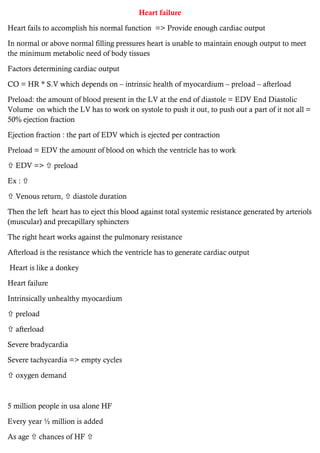
Heart failure occurs when the heart is unable to pump enough blood to meet the body's needs. It can be caused by an intrinsically unhealthy myocardium or factors that increase preload or afterload.
The body activates compensatory mechanisms like increasing sympathetic activity and renin-angiotensin-aldosterone system activity to increase cardiac output. However, over time these mechanisms cause remodeling of the myocardium and further reduce cardiac function, creating a vicious cycle. Prolonged compensatory mechanisms lead to chronic high preload and afterload, further damaging the myocardium and worsening heart failure over five years.




































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)












![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)



