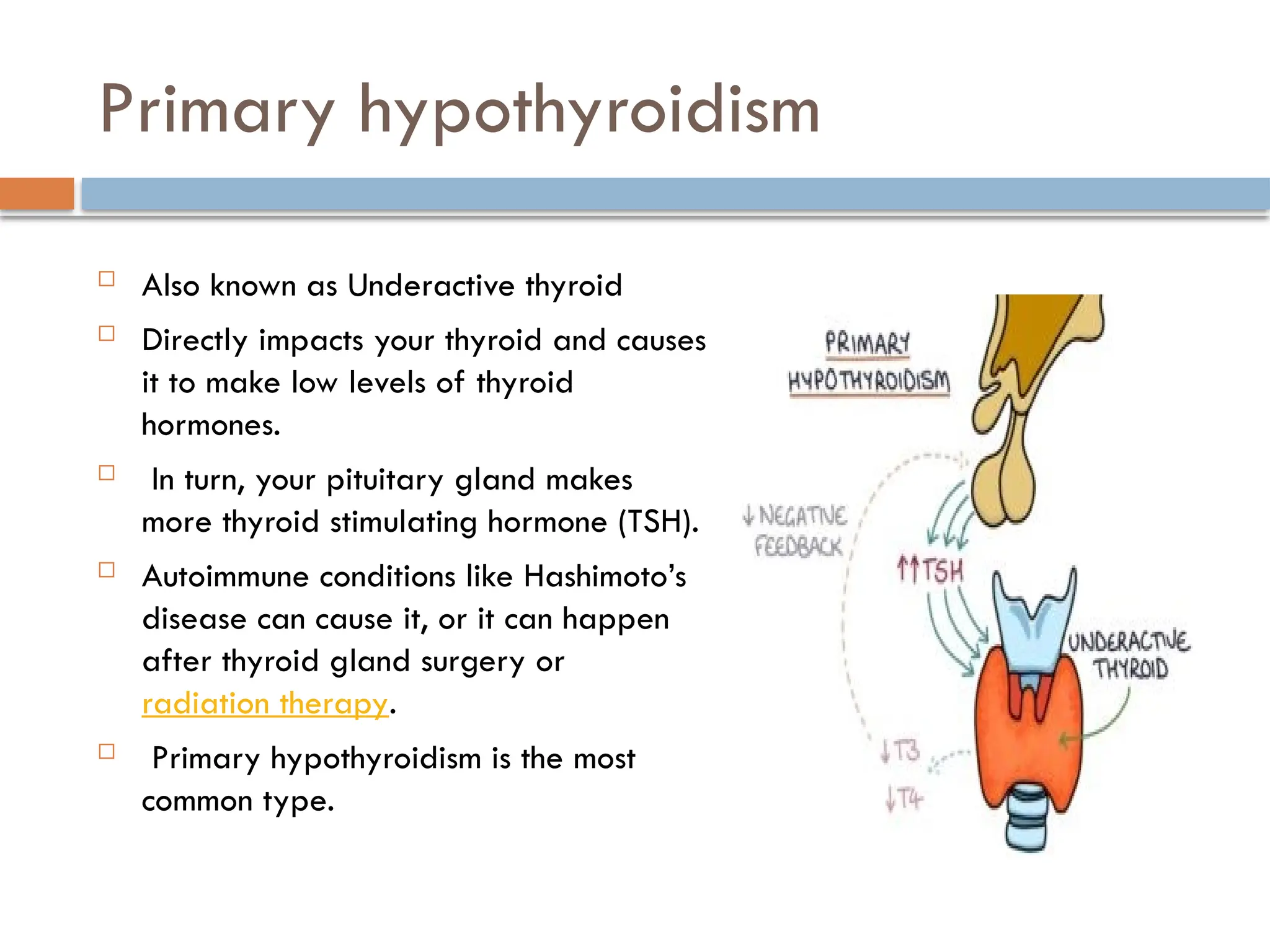
Hypothyroidism is a disorder where the thyroid gland fails to produce adequate hormones, leading to symptoms such as weight gain, fatigue, and metabolic slowdown. It is most commonly caused by Hashimoto's disease and can affect anyone, particularly those assigned female at birth over age 60. Diagnosis involves checking hormone levels, and treatment typically includes hormone replacement therapy to manage the condition effectively.