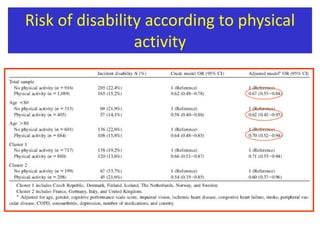
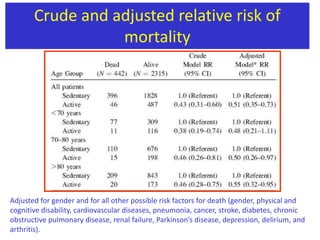
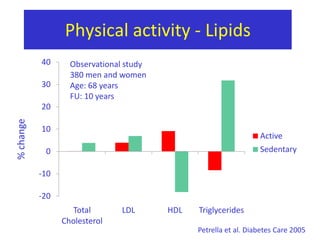
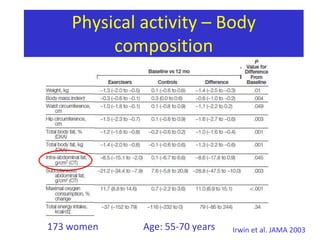
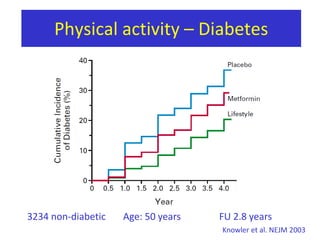
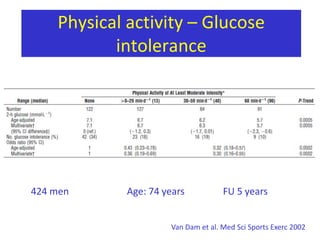
This document discusses the role of physical activity and exercise in aging populations. It covers factors for successful aging, characteristics of study populations according to physical activity levels, and the health benefits and goals of exercise for both younger-old and older-old age groups. The document also summarizes studies on the relationship between physical activity and reduced risks of mortality, cardiovascular disease, and other health outcomes. It provides guidelines for endurance and resistance training programs as well as screening recommendations for exercise in older adults.