Contents
Introduction
Types of Snakesin Nepal
Introduction to non-poisonous and poisonous snake
Identification of non-poisonous and poisonous snake
Sign and symptoms of poisonous and non- poisonous snake
bite
Diagnosis and First aid management
Antivenom treatment
Nursing Care
4.
Introduction
Snake bite isa life threatening and time limiting medical
emergency
89 species have been identified in Nepal
17 species of snake are found to be venomous
In Nepal, WHO estimates that 20,000 people are bitten by
snakes each year, resulting in over 1000 deaths
Snake bite commonly occurs in Terai districts during summer
and monsoon
5.
Snake of MedicalImportance
Poisonous
Non- Poisonous
● Ptyas mucosa – Rat Snake
● Checkered keelback- Paani Sarpa
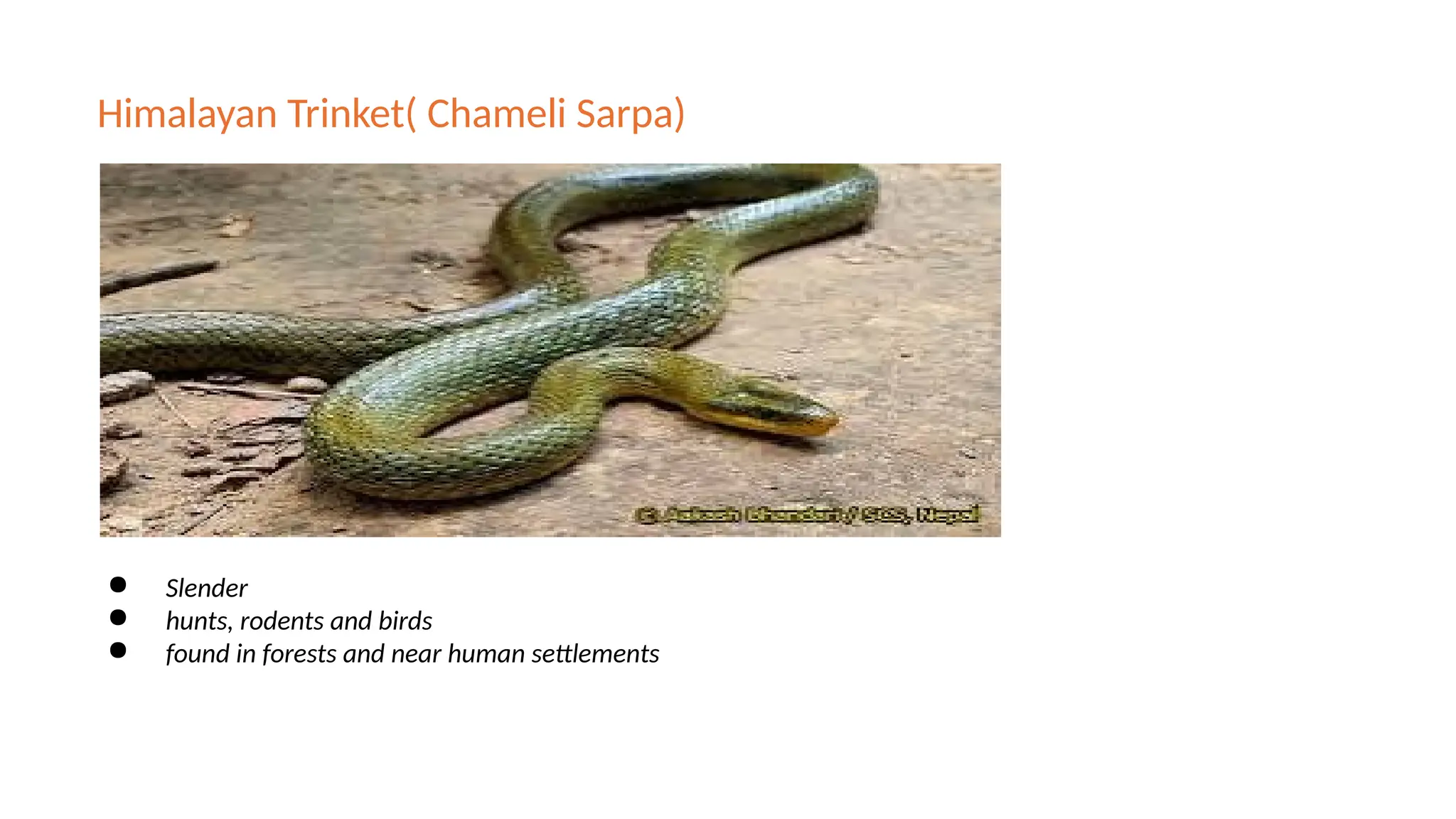
● Coelognathus helena – Common
Trinket Snake( Himalayan sarpa)
● Amphiesma stolatum – Buff-striped
Keelback
● Dendrelaphis tristis – Bronzeback
Tree Snake
Common Name Type of Venom
Common Krait Neurotoxic
Banded Krait Neurotoxic
Russell’s Viper Hematotoxic
Green Pit Viper Hematotoxic (mild)
Himalayan Pit Viper Hematotoxic (mild)
Features
No fangs orvenom glands,have small teeth instead
Rounded head(not triangular),no head neck
distinction
Round pupils
Double row of scales on the underside of tail
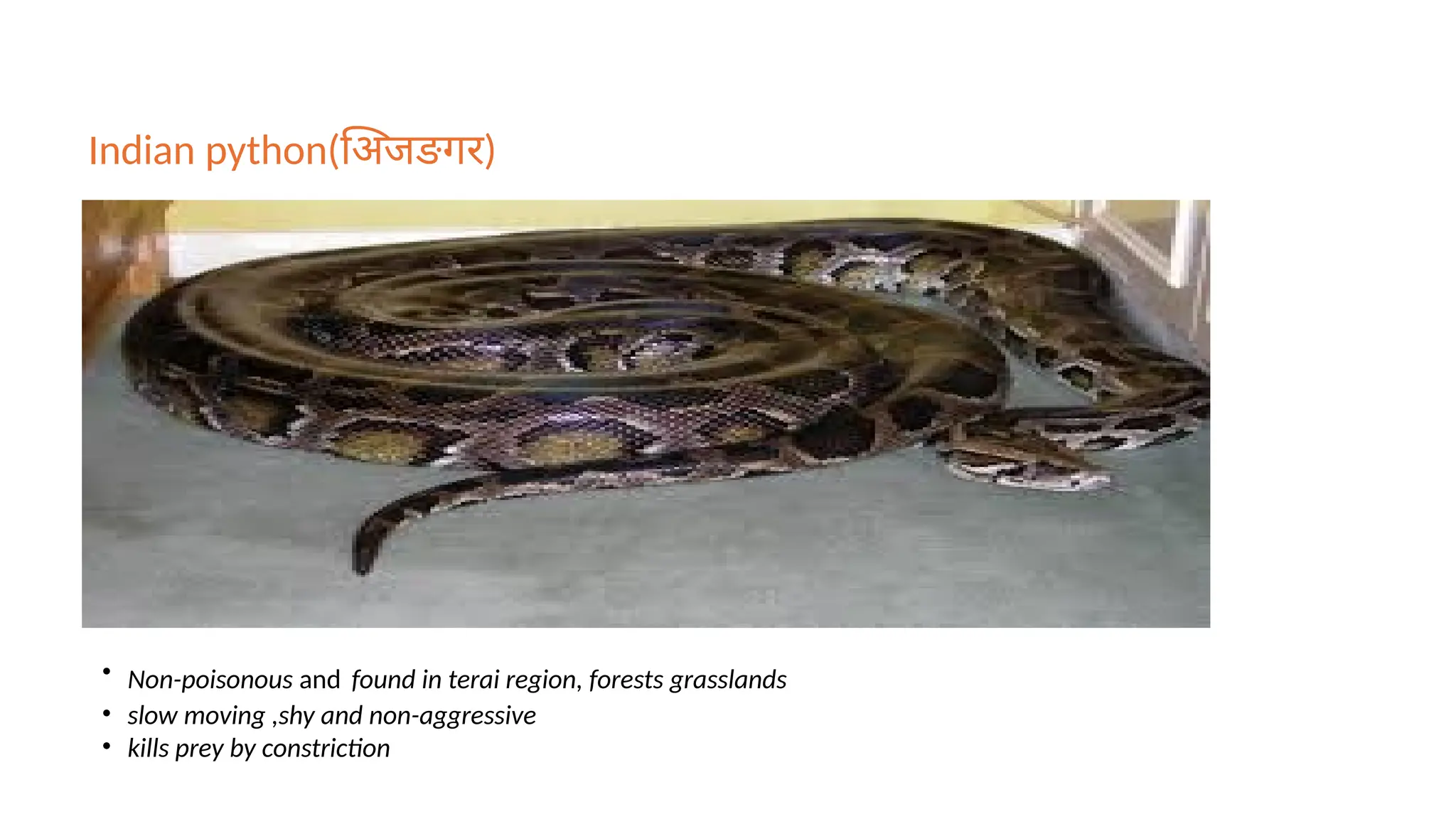
Indian python(अिजङगर)
• Non-poisonousand found in terai region, forests grasslands
• slow moving ,shy and non-aggressive
• kills prey by constriction
14.
Poisonous Snake
They canbe dangerous or
even life-threatening to
humans
Kill prey using venom –
neurotoxic, hemotoxic, or
cytotoxic
Often aggressive or defensive
when threatened
15.
Cont..
Have long, hollowfangs and
venom glands
Triangular head, distinct from
neck
Vertical slit pupils (like a cat)
Single row of scales on underside
of tail
16.
Common cobra(Goman, nag)
•Found in Terai region
• active during early morning and evening hours,
• warm and humid months (May to October)
17.
Krait
Common Krait(seto kalochure sarpa) Banded krait(laxmi sanp,pahelo kalo chure sarp)
• found mainly in the Terai region
• It is nocturnal and highly active at night.
Sign and symptomsof Non-
poisonous snake bite
◦ Local pain
◦ Swelling
◦ Redness
◦ Puncture/scratch marks
◦ No neurotoxic or hemotoxic symptoms
◦ Possible mild infection if untreated
Local effects
Cobra
• Swellingand local pain
with or without erythema
or discoloration at the bite
site.
• Blistering, bullae
formation and local
necrosis are also common.
• If it is infected, there may
be abscess formation.
Krait
• Usually do not cause signs
of local envenoming and
can be virtually painless.
Viper
• Swelling, blistering,
bleeding, and necrosis at
the bite site, sometimes
extending to the whole
limb.
• Persistent bleeding from
fang marks, wounds or
any injured parts of the
body.
• Swelling or tenderness of
regional lymph node.
23.
Systemic Manifestations
Hematotoxic
• Bleedingmay from
venipuncture site, gums,
• Epistaxis
• Hemoptysis
• Melena, rectal bleeding
• Hematuria, bleeding
from vagina
• Subconjunctival
hemorrhage
• Petechiae, purpura,
ecchymosis
Neurotoxic
• Ptosis
• Ophthalmoplegia
• Pupillary dilatation- often
non- responsive to light
• Inability (or limitation) to
open mouth
• Numbness around lips
and mouths
Neurotoxic
• Tongue extrusion-
inability to protrude the
tongue beyond incisors
teeth.
• Inability to swallow
• Broken neck sign
• Skeletal muscle
weakness.
• Loss of gag reflex
• Paradoxical breathing
• Respiratory failure
Diagnosis
Hematotoxic
•20-minute whole bloodclotting test (20WBCT)
•Bleeding time (BT) and clotting time (CT)
•Prothrombin time and International normalization ratio
(INR)
•fibrinogen, d-dimer
•Kidney function test and liver function test
•Complete blood count, blood group
•Urine for RBCs or myoglobin
•Creatine kinase
TREATMENT OF SNAKEBITE
ENVENOMING
Firstaid treatment and transport to the hospital
Rapid clinical assessment and resuscitation
Antivenom treatment
Supportive/ancillary treatment
Treatment of the bitten part
29.
Recommended First aidTreatment
REASSURANCE
• Most are nonvenomous snakes. Many are dry bites.
• Treatable condition.
IMMOBILIZAT
ION
• With a splint or sling.
• Pressure immobilization in case of purely neurotoxic snake bite
• Pressure pad immobilization
• Remove rings, jewelries, tight fittings and clothing
RAPID
TRANSPORT
• To decrease the delay in accessing the emergency care and reduce
mortility
30.
Rapid Clinical Assessmentand Resuscitation
A – Airway
• Check if the airway is clear and look for obstruction (especially in neurotoxic envenoming).
• Provide oxygen immediately using nasal prongs, catheter, or mask.
• Prepare for intubation if respiratory failure is present.
B – Breathing
• Assess the patient’s breathing rate and effort.
• Provide bag-mask ventilation if breathing is inadequate.
C – Circulation
• Monitor blood pressure and pulse.
• In cases like Russell’s viper bite, treat shock with:
• IV fluids (normal saline) ,Blood transfusion if bleeding.
31.
Cont..
D – Disability(Neurological status)
• Assess level of consciousness and neurological function.
• Look for signs of neurotoxicity: ptosis, paralysis, respiratory depression.
• Reassess regularly using a neurological scoring system if available.
E – Exposure & Environment
• Fully expose patient to examine bite site and swelling.
• Prevent hypothermia during examination.
• Observe for signs of systemic envenoming (bleeding, swelling, etc.)
32.
What to doand what not to do in snake bite
What To Do
• Reassure the patient
• Nil per mouth
• Remove shoes, rings, watches,
jewelleries,tight clothing at bitten area
• Leave blisters undisturbed
• Shift the victim to the nearest hospital ASAP
• Monitor closely and inform doctor about
sign and symptoms that were present
during transport
What Not To Do
• Cutting and sucking of bite site
• Application of various chemicals,
local remedies, cow dung
• Application of Tight Tourniquets
• Do not try to kill or capture the
snake(however if already killed
then should be taken to hospital
for identification)
Antivenom in Nepal
Importedfrom India and is Polyvalent
Anti-Snake Venom (ASV)
Effective against the four common
species of snakes;
Russell's Viper (Daboia russelii),
Common Cobra (Naja naja),
Common Krait (Bungarus caeruleus) and
Saw Scaled Viper (Echis carinatus).
35.
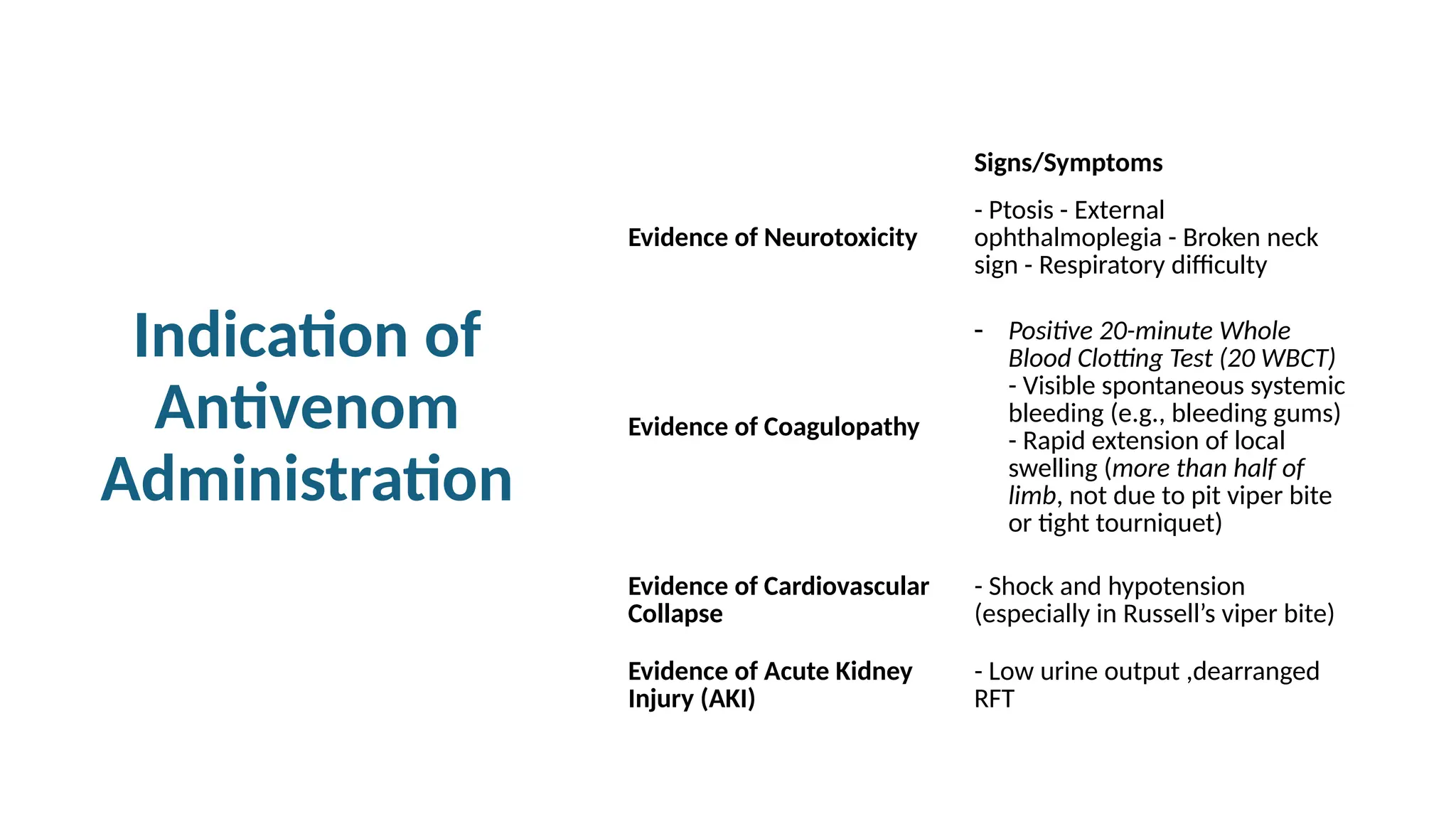
Indication of
Antivenom
Administration
Signs/Symptoms
Evidence ofNeurotoxicity
- Ptosis - External
ophthalmoplegia - Broken neck
sign - Respiratory difficulty
Evidence of Coagulopathy
- Positive 20-minute Whole
Blood Clotting Test (20 WBCT)
- Visible spontaneous systemic
bleeding (e.g., bleeding gums)
- Rapid extension of local
swelling (more than half of
limb, not due to pit viper bite
or tight tourniquet)
Evidence of Cardiovascular
Collapse
- Shock and hypotension
(especially in Russell’s viper bite)
Evidence of Acute Kidney
Injury (AKI)
- Low urine output ,dearranged
RFT
36.
Route of
Administration
Route PatientType Dilution Administration
Rate
Notes
IV Infusion Adult
5–10 ml/kg
body weight (≈
250–500 ml) of
isotonic saline
or glucose
Infusion at 2
ml/min
Most
commonly
used route
Children
3–5 ml/kg body
weight of
isotonic saline
or dextrose
water
Infusion at 2
ml/min
IV Injection Adult/Child
Reconstituted
antivenom (no
specific dilution
mentioned)
Slow IV at 2
ml/min
Rarely
practiced
Each vial is diluted with 10 ml. of sterile water as supplied with
the antivenom
37.
Antivenom Dose
Type ofEnvenoming Dose Dilution & Administration Repeat Dose Criteria
Neurotoxic Envenoming
Initial Dose: 10 vials (100
ml)
Dilute with 100–400 ml of
dextrose water or saline;
IV infusion at 2 ml/min
(over 40–60 min @ 60–70
drops/min)
Only if neurological signs
deteriorate (not just
persist); administer 5 vials
(50 ml) as IV push @ 2
ml/min
Hematotoxic Envenoming
(e.g., Russell’s viper)
Initial Dose: Same as
neurotoxic envenoming
(10 vials)
Same dilution and IV
infusion method
Repeat every 6 hours if
20WBCT or other
coagulation tests remain
abnormal; administer 5
vials (50 ml) as IV push @
2 ml/min
Pediatric Dose Same as adult dose
Snakes inject equal
venom regardless of age Same as adults
38.
Response to Treatment
◦General symptoms may disappear vary quickly.
◦ Spontaneous systemic bleeding usually stops within 15-30 min.
◦ Blood pressure may increase within 30-60 min.
◦ Neurotoxicity may improve as early as 30 min.
◦ Blood coagulability is usually restored in 3-9 hrs.
39.
Reasons for
failure to
respondto
antivenom
Excessive delay in administration of
antivenom
Patient with established respiratory
failure.
Insufficient dose of antivenom.
Inactive or poor quality antivenom.
Treatment of
the BittenPart
Elevation of limb with rest.
Simple washing with antiseptic solution like
chlorhexidine, povidone iodine etc.
Tetanus toxoid IM injection should be given. If patient
presents with coagulopathy, it should be postponed
until after resolution of coagulopathy.
In case of local necrosis and gangrene: Surgical
debridement.
Broad-spectrum antibiotic if features of infection.
42.
Prevention
of
Snakebite
Community based education.
Keephousehold clean by cutting grasses, bushes, and
plants, remove heaps of rubbish, building materials etc.
Bamboo, wood piles should be removed from
household so that snake cannot hide.
Close door, windows properly.
Try to avoid sleeping on floor.
Keep your granary away from the house, it may attract
rodents that snakes will hunt
43.
Cont..
Use high shoesor boots while walking in paddy field,
bushes, long grasses.
In dark, use light or strike the path using stick.
Never play with snakes or irritate them even if they are
dead. Never provoke them, they usually do not bite if
not irritated or provoked.
Never insert hands into long grasses, tree holes or mud
holes. Take care while pulling straw.
Shoes and cloths should be check before wearing, in an
area where snakes are abundant
44.
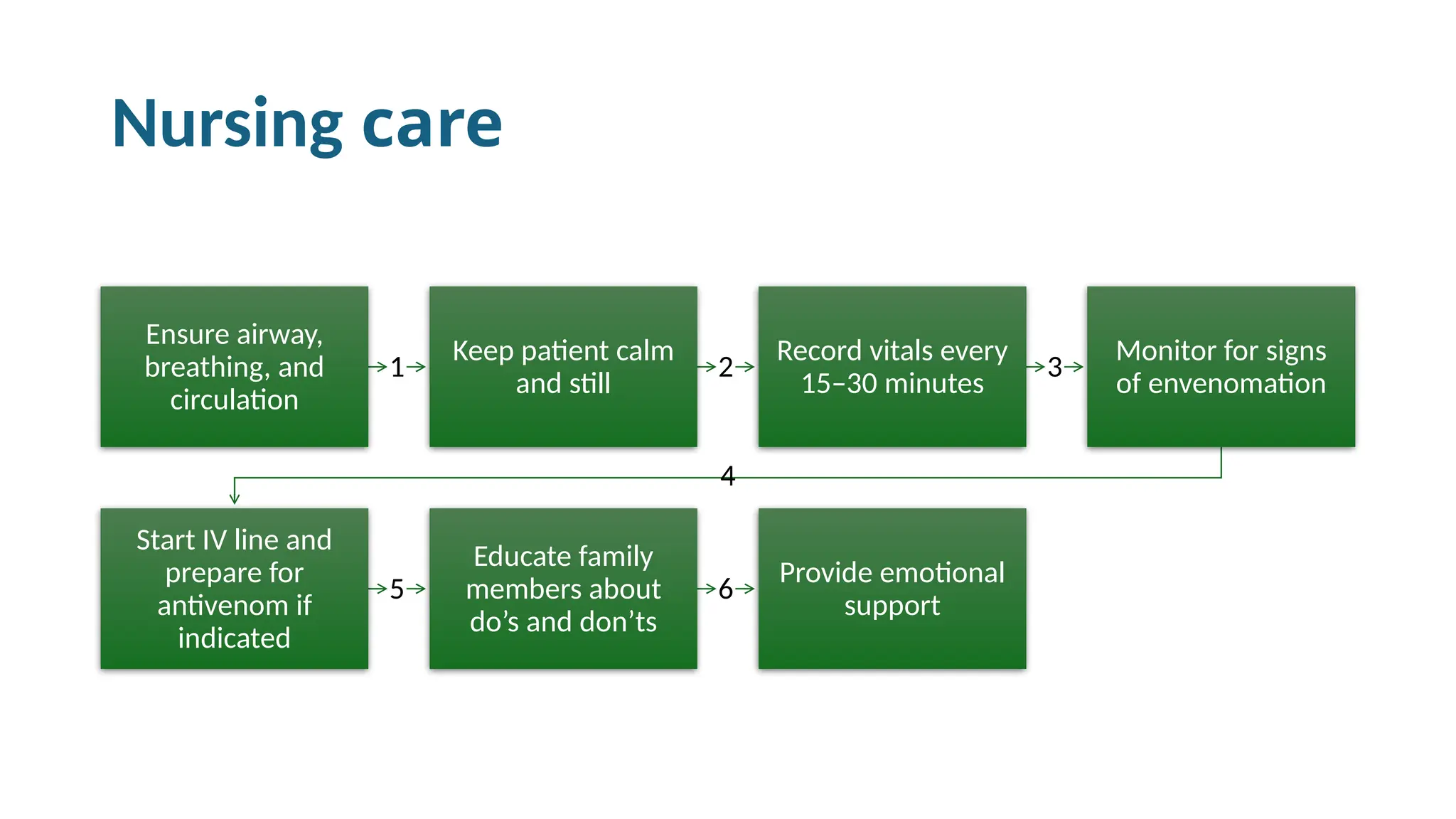
Nursing care
1
Ensure airway,
breathing,and
circulation
2
Keep patient calm
and still
3
Record vitals every
15–30 minutes
4
Monitor for signs
of envenomation
5
Start IV line and
prepare for
antivenom if
indicated
6
Educate family
members about
do’s and don’ts
Provide emotional
support
45.
References
• Epidemiology andDisease Control Division. (2016). National guideline for
snakebite management in Nepal. Ministry of Health, Government of Nepal.
• World Health Organization, Regional Office for South-East Asia. (2016). Guidelines
for the management of snakebites (2nd ed.). WHO Regional Office for South-East
Asia.
Editor's Notes
#9 Seen in village and farmland
Eats frogs and small birds
Often mistaken for cobra due to its size and holding behavior
#10 common near rivers, ponds and rice field
feeds on fish and frogs
#11 slender
hunts, rodents and birds
found in forests and near human settlements
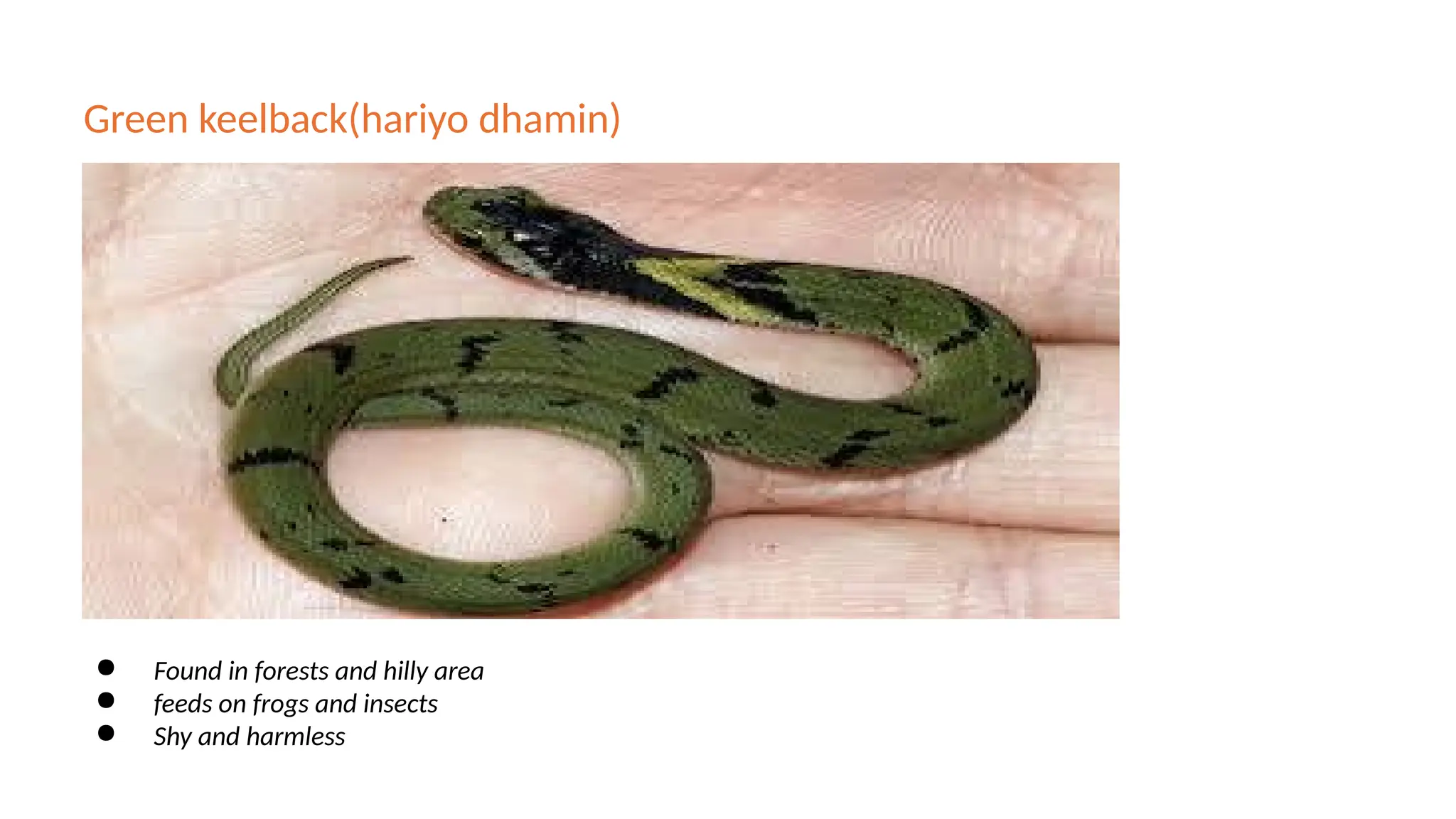
#12 Found in forests and hilly area
feeds on frogs and insects
Shy and harmless
#13 Non-poisonous
found in terai region, forests grasslands
slow moving ,shy and non-aggressive
kills prey by constriction
#16 Found in terai region
active during early morning and evening hours, especially in the warm and humid months (May to October)