Downloaded 78 times


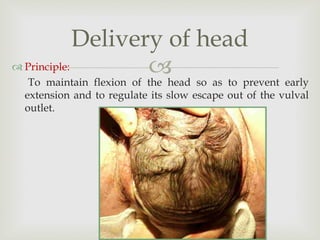
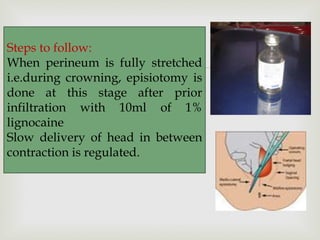


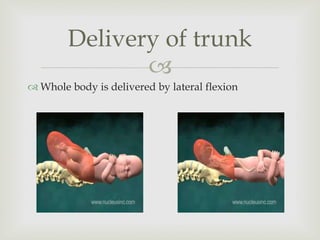
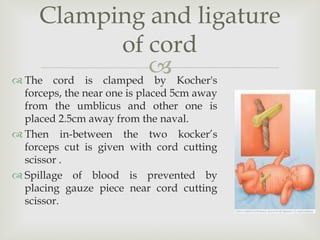


The document summarizes the management of the second stage of labor. It describes: 1) Events that occur in the second stage, including full dilation of the cervix, rupture of membranes, and stronger uterine contractions that help push the baby down the birth canal. 2) General measures taken during the second stage like monitoring the patient and preparing for delivery by cleaning the perineal area. 3) The process of delivery, including maintaining flexion of the baby's head during crowning, performing an episiotomy if needed, and regulating the slow delivery of the head and shoulders before delivering the trunk. 4) Clamping and cutting the umbilical cord after full delivery.






































![mechanism_of_labor[1].pptx obstetrics and gynaecology midwifery nursing mater...](https://cdn.slidesharecdn.com/ss_thumbnails/mechanismoflabor1-250610164745-6b6dfb9d-thumbnail.jpg?width=640&height=640&fit=bounds)











































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
