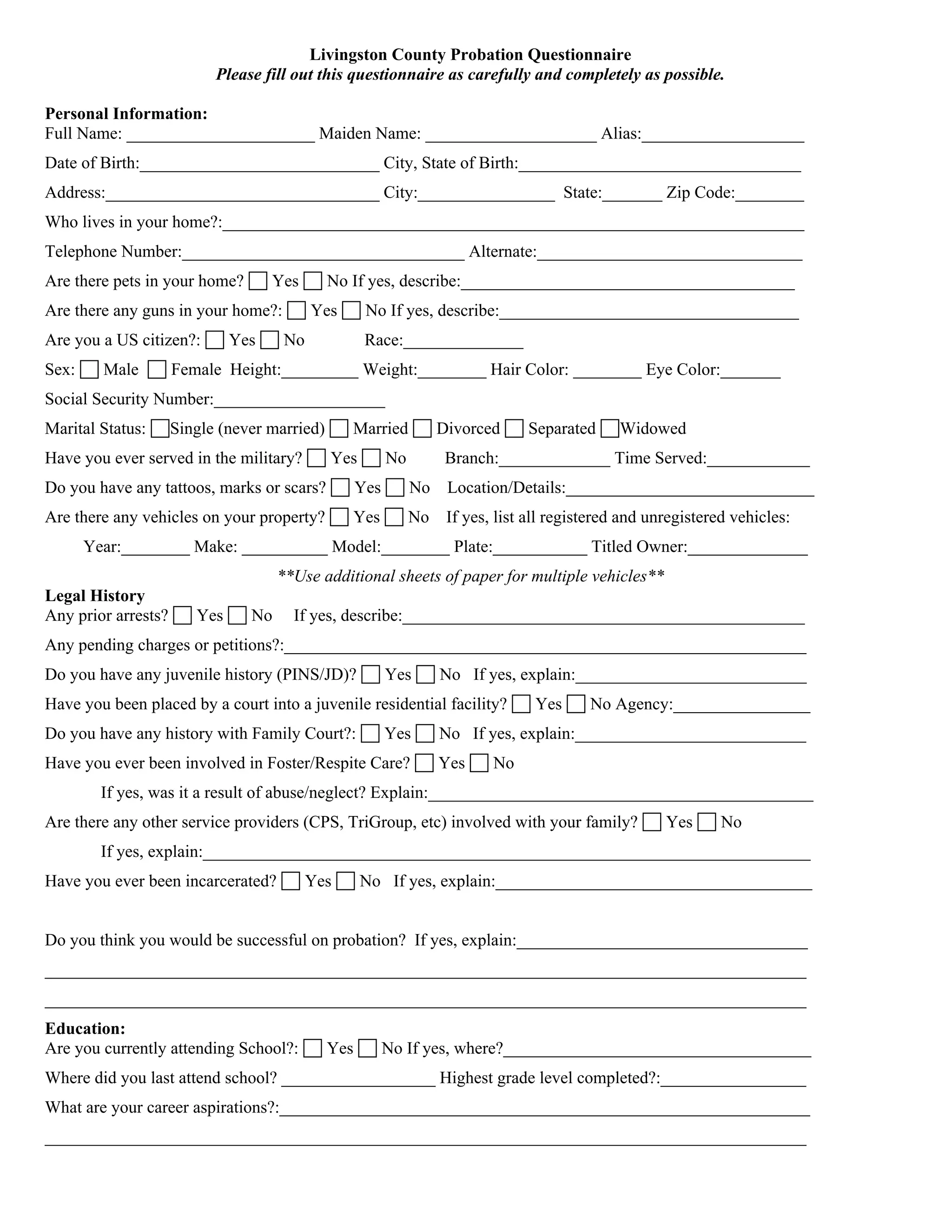
The document is a comprehensive questionnaire for Livingston County probation, requiring detailed personal information, including name, address, legal history, education, financial status, and family background. It includes inquiries about any history of arrests, substance abuse, mental health issues, and living conditions. Participants must answer questions related to their current situation and support systems to assess their eligibility and likelihood of success on probation.