Downloaded 124 times


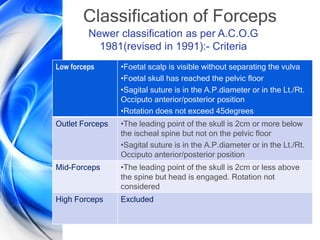
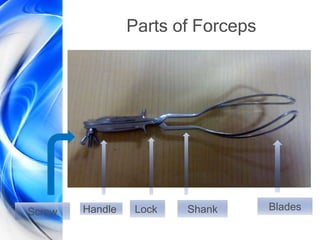
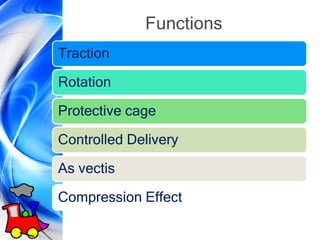
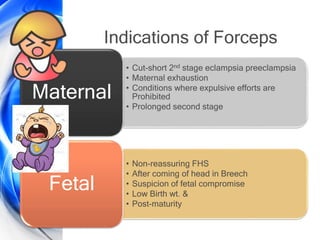
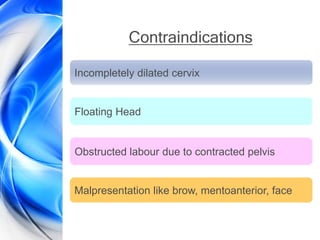





This document discusses obstetric forceps, including their history, classification, parts, functions, indications, contraindications, prerequisites for use, application techniques, complications, and special considerations like prophylactic forceps, trial forceps, and failed forceps. It notes that forceps were first used secretly in the 16th century in England and have since evolved in design. Forceps deliveries can be beneficial but also carry risks of injury to the mother or baby if improperly performed. Careful patient selection and operator skill are important.




















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)










