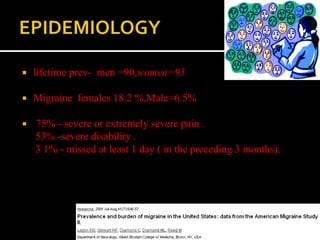
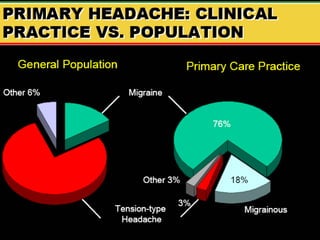
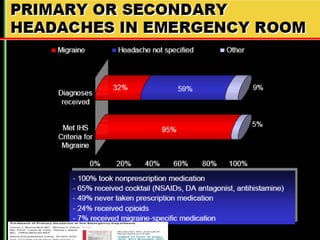
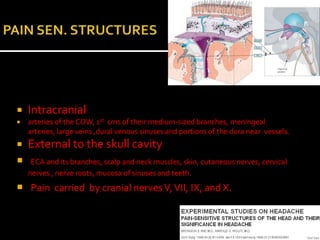
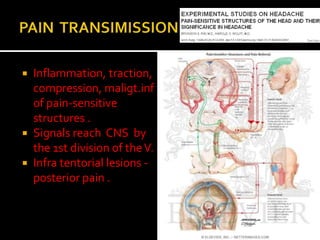
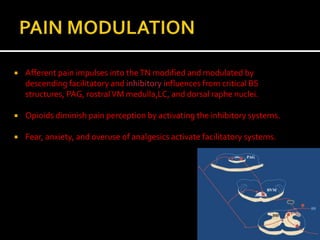
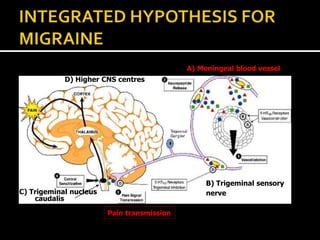
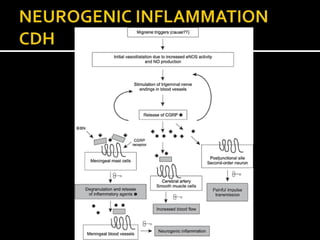
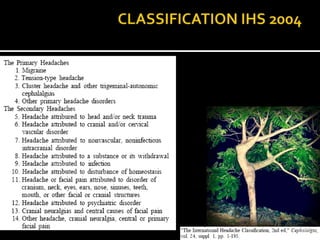

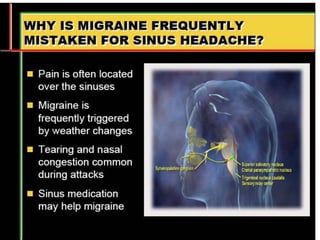
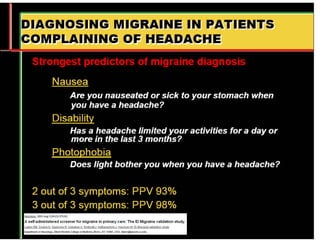

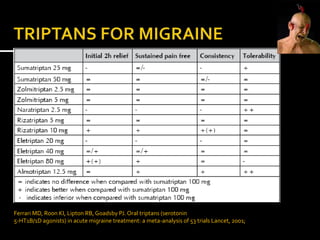

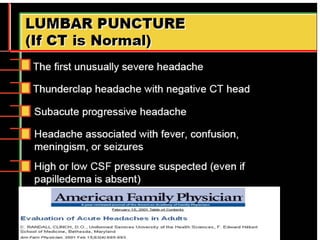


This document discusses migraine headaches. It notes that lifetime prevalence is around 90% for women and 95% for men. Migraines affect 18.2% of females and 6.5% of males. Three quarters of migraine sufferers experience severe or extremely severe pain, and over half experience severe disability, with 31% missing at least one day of work or school in the past three months. It then discusses anatomical structures involved in migraine pain transmission both inside and outside the skull. The document outlines several theories for migraine triggers and mechanisms of pain transmission and modulation in the central nervous system. It lists warning signs that could indicate an underlying condition is causing headache symptoms. Finally, it references a meta-analysis on the use of oral t





























































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




