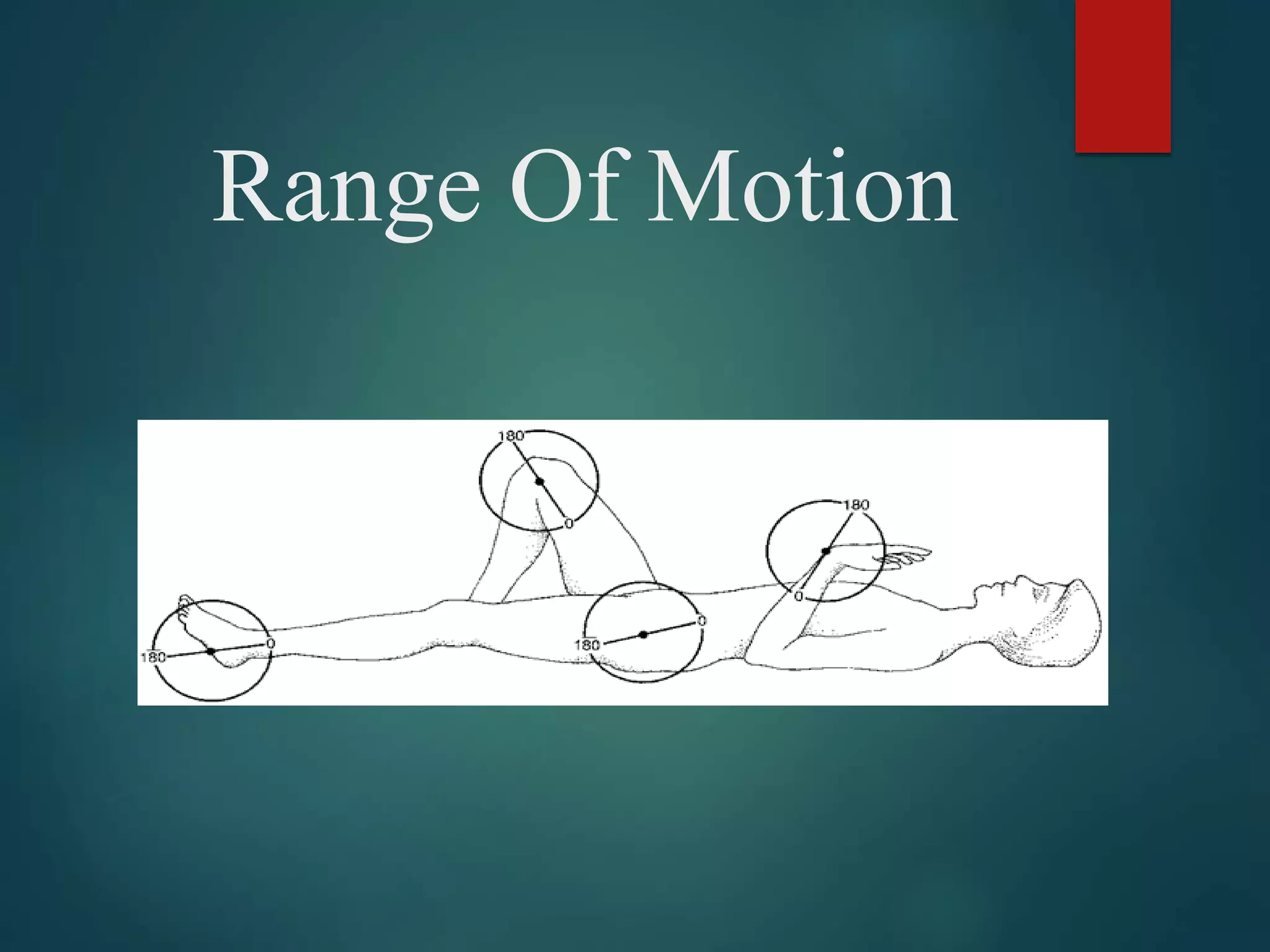
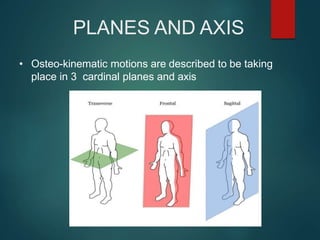
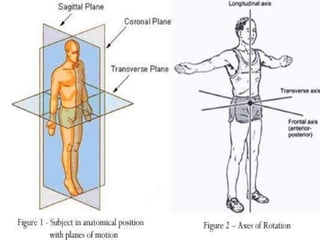
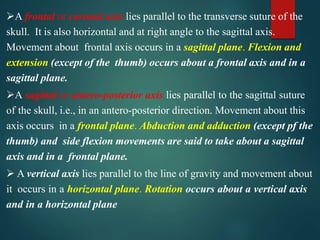
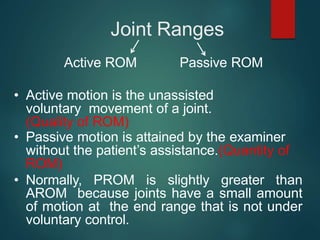
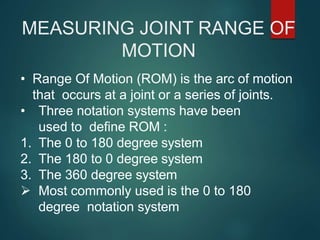
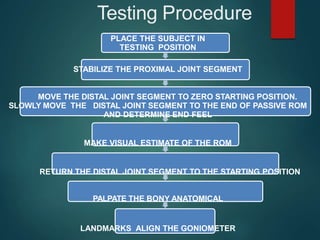
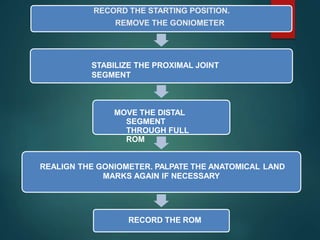
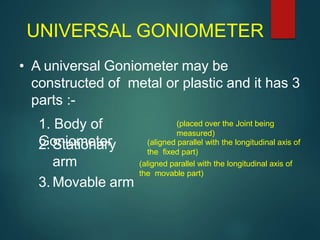
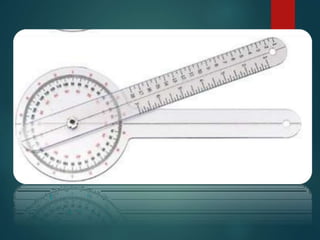
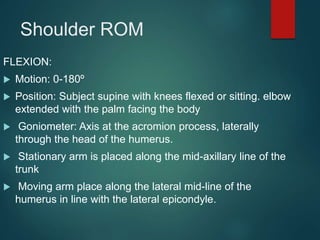
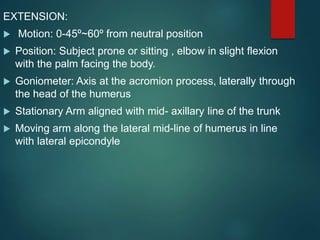
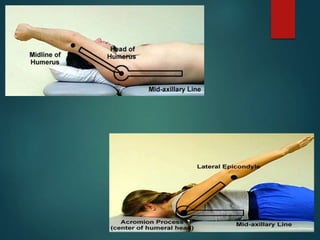
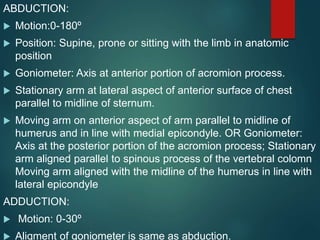
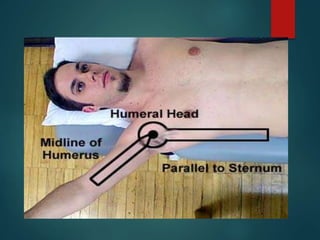
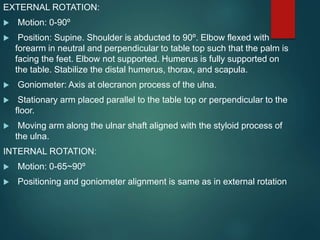
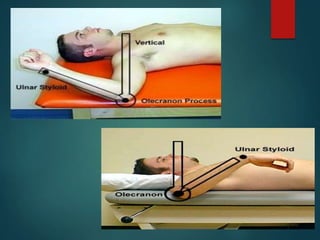
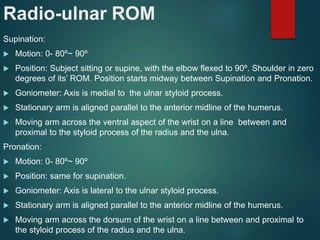
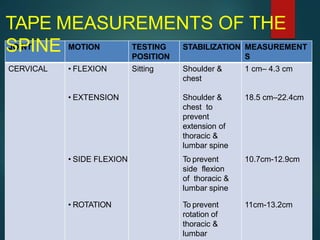
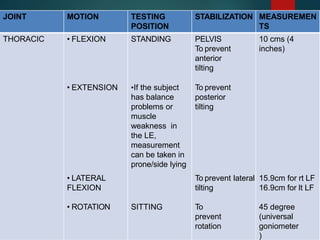
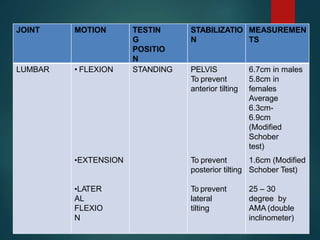
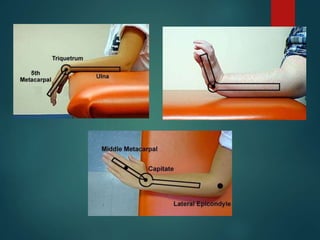
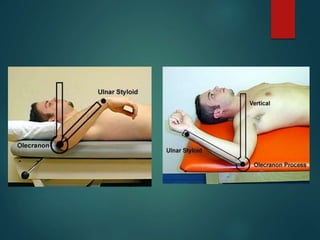
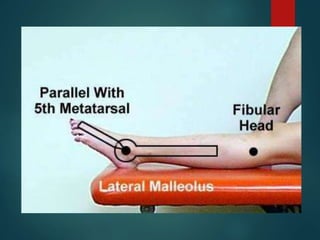
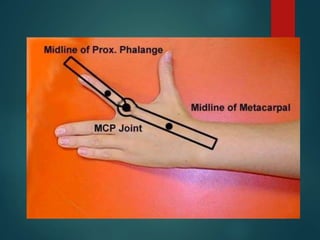
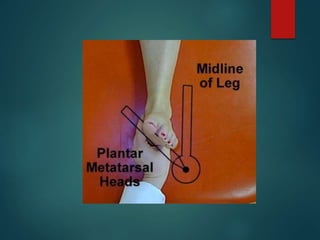
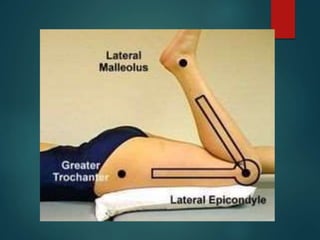
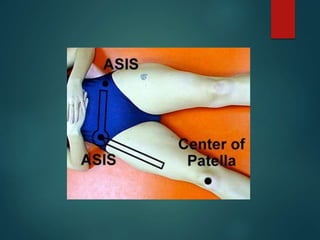
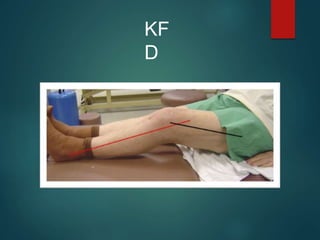
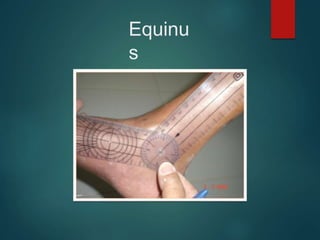
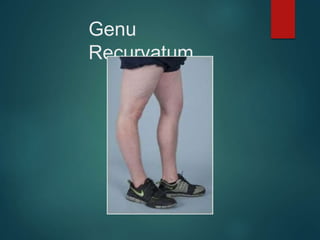
Range of motion (ROM) measurements are performed to evaluate joint impairment, develop treatment goals, assess progress, and modify treatment. ROM is described in 3 planes and axes and measured using a goniometer. Active ROM is voluntary motion while passive ROM uses external assistance. Several factors determine ROM including joint integrity, scarring, age, gender, joint shape, and health of surrounding tissues. Common causes of limited ROM include contractures, arthritis, and pain. Precise positioning and stabilization are needed to reliably measure ROM of various joints like the shoulder, spine, and knee. Standardized testing procedures and documentation of measurements are important.



















































![musculoskeletal_system_examination[1] (1) (3).pptx](https://cdn.slidesharecdn.com/ss_thumbnails/musculoskeletalsystemexamination113-241005064436-de0b77f1-thumbnail.jpg?width=640&height=640&fit=bounds)









![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)






