Downloaded 439 times
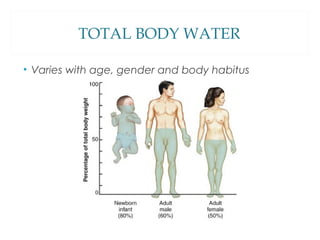
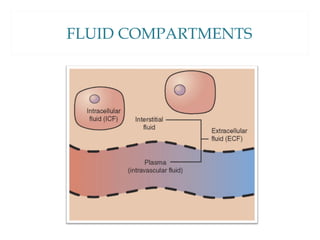
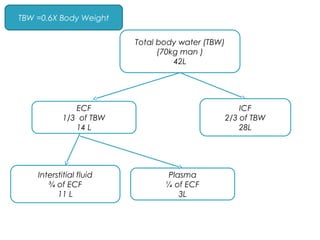
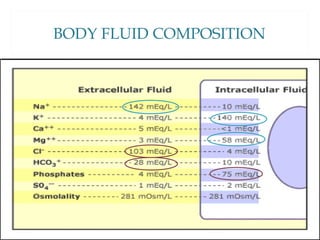
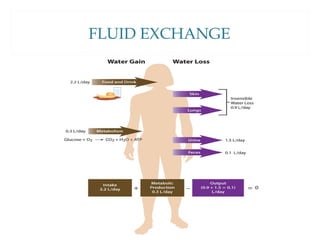
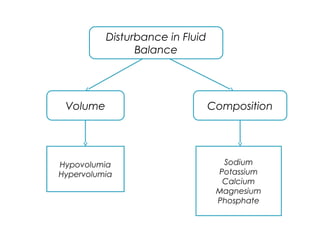
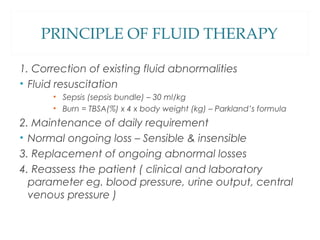
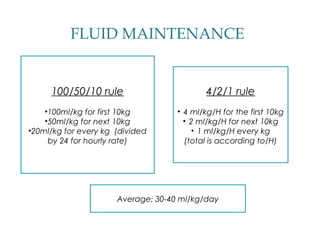
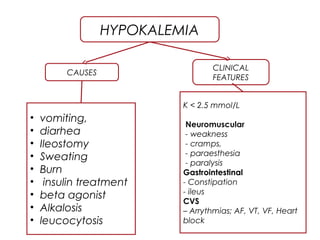
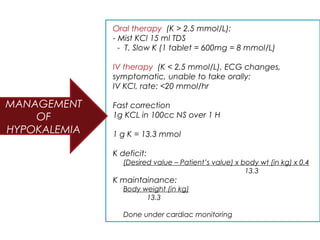
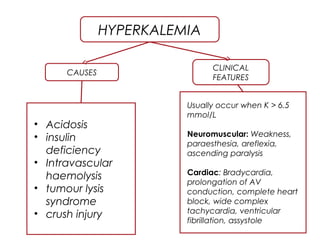
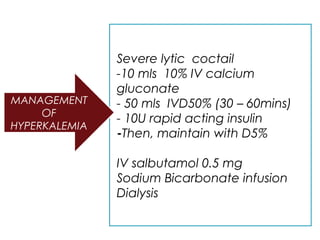
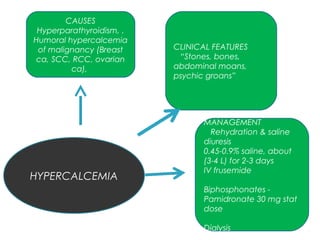

Dr. Mohd Anuar Bin Awang and Dr. Ainin Tasneem Bt Abdul Rafa presented on fluid and electrolyte balance. They discussed total body water distribution, fluid compartments, principles of fluid therapy, and common electrolyte imbalances including sodium, potassium, calcium, and their causes and management. Maintaining proper fluid and electrolyte balance is crucial as changes can occur due to surgery, trauma, or medical conditions and require careful monitoring and replacement as needed.























































































