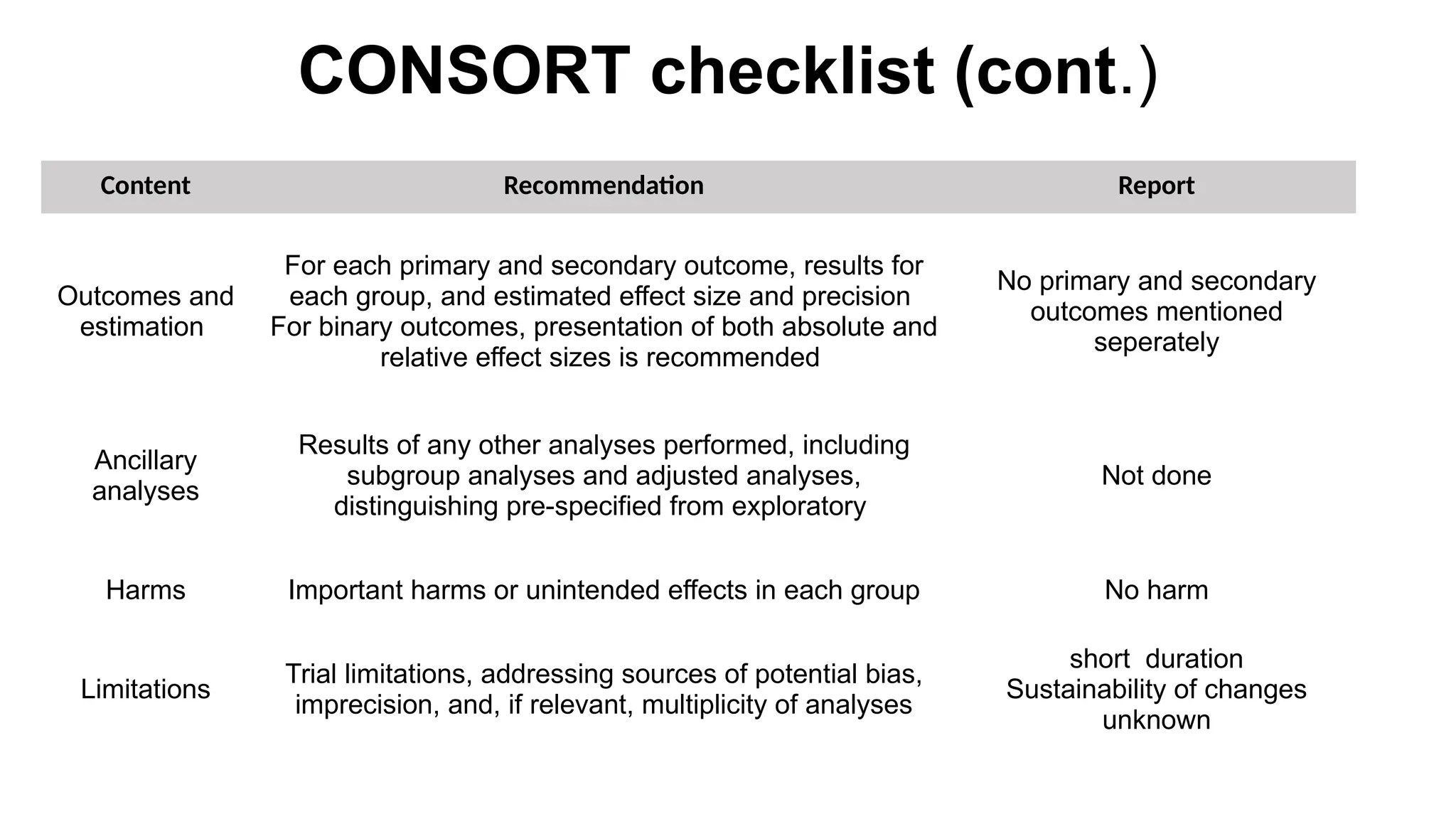
The study titled 'Seeds of Prevention' investigates the health behaviors of young adolescent girls in Uttar Pradesh, India, focusing on anemia, nutrition, and reproductive health through a cluster randomized control trial. Implemented in 30 schools with 1,800 participants, the intervention showed significant improvements in health behaviors, including increased consumption of iron folic acid and better menstrual hygiene. However, the short duration of the study and the sustainability of behavioral changes were identified as limitations.















































![Keys to Educational Psychology: [Irma, Eloff and Liesel, Ebersohn]](https://cdn.slidesharecdn.com/ss_thumbnails/pptpsikologiiv-161117164552-thumbnail.jpg?width=640&height=640&fit=bounds)