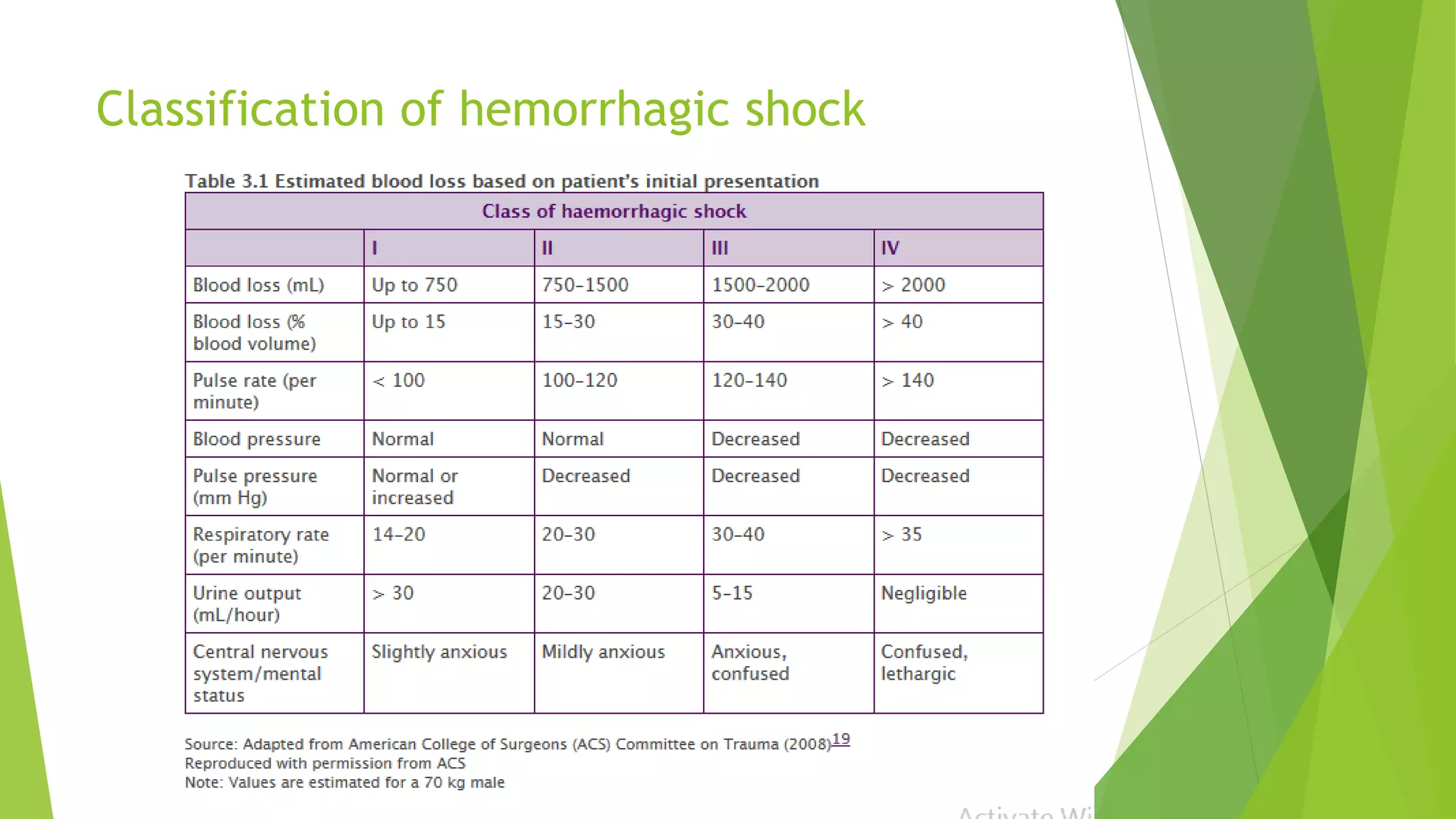
This document provides guidelines on managing massive blood transfusion. It defines major hemorrhage as loss of more than one blood volume within 24 hours or 50% of total blood volume lost within 3 hours. It recommends initiating a massive transfusion protocol for hemorrhagic shock classes 3 and 4, which follows a 1:1:1 ratio of packed red blood cells to fresh frozen plasma to platelets. It provides transfusion triggers based on lab values and outlines treatment with tranexamic acid and cautions on fluid resuscitation and electrolyte abnormalities during massive transfusion.