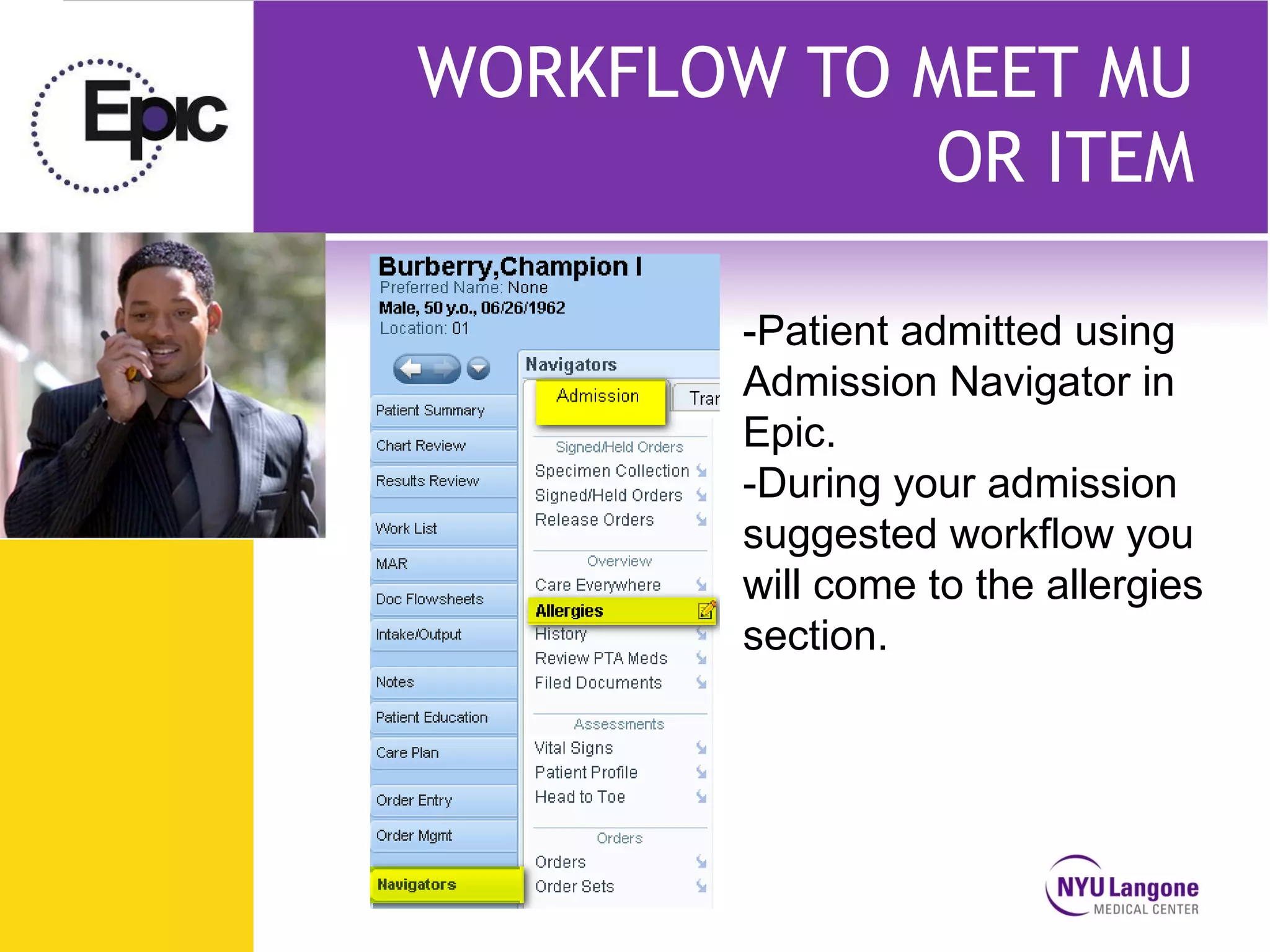
This presentation discusses how NYU can meet meaningful use objectives using the Epic electronic health record system. It begins with an overview of meaningful use and its goals of improving healthcare quality, reducing costs, and engaging patients. The presentation then demonstrates Epic workflows for documenting allergy information and smoking status, two key meaningful use objectives. It concludes by reviewing hospital reporting metrics and emphasizing the importance of accurate real-time documentation to achieve meaningful use goals.

































































![Trudel cms-rules-072810[1]](https://cdn.slidesharecdn.com/ss_thumbnails/trudel-cms-rules-0728101-100810094307-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
![Trudel Cms Rules 072810[1]](https://cdn.slidesharecdn.com/ss_thumbnails/trudelcmsrules0728101-12814484645456-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
![Trudel Cms Rules 072810[1]](https://cdn.slidesharecdn.com/ss_thumbnails/trudelcmsrules0728101-12814485135294-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
![Trudel Cms Rules 072810[1]](https://cdn.slidesharecdn.com/ss_thumbnails/trudelcmsrules0728101-12814486180502-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
![Trudel cms-rules-072810[1]](https://cdn.slidesharecdn.com/ss_thumbnails/trudel-cms-rules-0728101-100810090601-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
![Trudel Cms Rules 072810[1]](https://cdn.slidesharecdn.com/ss_thumbnails/trudelcmsrules0728101-12814488066912-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
![Trudel cms-rules-072810[1]](https://cdn.slidesharecdn.com/ss_thumbnails/trudel-cms-rules-0728101-100810090705-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)



























