NABH Accreditation Process & Quality Control Parameters
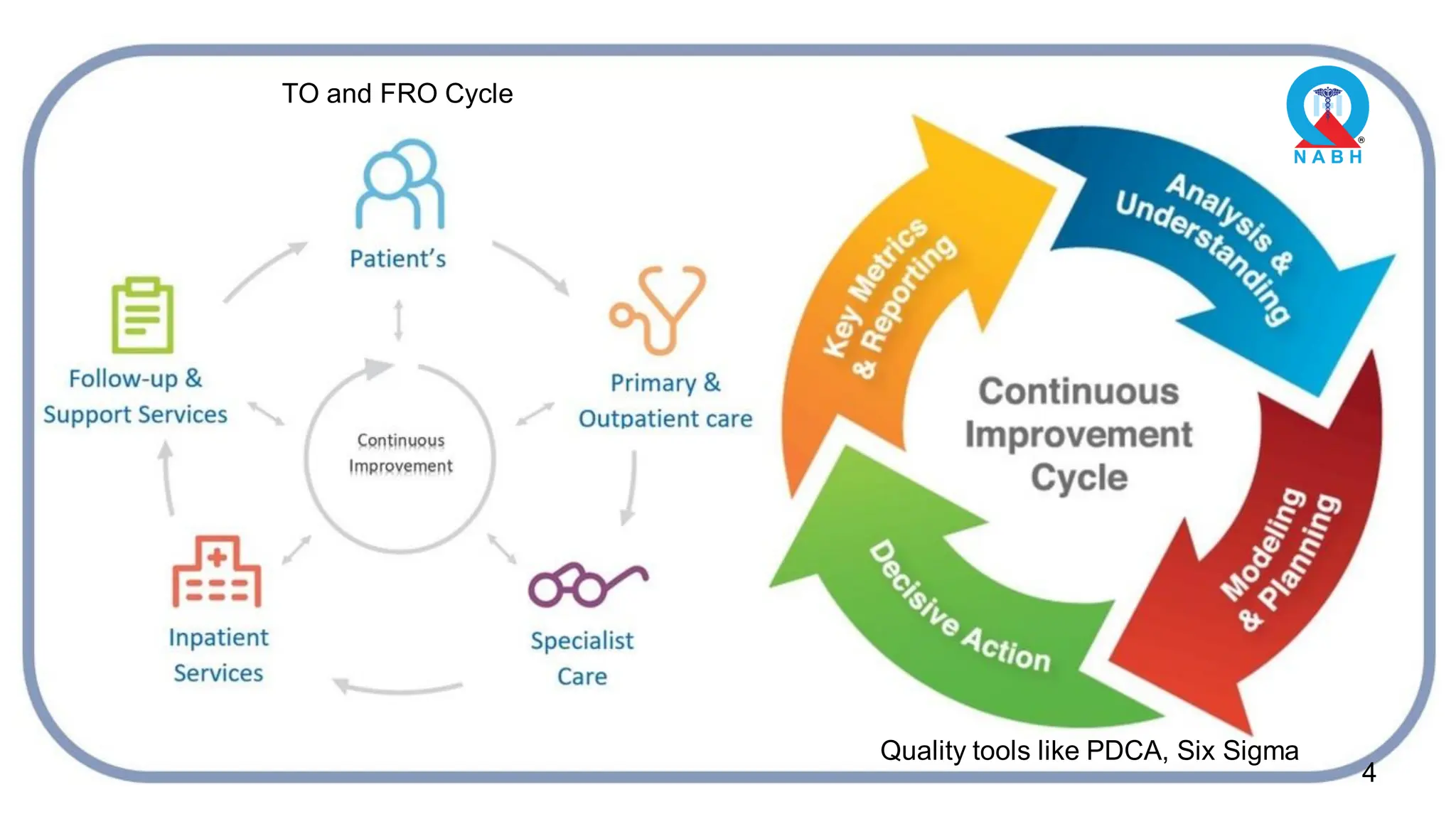
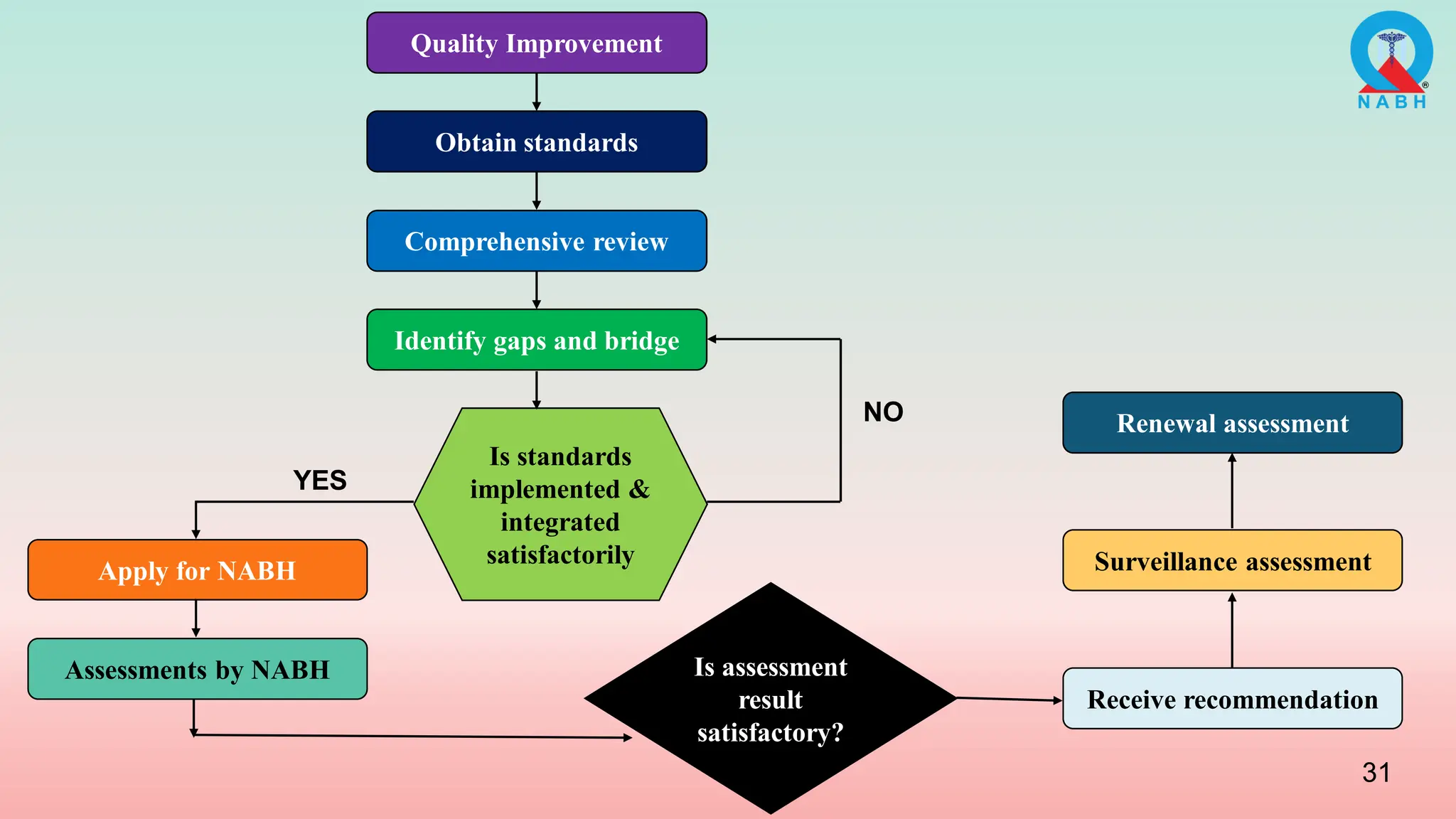
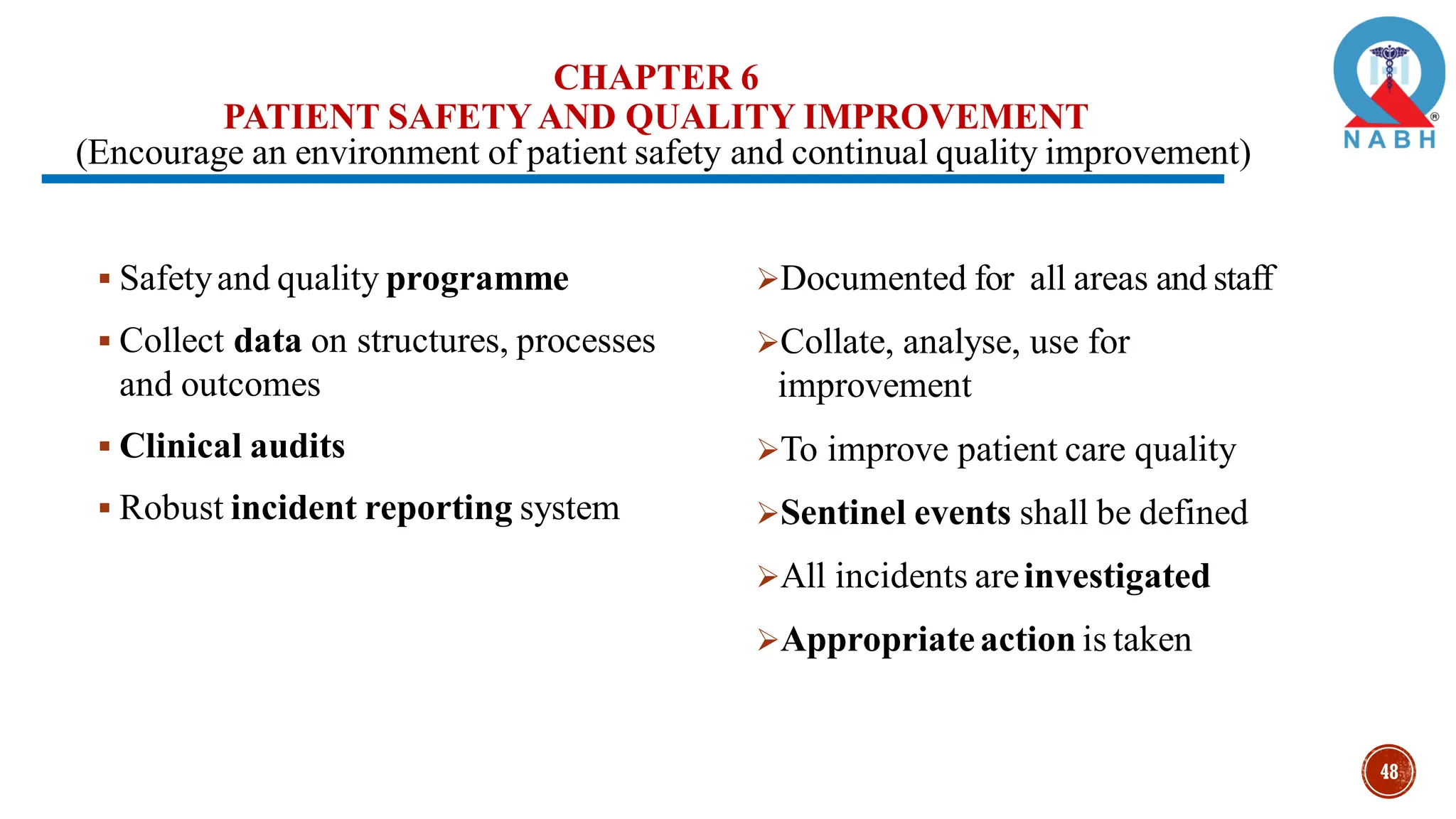
1. NABH outlines the process for healthcare organizations to achieve accreditation and continuously improve quality, including empowering leadership, investing in quality champions, and using tools like PDCA cycles.
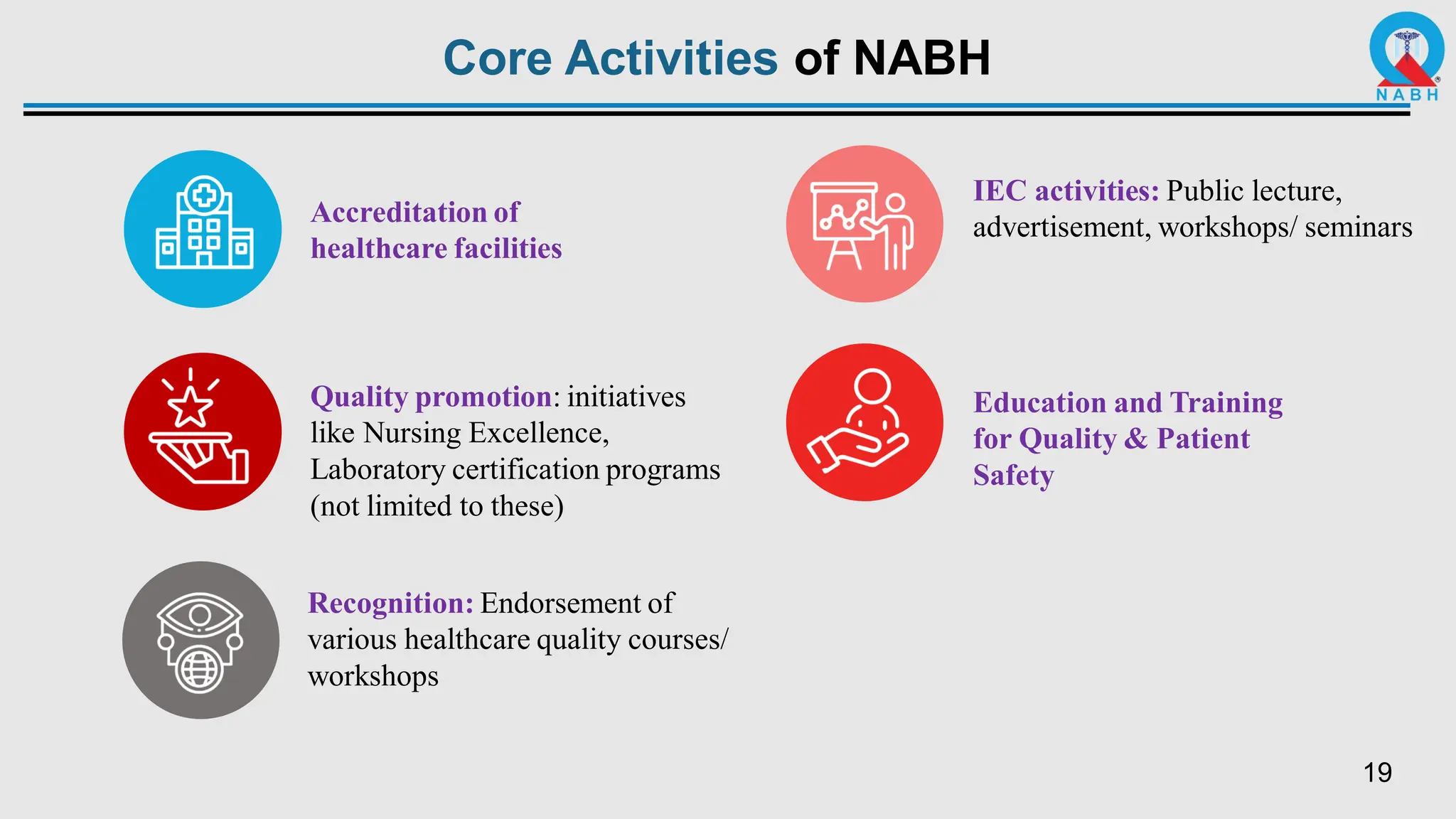
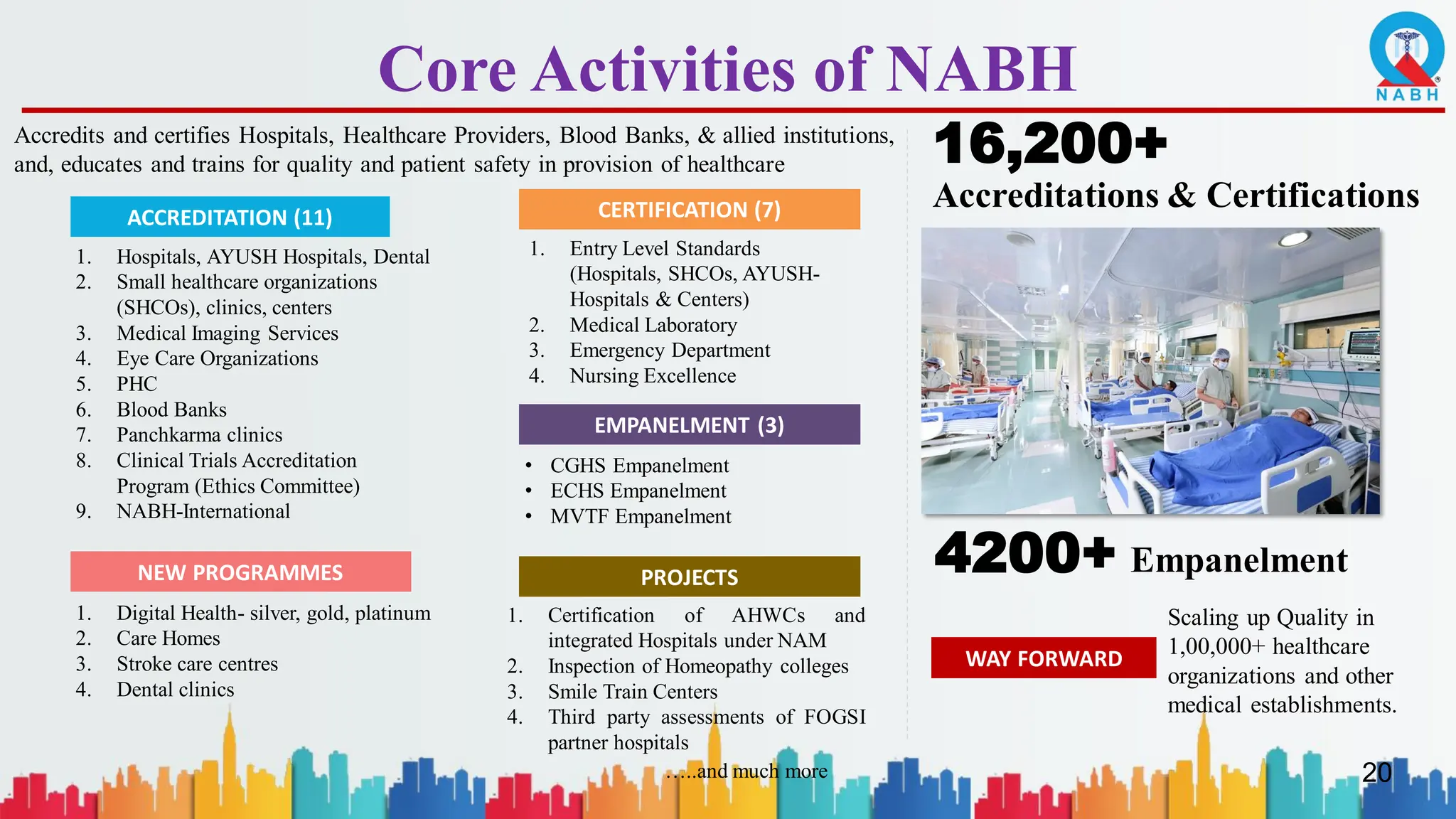
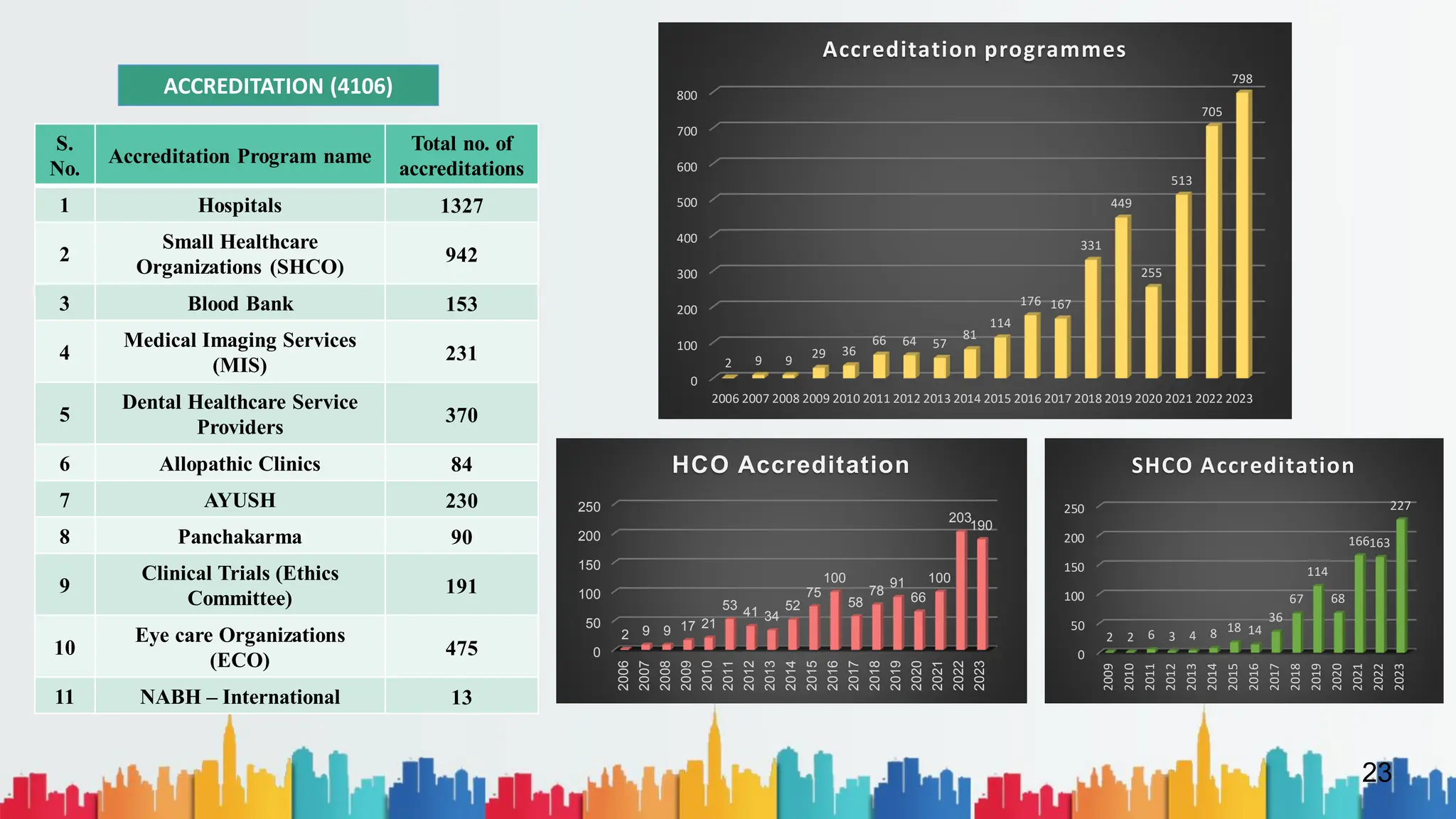
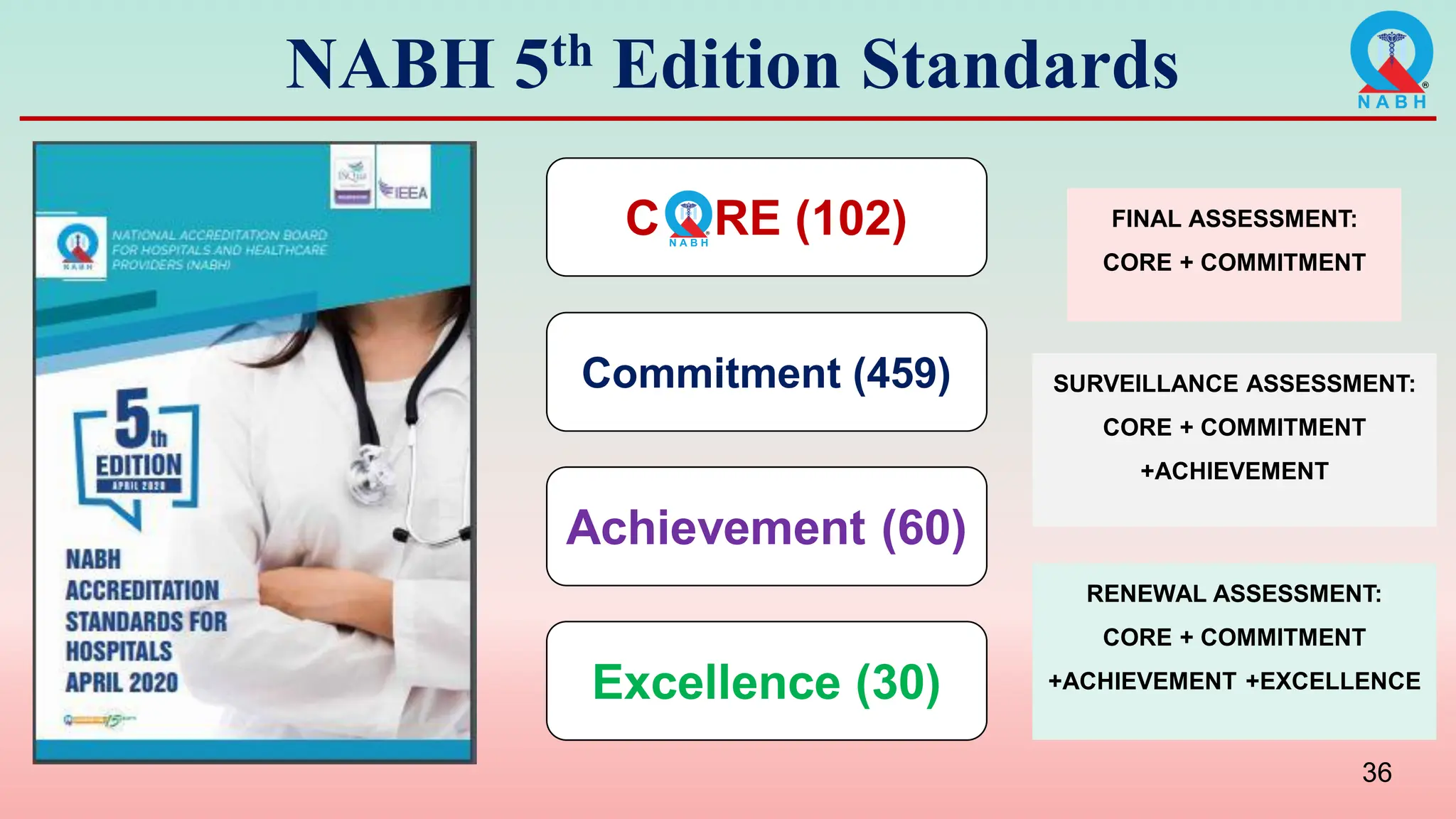
2. NABH accredits various types of healthcare facilities and certifies them based on established quality standards to ensure safe, effective, patient-centered, timely, efficient, and equitable care.
3. Achieving NABH accreditation is an ongoing process that requires continuous quality improvement rather than a single event, in order to embed a culture of quality in healthcare.