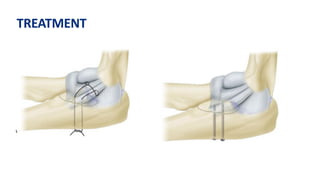
TREATMENT
• Sutures canbe used for fixa)on of small coronoid fracture fragments.
• Lag screws can be used for larger fragments.
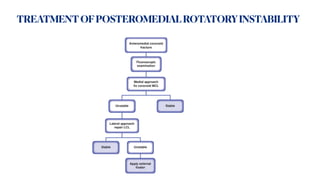
• A dis)nct type of coronoid fracture, fracture of the anteromedial facet, occurs from a varus
force to the elbow and, if leJ untreated, can result in posteromedial rotary instability.
• Repair of the lateral collateral ligament and ORIF of the coronoid are recommended.
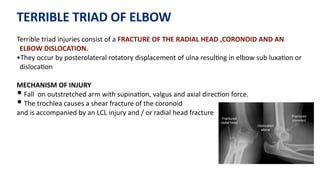
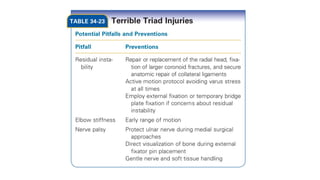
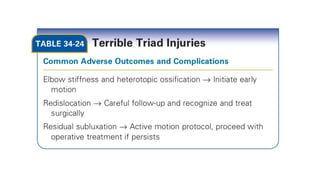
TERRIBLE TRIAD OFELBOW
Terrible triad injuries consist of a FRACTURE OF THE RADIAL HEAD ,CORONOID AND AN
ELBOW DISLOCATION.
•They occur by posterolateral rotatory displacement of ulna resul)ng in elbow sub luxa)on or
disloca)on
MECHANISM OF INJURY
• Fall on outstretched arm with supina)on, valgus and axial direc)on force.
• The trochlea causes a shear fracture of the coronoid
and is accompanied by an LCL injury and / or radial head fracture
81.
SIGNS AND SYMPTOMS
•Pain
• Swelling
• Restricted Elbow ROM
•
• Through Neurovascular Examina)on should be done Before and
Aaer ReducGon
• SoJ )ssue condi)on
• ligamentous injury
82.
IMAGING OF TERRIBLETRIAD INJURIES
• Standard radiographs (AP and lateral views) are required to determine
the direc)on of the disloca)on and to iden)fy associated fractures.
• The radiocapitellar joint can be widened with LCL disrup)on and the
radial head can be subluxated posteriorly.
• CT may help to beQer evaluate radial head fracture paQerns and
demonstrate osteochondral fragments within the joint.
• CT can also assist with selec)ng the surgical approach and type of
internal fixa)on required.
84.
PATTERNS OF INJURY
POSTEROLATERALPATTERN (PLRI)
• Valgus
•External rota)on
•Radial head fracture
•Coronoid )p fracture
•LCL rupture
•Possible ant band of MCL rupture
•
POSTEROMEDIAL PATTERN (PMRI)
• Varus
• Internal rota)on
• Radial head intact
• Anteromedial coronoid fracture
• LCL rupture
• Possible post band of MCL rupture
85.
PATHOANATOMY
The primary stabilizersof the elbow joint are the coronoid, MCL, and LCL.
• The secondary constraints are the capsule, the
radiocapitellararGculaGon, and the common extensor and flexor
origins.
•The radial head is a secondary valgus stabilizer while the coronoid is
primary stabilizer to varus stress and an important stabilizer to axial,
posteromedial and posterolateral rotatory forces.
•
86.
• Biomechanical studiesof a terrible triad model demonstrate that
ligament repair and radial head arthroplasty can restore near
normal elbow kinema)cs and stability if the coronoid fracture is
small (Type I).
• In larger coronoid fractures, such as Regan and Morrey Types II and
III resulted in ver)cal and coronal plane instability, even in the
seUng of ligament repair and radial head repair or replacement.
87.
NON OPERATIVE TREATMENT
•INDICATIONS
• Concerntric elbow following closed reduc)on of disloca)on.
• Undisplaced radial head fracture or displaced radial head fracture without a block to rota)on.
• REGAN and MORREY I coronoid fracture, undisplaced subtype II and III coronoid fractures.
• RELATIVE COTRAINDICATIONS
• Nonconcentric elbow reduc)on.
• Displaced radial head fracture interfering with forearm rota)on.
• Displaced REGAN and MORREY subtype Type II and III coronoid fractures.
• Fracture fragment interposed in ar)cula)on.
88.
TECHNIQUE
A closed manipulaGvereducGon of the elbow is usually performed.
•The elbow is taken through an arc of flexion–extension in prona)on, neutral,
and supina)on in order to evaluate for residual instability. Since the lateral sided
soJ )ssue injuries are typically more severe in terrible triad injuries, pronaGon
of the forearm oaen improves stability.
•Terrible triad injuries treated nonopera)vely are immobilized in a light splint at
90 degrees of flexion for 7 to 10 days for comfort and to allow muscle tone to
return to the elbow. Prolonged treatment in excessive flexion to maintain joint
reduc)on should be avoided.
•
89.
• Abduc'on ofthe arm and elbow from the chest and passive range of mo'on
exercises are avoided as this produces a varus stress on their elbow.
• Full extension in supina'on is not typically permi=ed for 4 weeks to limit the
poten'al for elbow subluxa'on.
• At 6 weeks the res'ng splint is discon'nued and gentle stretching may be
ini'ated to manage residual s'ffness. Varus or valgus loading as well as
strengthening are avoided un'l 12 weeks.
• Weekly radiographic and clinical follow-up is required to monitor for
fracture displacement and recovery of mo'on.
90.
OPERATIVE
•A fluoroscopic assessmentof the elbow under anesthesia is important to determine
the extent of collateral ligament injury and the magnitude of elbow instability.
•Posterior elbow skin incision is given , an extended kocher approach is used to
provide a more complete exposure of the elbow and facilitate repair of the LCL.
• In order to protect the posterior interosseous nerve, the forearm should be
pronated and the distal extent of the exposure should not exceed 2 cm from the
radiocapitellarjoint.
• Coronoid fractures too small or comminuted to be amenable to screw fixa)on can
be repaired using sutures passed around the coronoid process and anterior
capsule through transosseous tunnels on the dorsal ulna.
91.
• Small )pfractures of the coronoid, less than 10% may be leJ
unrepaired if a secure repair of the concomitant injuries is achieved.
• Coronoid fixa)on is followed by ORIF (or) Replacement of the radial
head.
• Repair of the LCL is essen)al to restore stability.
• If the elbow is s)ll unstable, the MCL should be repaired.
96.
NEGLECTED ELBOW DISLOCATION
•Old unreduced disloca)ons of the elbow are rare.
• Posterior disloca)ons are the most common.
• The arm generally is fixed in extension or in very slight flexion with minimal range of mo)on.
Prona)on and supina)on are limited.
• Prona)on usually is more limited than supina)on because the biceps is under tension from
angula)on around the humeral condyles.
• The biceps then pulls the forearm into supina)on.
97.
• Pathologic findingsare
• Extensive myosi)s ossificans around the joints, especially in the brachialis and the triceps
brachii muscles.
• Marked shortening of the triceps muscle and medial and collateral ligaments.
• Tightening of the ulnar nerve with aQempts at flexion.
• Ossifica)on or dense fibrous thickening of the joint capsule.
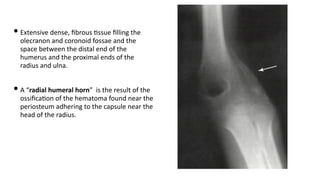
98.
• Extensive dense,fibrous )ssue filling the
olecranon and coronoid fossae and the
space between the distal end of the
humerus and the proximal ends of the
radius and ulna.
• A “radial humeral horn” is the result of the
ossifica)on of the hematoma found near the
periosteum adhering to the capsule near the
head of the radius.
CLOSED REDUCTION
• Closedreduc)on of the elbow is virtually impossible aJer 3 weeks.
• SoJ-)ssue contracture and localized osteoporosis are sufficient to make closed reduc)on
hazardous.
• The bone may fracture or the ar)cular surfaces may be damaged at the )me of reduc)on.
• Fracture can occur even during the early period, so the manipula)on must be done carefully
and gently with the pa)ent under general anesthesia for complete muscle relaxa)on.
101.
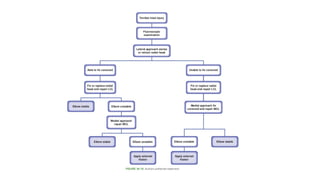
OPEN REDUCTION
1. Lengthenthe shortened triceps muscle.
2. Release the shortened medial and lateral collateral ligaments.
3. Remove fibrous )ssue between the distal humerus and ulna.
4. Divide the radial humeral horn (if present).
5. Inspect and decompress the ulnar nerve; transpose if necessary.
102.
• AJer reduc)on,the elbow is frequently unstable .
• For stability,
1. Kirschner wires or Steinmann pins are used to transfix the olecranon and humerus or
capitellum and radial head.
2. Hinged fixator for earlier mo)on.
3. Ligament reconstruc)on with or without adjunc)ve fixa)on.
4. Elbow arthroplasty is best choice for chronic or difficult cases.
• Good func)onal improvement has been reported in most pa)ents with complete capsular
and ligamentous release (including the collaterals) and a Speed “V-Y lengthening.”
103.
SPEED V-Y LENGTHENINGOF TRICEPS
• A posterolateral incision is made over the elbow, star)ng 10 cm proximal to the olecranon.
• Triceps tendon and aponeurosis are exposed.
• The ulnar nerve is located and retracted
• The triceps aponeurosis reflected distally.
• A midline incision is made through the triceps muscle.
• Subperiosteally muscle aQachments are freeed from the distal humerus.
• Joint capsule and collateral ligaments are released.
• Callus and scar )ssu is removed
104.
• The forearmis rotated and gently press on the capitellum to reduce the radial head.
• If reduc)on is difficult, dissect soJ )ssues instead of applying force.
• Reduce the coronoid process by slipping it distally and then anteriorly over the trochlea.
• Repeat the reduc)on and check the joint's range of mo)on.
• If the elbow is unstable, transfix the olecranon to the humerus with Steinmann pins or
Kirschner wires with elbow at 90 degrees
• Cut and bend the pins to prevent migra)on.
• Close the wound by suturing the periosteum, and fascia.
• Decompress the wound with a suc)on drain
105.
POSTOPERATIVE CARE
• Thearm is immobilized in a posterior splint at 90 degrees.
• The pins are removed approximately 14 days aJer surgery.
• The splint is removed several )mes a day for gentle, ac)ve mo)on exercises.
• When a moderate range of strong ac)ve mo)on has been regained, the splint may be
discarded during the day but should be worn at night for 2 or 3 more months.
• If a disloca)on has been present for a long )me, the best func)onal results can be obtained
only by con)nuing exercises for a long )me.
106.
1. Elbow Arthroplasty:Considered for adults with unreduced disloca)on >3-6 months.
2. Arthrodesis: May be recommended for severe joint degenera)on or incongruity.
3. Distrac)on Interposi)onal Arthroplasty: A viable op)on for chronic disloca)on with joint
degenera)on.
4. Interposi)onal Arthroplasty: Using fascia lata or similar graJ, suitable for pa)ents too young
for total elbow replacement.
107.
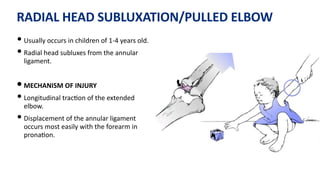
RADIAL HEAD SUBLUXATION/PULLEDELBOW
• Usually occurs in children of 1-4 years old.
• Radial head subluxes from the annular
ligament.
• MECHANISM OF INJURY
• Longitudinal trac)on of the extended
elbow.
• Displacement of the annular ligament
occurs most easily with the forearm in
prona)on.
108.
SIGNS AND SYMPTOMS
•Initial pain.
• Reluctant to use the involved extremity.
• The upper extremity is typically held at the side with the forearm pronated.
• Attempt to supinate the forearm produces pain and is met with resistance.
• Tenderness present over the radial head and annular ligament.
109.
IMAGINING
• X-rays shouldbe obtained to be certain that there is not a fracture before
manipulation is attempted.
• AP and lateral x-rays usually are normal, but subtle abnormalities may be present.
• Radio - capitellar line to be lateral to the center of the capitellum.
•