Downloaded 357 times
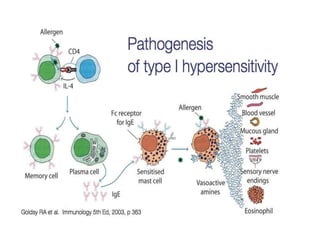
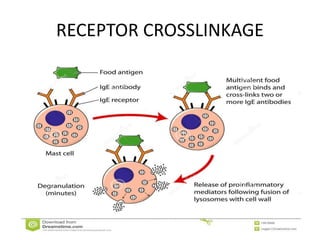
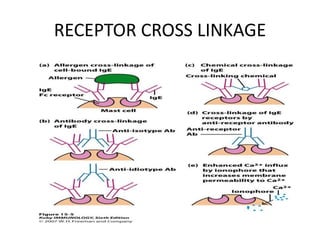
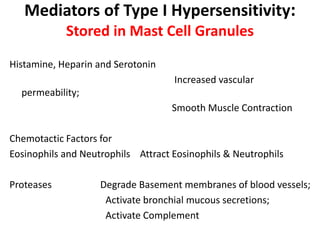
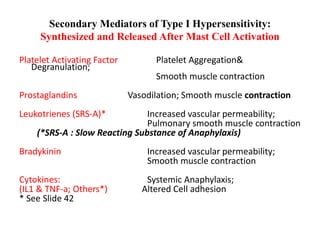
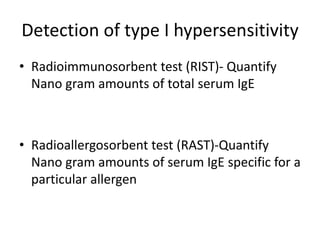
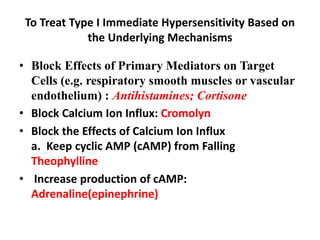
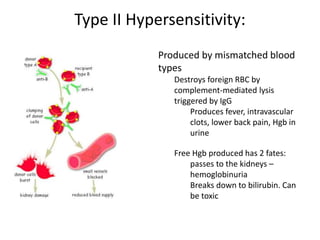


This document discusses hypersensitivity reactions of types I and II. It defines hypersensitivity as undesirable immune responses that can cause tissue damage or death. Type I reactions are immediate and IgE-mediated, involving mast cell degranulation. Common allergens are listed. Type II reactions are antibody-mediated and cytotoxic, destroying cells through complement activation or antibody-dependent cellular cytotoxicity. Examples given include blood transfusion reactions and hemolytic disease of the newborn. The mechanisms, mediators, treatments, and tests related to types I and II hypersensitivity reactions are described in detail.































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

















