Emotional quality of life in boys and girls with asthma 10 to 13 years of age
•
0 likes•190 views

The document discusses the benefits of meditation for reducing stress and anxiety. Regular meditation practice can help calm the mind and body by lowering heart rate and blood pressure. Studies have shown that meditating for just 10-20 minutes per day can have significant positive impacts on both mental and physical health over time.

Recommended
More Related Content
More from Center for Managing Chronic Disease
More from Center for Managing Chronic Disease (20)
Emotional quality of life in boys and girls with asthma 10 to 13 years of age
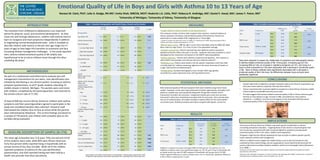
- 1. Emotional Quality of Life in Boys and Girls with Asthma 10 to 13 Years of Age Noreen M. Clark, PhD1; Julie A. Dodge, RN MS1; Smita Shah, MBChB, MCH2; Roderick J.A. Little, PhD1; Rebecca R. Andridge, MS1; Daniel F. Awad, MA1; James Y. Paton, MD3 1University of Michigan, 2University of Sidney, 3University of Glasgow Table 1. Baseline Demographics and Health Status, Overall and by Gender Table 3.Variables Associated with Emotional QL, by Gender INTRODUCTION MEASURES P-Value Overall Males Females (N=776) (N=392) (N=384) p-value* Difference in by P-value The transition from childhood to adolescence is an important •Juniper Pediatric Asthma Quality of Life Questionnaire*: Effect Comparison EQL gender Boys vs Girls Demographics This measure contains 23 items that comprise three domains: activity limitation (5 period for physical, social, and emotional development. As they Age +1 year Boys -0.08 0.49 0.16 items); symptoms (10 items); and emotional quality of life (8 items). Results are move into and through adolescence, children with asthma need to Age (Mean, SD) 11.6 (0.6) 11.7 (0.7) 11.6 (0.6) 0.02 Girls -0.31 0.02 expressed as a mean quality of life ranging from 1‐7 (low‐high). learn to recognize and treat symptoms independently in addition African-American Race 744 (96%) 374 (95%) 370 (96%) 0.71 * Juniper EF, Guyatt, GH, Feeny, DH, Ferrie, PJ, Griffith, LE, Townshend, M. (1995). Measuring quality of life in BMI Z-score +1 unit Boys -0.06 0.28 0.42 to negotiating normal developmental tasks. Little is available to Parent Education children with asthma. Quality of Life Research: 5; 35‐46. Girls -0.13 0.04 describe children with asthma in the pre teen age range (10‐13 •BMI‐for‐age Z‐scores: BMI‐for‐age Z‐scores were calculated using the 2000 CDC Body Yearly Income <$15K vs >$15K Boys -0.23 0.13 Less than High School 142 (18%) 77 (20%) 65 (17%) 0.58 Mass Index‐For‐Age Charts. A Z‐score of zero is the population average. 0.78 years of age) as they begin this transition to autonomy and face Girls -0.28 0.06 •Symptom Assessment: Parents reported day and nighttime asthma symptoms increasing disease management challenges. In the study reported High School graduate 280 (36%) 141 (36%) 139 (36%) experienced by the child in the past 12 months. Symptom data were provided in a form Symptom Nights 50% increase Boys -0.01 0.40 0.24 here, asthma related emotional quality of life (EQOL) was More than High School 354 (46%) 174 (44%) 180 (47%) developed by the researchers and based on the NAEPP national guidelines. Girls -0.04 0.01 hypothesized to be at risk as children move through this often •Asthma Diagnosis: Parents were asked to respond to the question, "Has a doctor or Household Income unsettling life phase. other health care provider ever told you that your child has asthma?" Data were analyzed to assess the relationship of symptoms and demographic factors < $15,000 349 (45%) 166 (42%) 183 (48%) 0.01 •Medication Use: Parents were asked to list the specific medications that their child to asthma-related emotional quality of life. Among girls, increasing age (p=.02), currently takes for "asthma, wheezing, tightness in the chest, shortness of breath, or increasing BMI (p=.04), an increase in nighttime symptoms (p=.01), and living in a $15,000-$40,000 315 (41%) 159 (41%) 156 (41%) cough" and the form of administration. lower income household (p=.06) were associated with a decrease in emotional quality > $40,000 112 (14%) 67 (17%) 45 (12%) •Demographics: Standard demographic items include child's age, gender, of life. None of these variables were significantly associated with a decrease in METHODOLOGY race/ethnicity, parent education level, and household income. emotional quality of life in the boys. No differences between boys and girls were Health statistically significant. •As part of a randomized controlled trial to evaluate two self‐ BMI-for-age Z-score (Mean, SD) 1.1 (1.3) 1.0 (1.3) 1.1 (1.2) management interventions for pre‐teens, case identification was Quality of Life, Emotions CONCLUSIONS initiated by distributing a recruitment packet, including an asthma (Mean, SD) 5.3 (1.5) 5.3 (1.5) 5.2 (1.5) STATISTICAL METHODS • Despite high levels of nighttime symptom frequency about one‐third of respondents say symptom questionnaire, to all 6th grade students attending 19 Asthma Status they were never told by a physician that they have asthma. Asthma Symptom Days, middle schools in Detroit, Michigan. The packets were sent home past year Both emotional quality of life and symptom level were modeled using linear mixed • Factors associated with increased nighttime symptoms in these African American middle models. Symptom counts were log‐transformed to better approximate normality. Each with children, completed by the parent/guardian, and returned to None 82 (11%) 39 (10%) 43 (11%) school students include BMI and very low income. predictor variable was used separately (along with the gender indicator and its the schools (return rate of 71.3%). interaction) to predict the outcomes. Unadjusted models were used since we were • The data suggest that asthma related emotional quality of life in African American girls 1 - 12 days 149 (19%) 67 (17%) 82 (21%) declines as they advance in age, increase in BMI, and experience more asthma interested in what was univariately associated with the outcomes. Since schools were 13 - 52 days 206 (27%) 111 (28%) 95 (25%) the unit of randomization, all models included a random effect for the school within symptoms. In addition, very low income appears to be associated with decreased •A total of 906 low income African American children with asthma recruitment year. Statistical analyses were done using the SAS System, version 9.1. emotional quality of life in these preteen girls with asthma. symptoms and their parent/guardians agreed to participate in the 53 - 365 days 208 (27%) 105 (27%) 103 (27%) study and completed baseline data collection. Research staff > 365 days 131 (17%) 70 (18%) 61 (16%) Asthma Symptom Nights, interviewed the children face‐to‐face at school while the parents past year were interviewed by telephone. The current findings are based on a sample of 776 parents and children with complete data on the RESULTS None 150 (20%) 70 (18%) 80 (21%) 0.12 variables being evaluated. 1 - 12 nights 202 (27%) 97 (25%) 105 (27%) Table 2. Variables Associated with Nighttime Symptoms, by Gender IMPLICATIONS 13 - 52 nights 167 (22%) 103 (26%) 64 (24%) % Increase in P-Value P-value Effect Comparison Symptoms by gender Boys vs Girls •Low‐income African‐American children may need special consideration in asthma 53 – 365 nights 146 (20%) 78 (20%) 68 (18%) Age +1 year Boys -2% 0.90 counseling and patient education. Targeting those of low income is important given that 0.45 low income was associated with both increased nighttime symptoms and decreased > 365 nights 81 (11%) 44 (11%) 37 (10%) BASELINE DESCRIPTION OF SAMPLE (N=776) Ever Diagnosed with Girls 17% 0.38 emotional quality of life in this urban, middle school population. Asthma 477 (62%) 260 (66%) 217 (57%) 0.01 BMI Z-score +1 unit Boys 20% 0.02 0.71 •Programs might also be offered separately for boys and girls to address gender‐specific The mean age at baseline was 11.6 years. Fifty‐one percent (51%) Uses a Bronchodilator 415 (54%) 230 (59%) 185 (49%) 0.003 Girls 26% 0.01 issues related to asthma self‐management. of the students were male, while 96% were African‐American. Yearly Income <$15K vs >$15K Boys 11% 0.62 •Efforts to address excess weight and related factors such as diet and activity are also Uses an Anti-Inflammatory 160 (21%) 98 (25%) 62 (16%) 0.002 0.16 indicated by these study findings and are supported by recent data that demonstrate the Forty‐five percent (45%) reported living in households with an Girls 67% 0.01 poorly understood association between pediatric asthma and overweight status (Abramson, annual income of less than $15,000. While all of the children Uses No Asthma Meds 344 (45%) 151 (39%) 193 (51%) 0.001 Nighttime symptoms increased with higher BMI for both girls (p=.02) and boys (p=.01). et al, 2008). * reported symptoms of asthma on the case identification None 150 (20%) 70 (18%) 80 (21%) 0.12 Nighttime symptom counts were significantly higher (p=.01) for girls living in households with Actions such as these may improve the symptom experience and emotional quality of life of early adolescent children, especially girls, with asthma. questionnaire, only 62% reported having ever been told by a an annual income less than $15,000 compared to households with income above $15,000. All percentages use the number of valid responses as the denominator. Valid percentages range from 96 to 100%. Despite apparent differences in point estimates there were no statistically significant differences *Abramson, NW, Wamboldt, FS, Mansell, AL, Carter, R, Federico, MJ, Wamboldt, MZ. (2008). Frequency and correlates of health care provider that they had asthma. *Comparisons made using linear and non-linear mixed models with a random effect for the school within cohort. in these effects comparing boys to girls. overweight status in adolescent asthma. Journal of Asthma: 45; 135‐139.