1. Community nutrition focuses on assessing the nutritional status of individuals in a community, identifying nutritional problems and their causes, and developing programs and policies to improve nutrition.
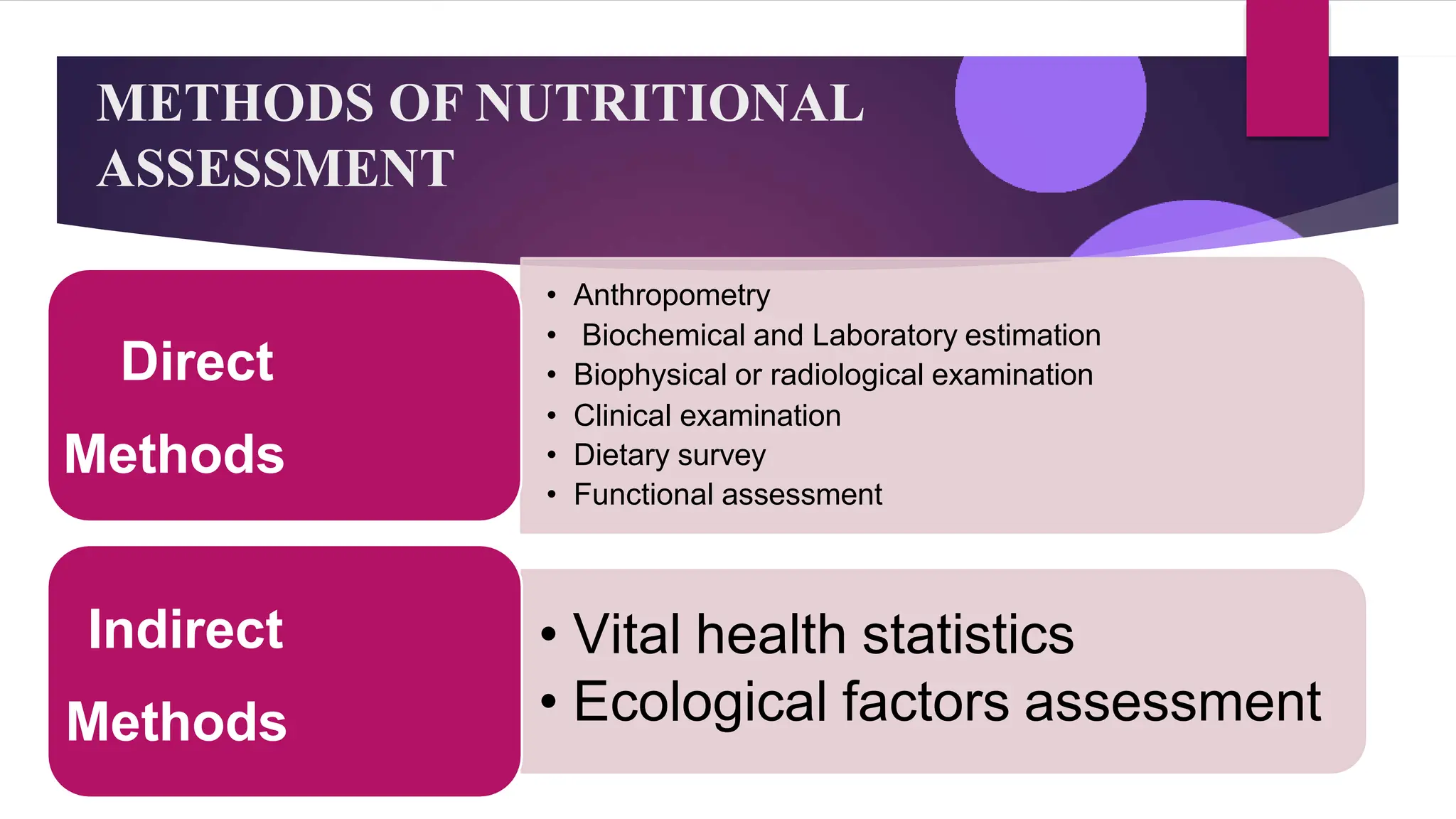
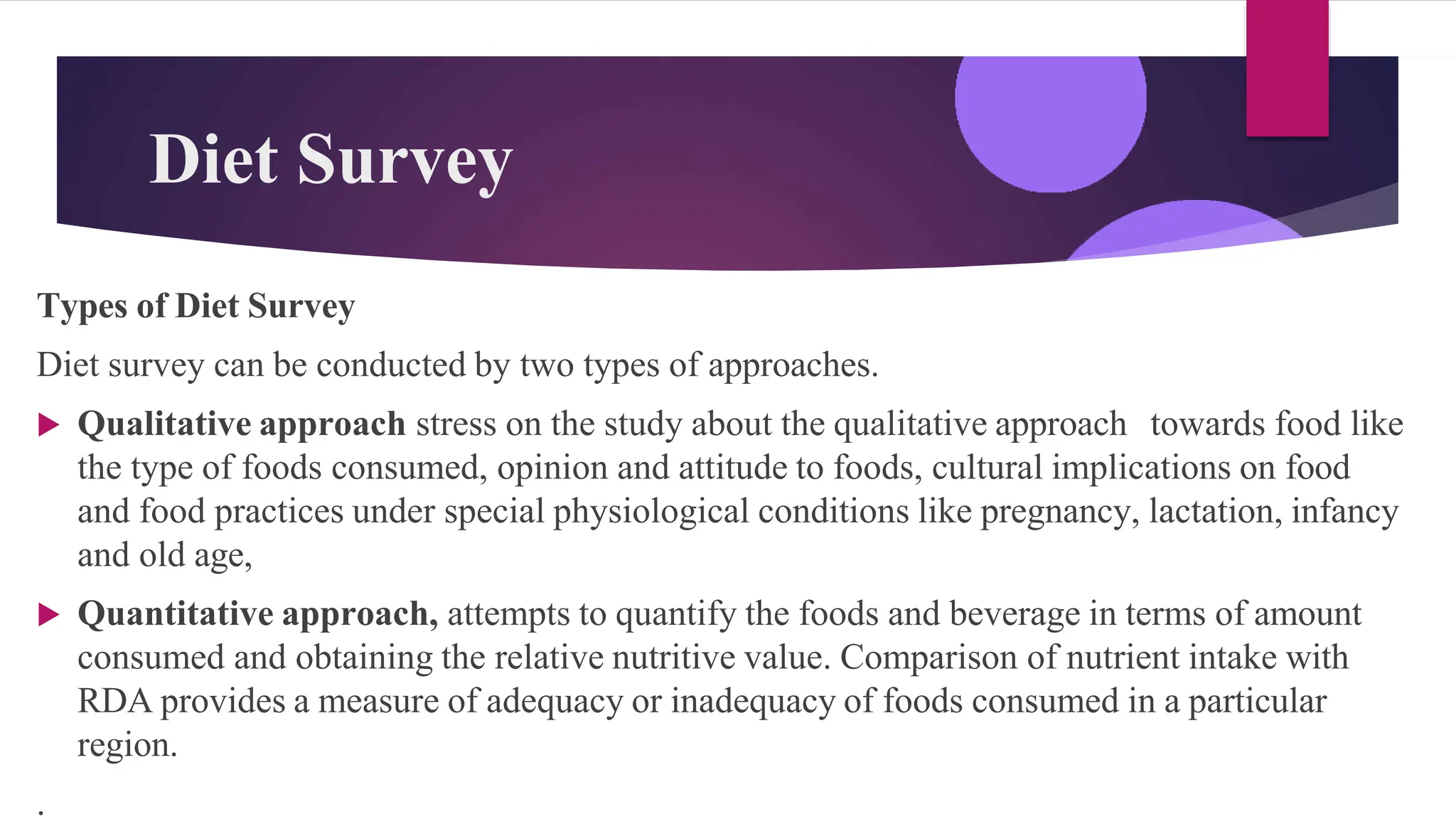
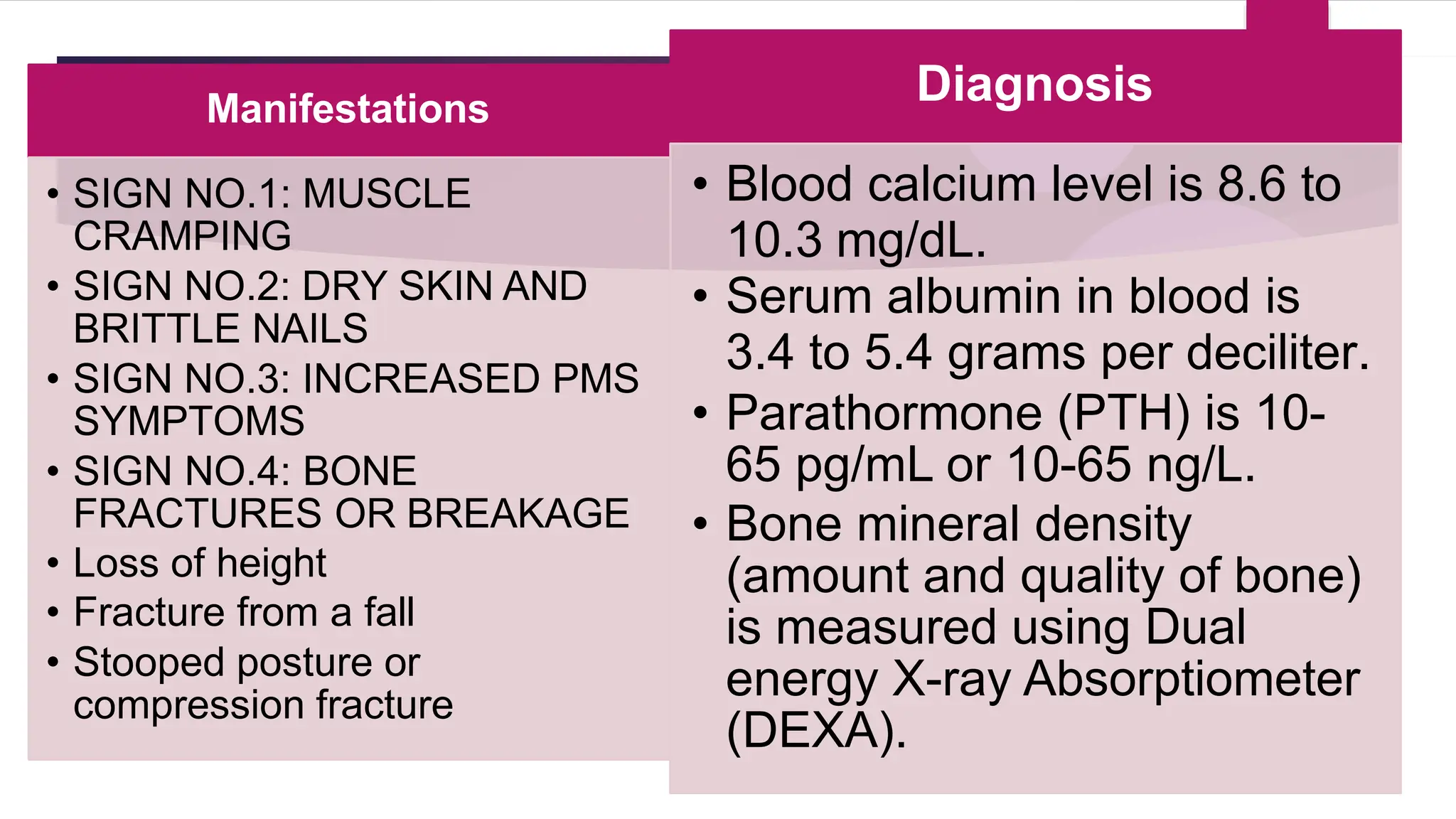
2. Assessing the nutritional status of a community involves determining the prevalence of malnutrition through anthropometric, biochemical and clinical measurements of individuals, as well as understanding dietary habits and food security issues.
3. The data collected from various assessment methods is then used to design appropriate community nutrition interventions, such as nutrition education programs, to address the nutritional problems identified and improve health outcomes.