Non-selective beta blockers (2).docx
•Download as DOCX, PDF•
0 likes•3 views

Complication of Epi and non-selective beta blocker

Recommended
More Related Content
Similar to Non-selective beta blockers (2).docx
Similar to Non-selective beta blockers (2).docx (20)
More from Virginia Western Community College
More from Virginia Western Community College (17)
Recently uploaded
Recently uploaded (20)
Non-selective beta blockers (2).docx
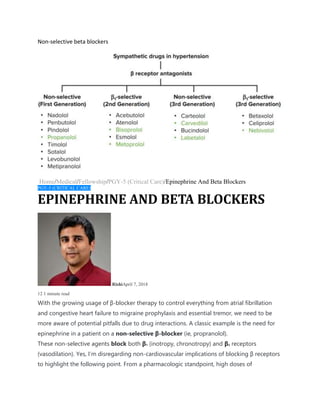
- 1. Non-selective beta blockers Home/Medical/Fellowship/PGY-5 (Critical Care)/Epinephrine And Beta Blockers PGY-5 (CRITICAL CARE) EPINEPHRINE AND BETA BLOCKERS RishiApril 7, 2018 12 1 minute read With the growing usage of β-blocker therapy to control everything from atrial fibrillation and congestive heart failure to migraine prophylaxis and essential tremor, we need to be more aware of potential pitfalls due to drug interactions. A classic example is the need for epinephrine in a patient on a non-selective β-blocker (ie, propranolol). These non-selective agents block both β1 (inotropy, chronotropy) and β2 receptors (vasodilation). Yes, I’m disregarding non-cardiovascular implications of blocking β receptors to highlight the following point. From a pharmacologic standpoint, high doses of
- 2. epinephrine will potentiate β1, β2, and alpha receptors. With a β-blocker like propranolol on board, epinephrine will primarily work through the α1 receptor – receptors on the peripheral vasculature involved with vasoconstriction. The net effect will be unopposed vasoconstriction leading to significant increases in blood pressure. This hypertension will, in turn, activate pressure receptors in the carotid sinus to increase vagal tone on the heart leading to profound decreases in heart rate. Worst case scenario, the patient will become asystolic. Funny thing because in true asystole, the treatment is chest compressions and…. you guessed it… epinephrine! � So why would we need to give epinephrine to these patients anyways? Anaphylaxis is one example! The mainstay of treatment will be epinephrine to stabilize further mast cell degranulation and promote bronchodilation, histaminergic blockers, steroids, and significant intravenous fluid resuscitation. A patient receiving β-blocker therapy may not mount the typical tachycardic response after receiving epinephrine. One will need to likely
- 3. escalate their doses rapidly but be mindful of paradoxical bradycardia related to the mechanism above! Another option is to give small doses of glucagon (1-3 mg followed by an infusion), but keep in mind that the evidence supporting the use of glucagon to reverse β-blocker therapy has only been shown in animal studies. Additionally, patients who receive this much glucagon invariably become nauseous and can vomit (oh the perils of an unprotected airway!) Hopefully this makes sense, but if not, drop me a comment below with questions! �