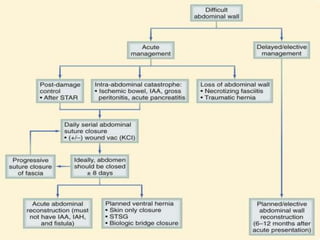
The document discusses difficult abdominal wall closure, techniques for temporary abdominal closure, and definitive abdominal wall reconstruction. It provides details on:
- Ideal suture materials that resist infection and provide strength for closure.
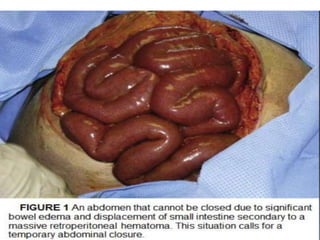
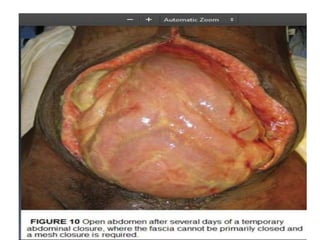
- Indications for leaving the abdomen open such as damage control surgery or intra-abdominal hypertension.
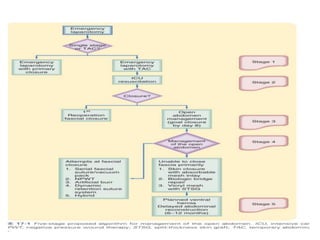
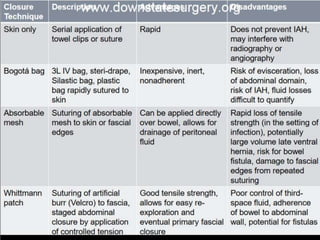
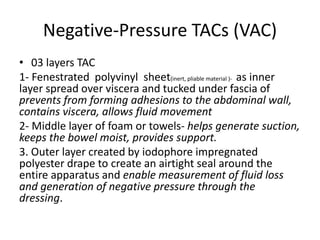
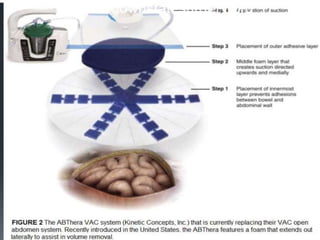
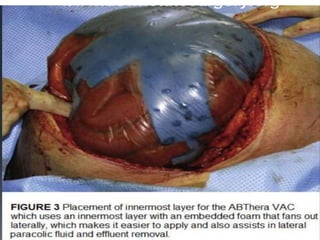
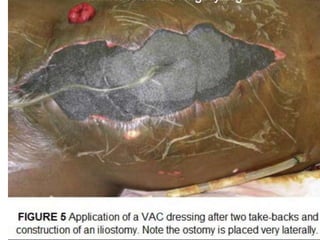
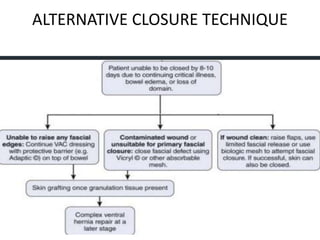
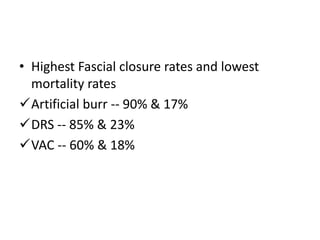
- Temporary abdominal closure techniques including negative pressure devices that control fluids and promote primary fascial closure in 70-80% of cases.
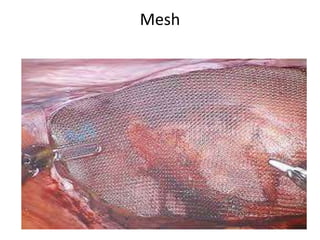
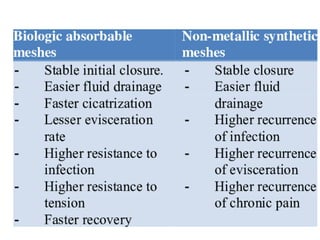
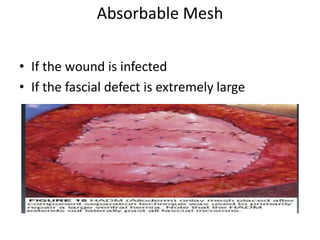
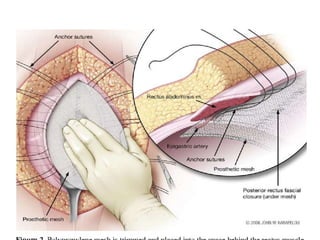
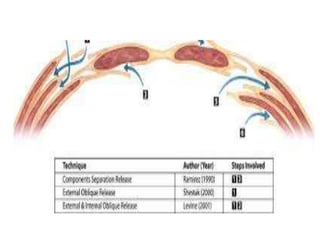
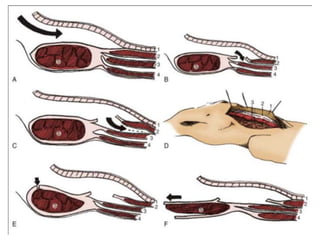
- Factors to consider before definitive reconstruction such as optimizing patient status and using tension-free techniques like component separation with mesh reinforcement for a durable repair.






































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)










