- Dr. Tamagnsew presented a seminar on the management of digitalis toxicity. The presentation covered the mechanism of action, pharmacokinetics, signs and symptoms, and management of digitalis toxicity.
- Digitalis toxicity can cause a variety of cardiac arrhythmias and other symptoms. Diagnosis involves physical exam, ECG, lab tests including serum digoxin level.
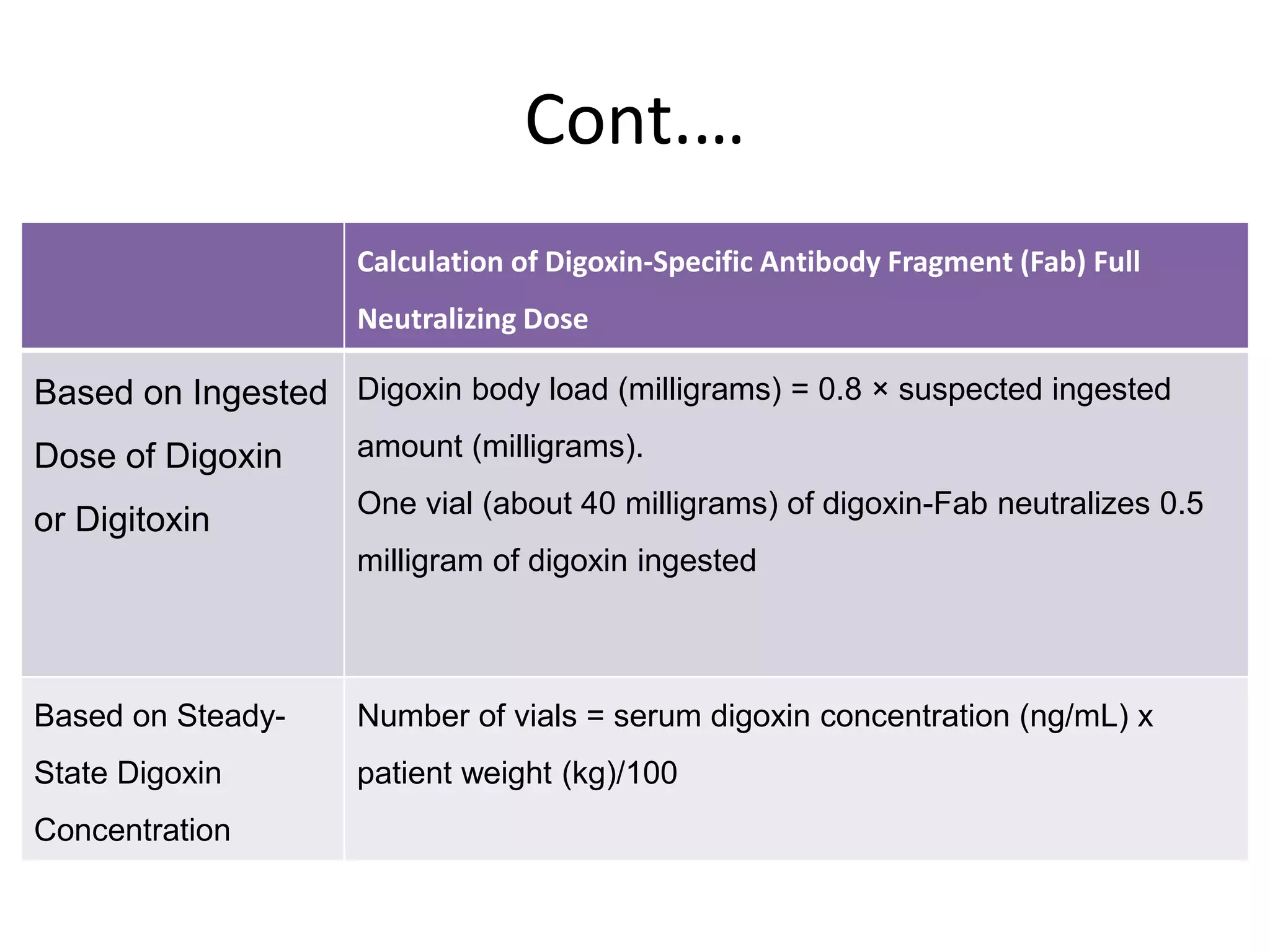
- Treatment focuses on preventing further absorption, enhancing elimination, and administering digoxin antibody fragments (digibind) based on ingested dose or serum level to neutralize digoxin effects for life-threatening arrhythmias or end-organ toxicity.