Downloaded 275 times
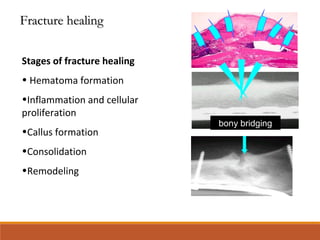
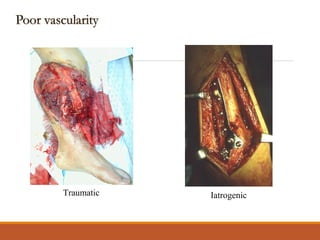
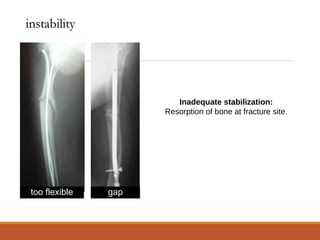
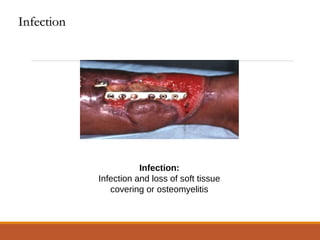
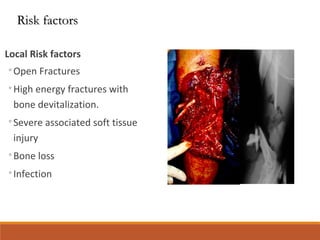

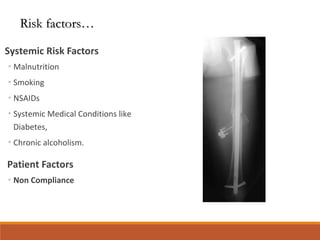
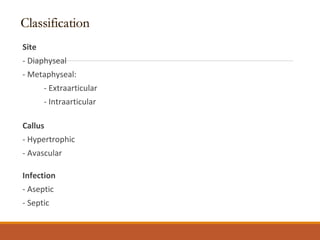
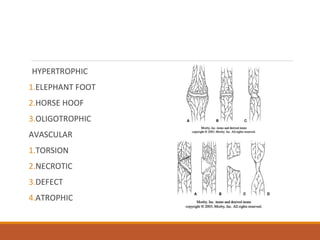
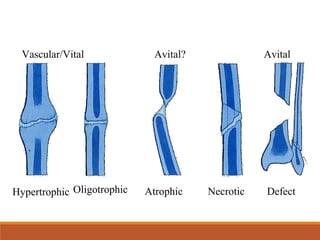
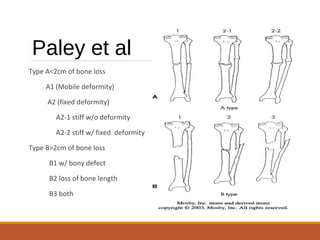
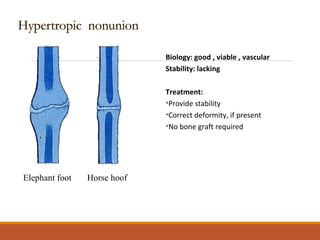
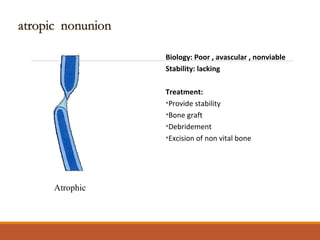
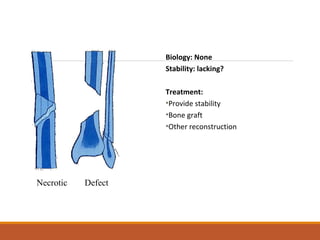

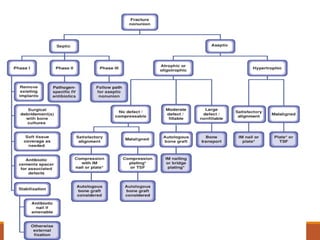


This document discusses nonunion fractures, including definitions, causes, classification, evaluation, and management. Some key points: - Nonunion occurs when a fracture fails to heal in the expected time and is unlikely to heal without further intervention. Delayed union is when healing is delayed but still possible with treatment. - Causes of nonunion include poor vascularity, instability, infection, and patient factors like smoking or diabetes. Types of nonunion include hypertrophic, atrophic, necrotic, and defect. - Evaluation involves standard radiographs and stress views. Treatment includes non-operative options like bracing or stimulation, or operative options like plating, nailing, bone grafting, and correction



















































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)



