creat 60 slides from the pdf , for acadamic presentation for urology resident , include images from standard urology books and mention video links from youtube to be included in the slides
creat 60 slides from the pdf , for acadamic presentation for urology resident , include images from standard urology books and mention video links from youtube to be included in the slides
Similar to creat 60 slides from the pdf , for acadamic presentation for urology resident , include images from standard urology books and mention video links from youtube to be included in the slides
creat 60 slides from the pdf , for acadamic presentation for urology resident , include images from standard urology books and mention video links from youtube to be included in the slides
1.
Approach to
pathology, diagnosis
andstaging of
testicular tumor
Presenter - Dr . Hawi D (USRIII)
Moderator - Dr. Fitsum (Consultant
urologist)
12/14/2025
1
Introduction
• Morphologically andclinically diverse group of tumors,
more than 95% are germ cell tumors (GCTs).
• GCTs are broadly categorized as seminoma and
nonseminoma (NSGCT)
• GCT is a relatively rare malignancy,
• 1% to 2% of cancers among adult males in the United
States.
• Approximately 95% of GCTs arise in the testis, and 5% are
extragondal in origin.
• GCTs - curable neoplasm (metastatic GCT is 80-90%)
12/14/2025 4
5.
Epidemiology
• Most commonmalignancy among males aged 20 to 40
years.
• The incidence rate rises rapidly after puberty, peaking 25
- 35
• The incidence of bilateral GCT is approximately 2%.
- Majority Metachronous
- Over an average interval of 5 years
- Discordant histology occurs in 30% to 50%
12/14/2025 5
6.
Epidemiology…
• Highest inScandinavia, Western Europe, and
Australia/New Zealand
• lowest in Africa and Asia.
• The incidence of GCT appears to be increasing
worldwide.
• Only about 13% of males present with distant
metastatic disease.
12/14/2025 6
7.
Risk factors
Five wellestablished risk factors
1. White race
2. Cryptorchidism ( 4-6 x more likely to be dx with testis
cancer, 2-3 x if orchidopexy is performed before puberty).
3. Family history of testis cancer
4. Personal history of testis cancer – 12-fold increased risk
of developing GCT in the contralateral testis
5. Germ cell neoplasia in situ (GCNIS)/intratubular germ cell
neoplasia (ITGCN)
• Subfertility and infertile
• Diet and/or environmental factors
12/14/2025 7
8.
Histologic classification
• GCNIS-derivedand non-GCNIS–derived.
• Majority of postpubertal GCTs are GCNIS-derived.
• GCNIS- derived GCTs – seminoma (52-56%) and NSGCT(44-48%)
• NSGCTs include embryonal carcinoma (EC), yolk sac tumor, teratoma,
and choriocarcinoma subtypes, either alone(pure forms) or in
combination as mixed GCT with or without seminoma.
• Most NSGCTs are mixed tumors that are composed of two or more GCT
subtypes.
• GCTs that contain both NSGCT subtypes and seminoma are classified as
NSGCT even if component is a tiny proportion of the tumor.
12/14/2025 8
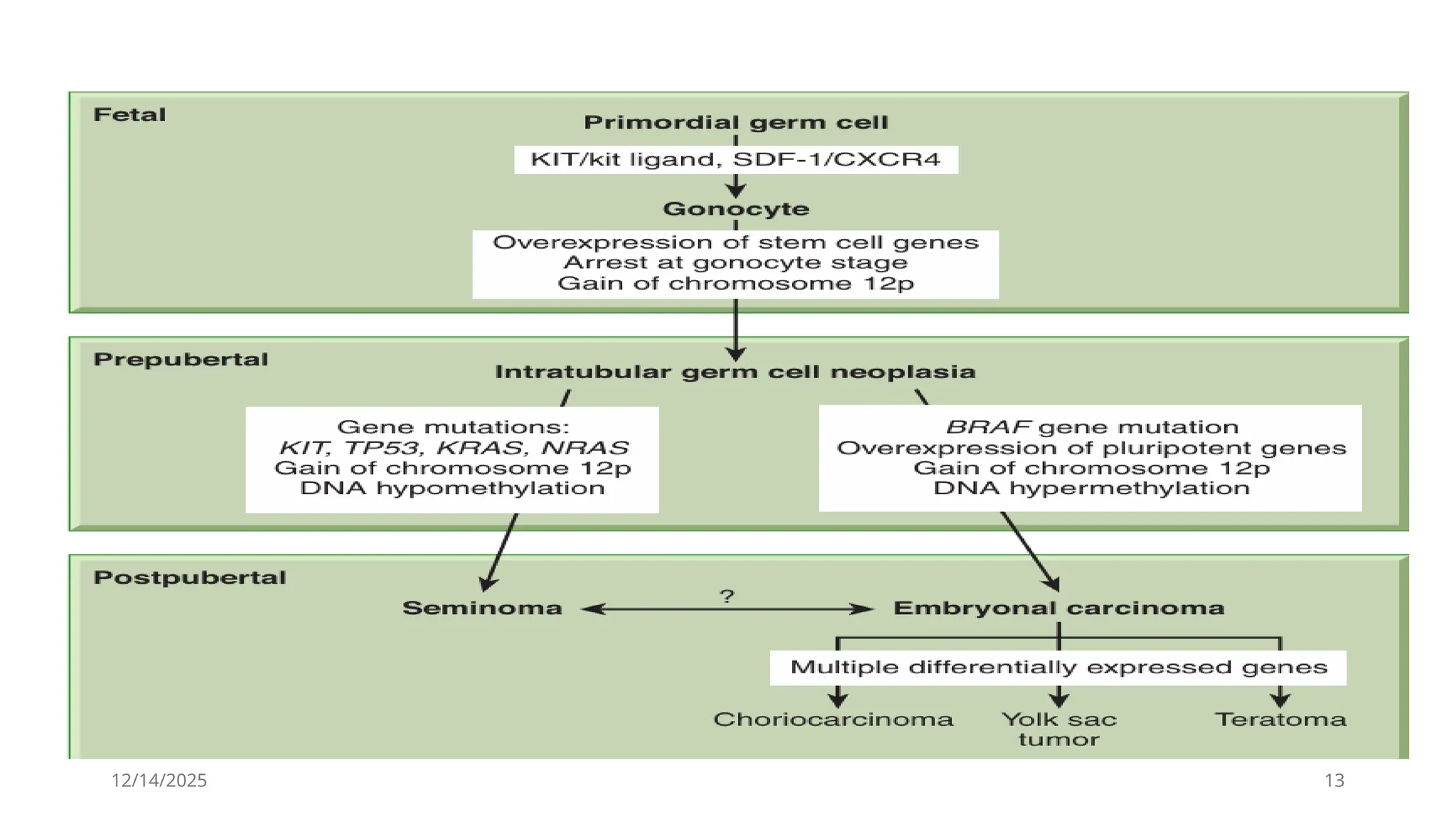
Pathogenesis
• Not welldefined /Poorly understood
• Transformed primordial germ cells that develop in
utero or early infancy.
• gonocytes that failed to differentiate into
prespermatogonia, that lay dormant until puberty
when they are stimulated by increased serum (LH)
and/or testosterone levels.
12/14/2025 11
12.
Pathogenesis…
• Additionally, polymorphismsof certain genes, including the
gene encoding c-KIT ligand, have been associated with an
increased risk of testis cancer.
• Gonocytes depend on KIT ligand for survival; the gene for
this protein is located on the long arm of chromosome 12,
where an increased number of copies is a universal finding
in adult GCT.
• Thus, a connection between mutations or polymorphisms in
c-KIT ligand and GCT has biological plausibility.
• Inherited alterations to susceptibility genes involved in DNA
repair may contribute to the development of adult GCT.
12/14/2025 12
12/14/2025 14
Pathogensis….
• Approximately5% of postpubertal GCTs are extragondal in origin,
- midline anatomic locations (retroperitoneum and mediastinum are most common).
first hypothesizes that
• they originate from germ cells that mis-migrated along the genital ridge and were able to
survive in an extragonadal environment.
The second theory
• reverse migration from the testis to extragonadal locations
• Primary mediastinal NSGCTs differ from those originating in the testis or
retroperitoneum.
• they are less sensitive to chemotherapy and have
• poor prognosis with a 5-year overall survival of about 45%
• likely to have yolk-sac-tumor components and thus to be associated with elevations in serum
α-fetoprotein (AFP)
They are also associated with Klinefelter syndrome and with hematologic malignancies that
carry extra copies of the short arm of chromosome 12, as seen in adult GCT
15.
12/14/2025 15
• Mediastinalseminomas carry a similar prognosis to
testicular seminomas, and
• Mature teratomas of the mediastinum have low metastatic
potential and can
• generally be cured surgically
• Primary retroperitoneal GCTs are indistinguishable
biologically from testicular GCTs and carry the same
prognosis.
16.
12/14/2025 16
GCNIS
• MostGCTs arise from ITGCN.(Except for spermatocytic seminoma in
adults and teratomas and yolk sac tumor in pediatric patients.)
• Characterized by proliferation of uncommitted neoplastic
germ cells within seminiferous tubules.
• Progress to GCT in ~50% of cases within 5 years.
17.
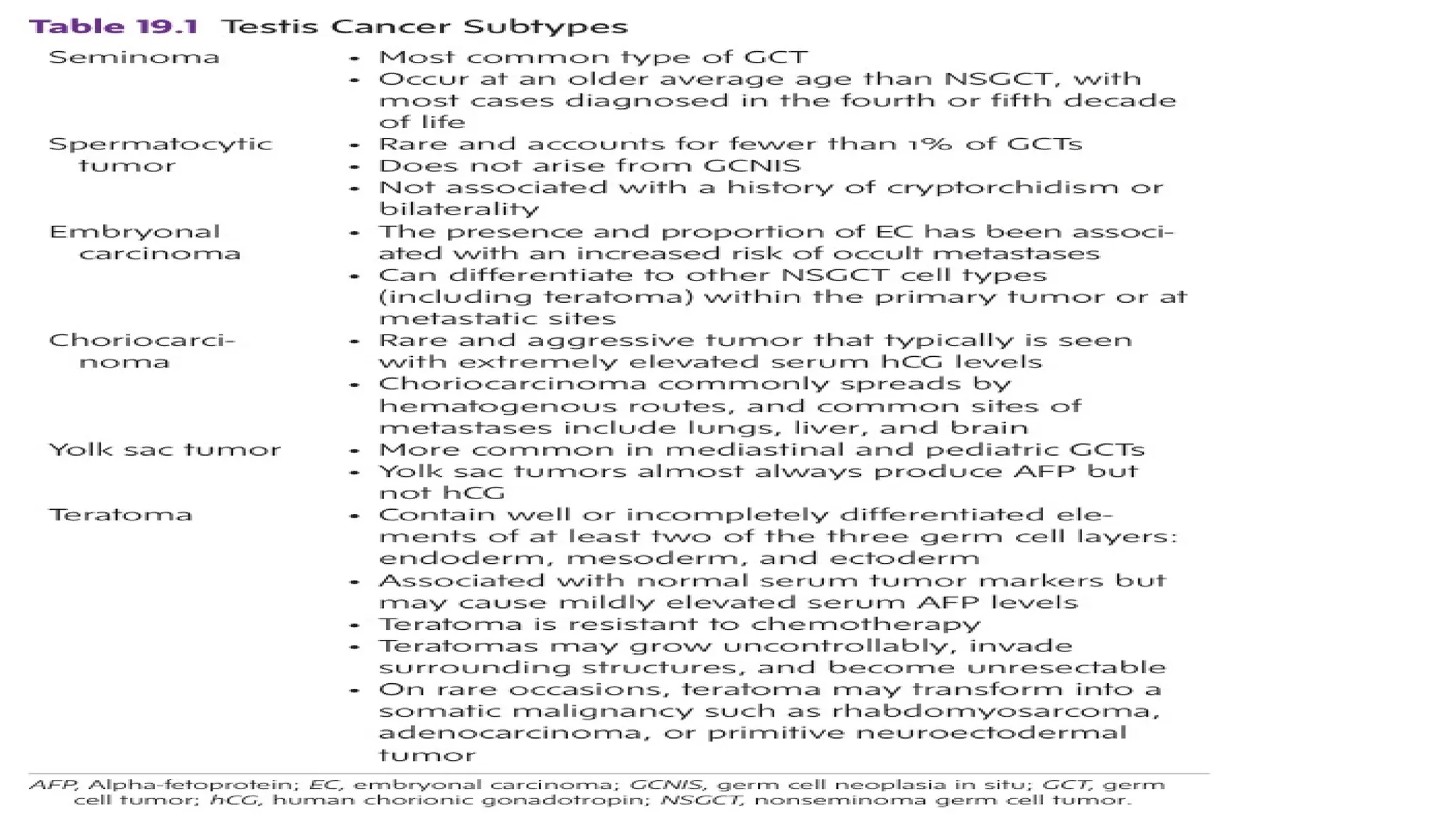
Seminoma
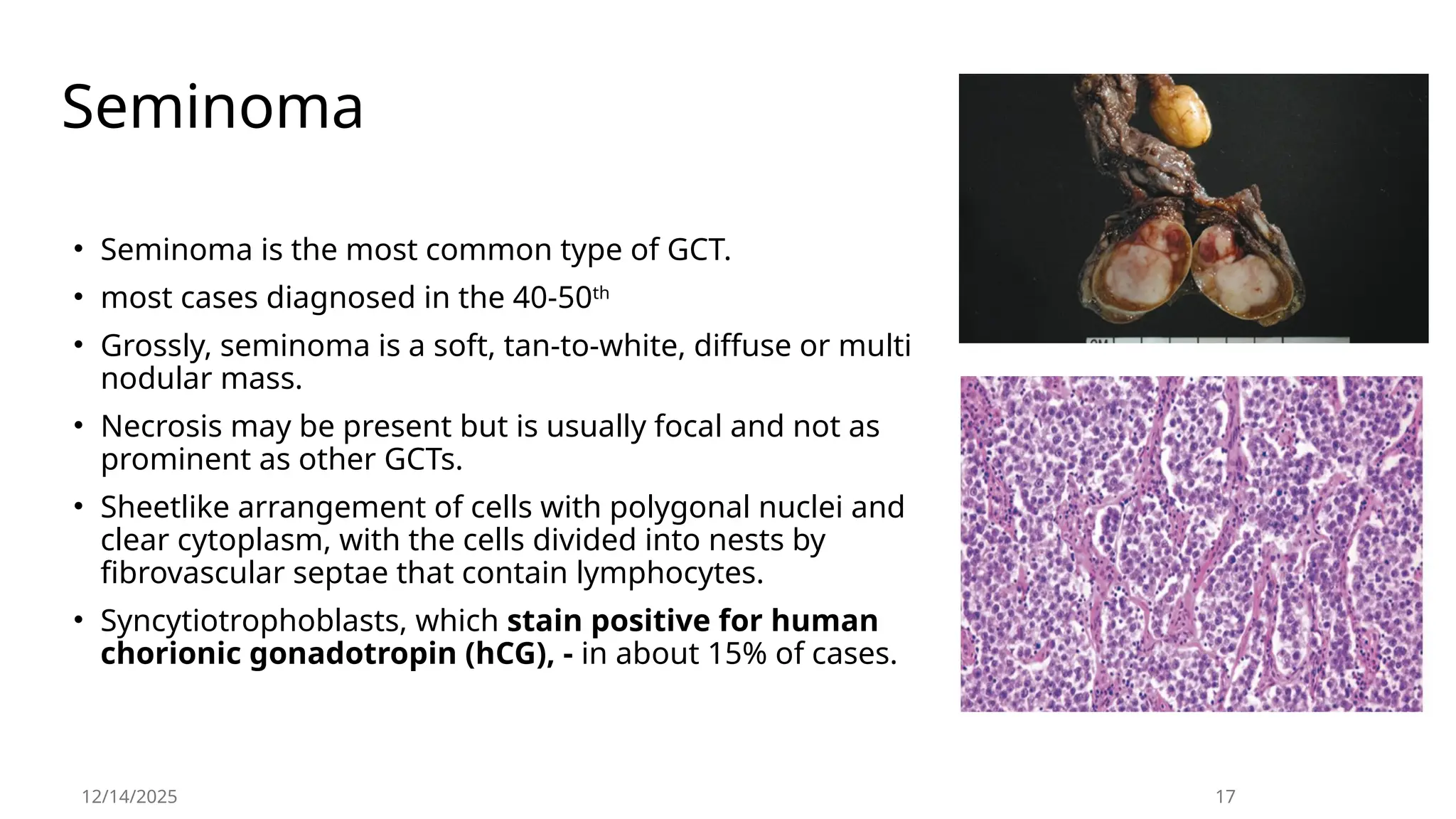
• Seminoma isthe most common type of GCT.
• most cases diagnosed in the 40-50th
• Grossly, seminoma is a soft, tan-to-white, diffuse or multi
nodular mass.
• Necrosis may be present but is usually focal and not as
prominent as other GCTs.
• Sheetlike arrangement of cells with polygonal nuclei and
clear cytoplasm, with the cells divided into nests by
fibrovascular septae that contain lymphocytes.
• Syncytiotrophoblasts, which stain positive for human
chorionic gonadotropin (hCG), - in about 15% of cases.
12/14/2025 17
18.
Seminoma…
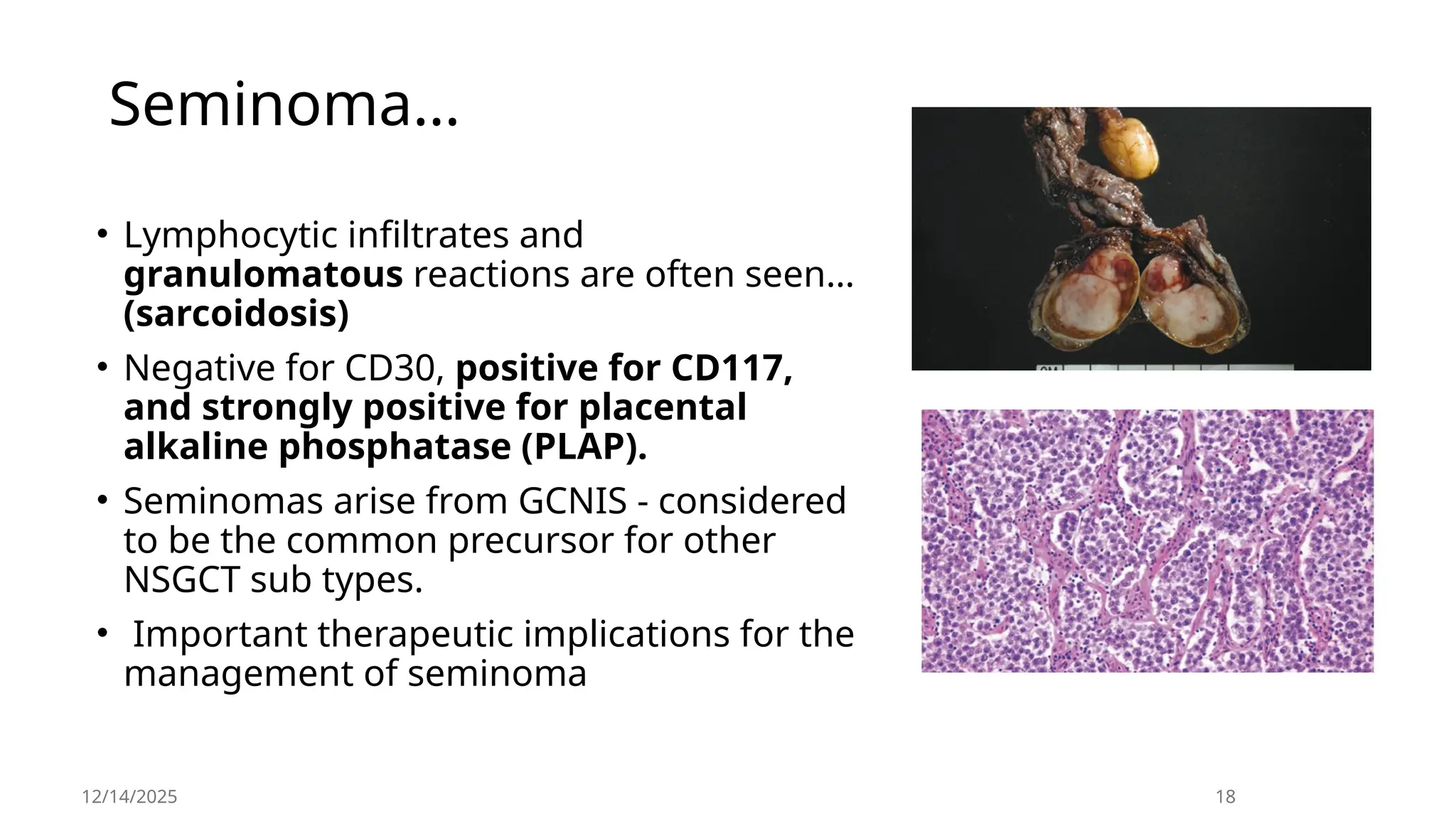
• Lymphocytic infiltratesand
granulomatous reactions are often seen…
(sarcoidosis)
• Negative for CD30, positive for CD117,
and strongly positive for placental
alkaline phosphatase (PLAP).
• Seminomas arise from GCNIS - considered
to be the common precursor for other
NSGCT sub types.
• Important therapeutic implications for the
management of seminoma
12/14/2025 18
19.
12/14/2025 19
Spermatocytic
Tumor
• Spermatocytictumor used to be classified as a
subtype of seminoma.
• Rare and accounts for less than 1% of GCTs.
• Do not arise from GCNIS, not associated with
cryptorchidism or bilaterality, does not
demonstrate i(12p),
• Do not stain for OCT 3/4, PLAP, or glycogen
(periodic acid–Schiff [PAS] stain)
• The peak incidence is the sixth decade of life.
• It is a benign tumor and is almost always cured
with orchiectomy.
• Exceptions - “spermatocytic tumor with sarcoma,”
20.
12/14/2025 20
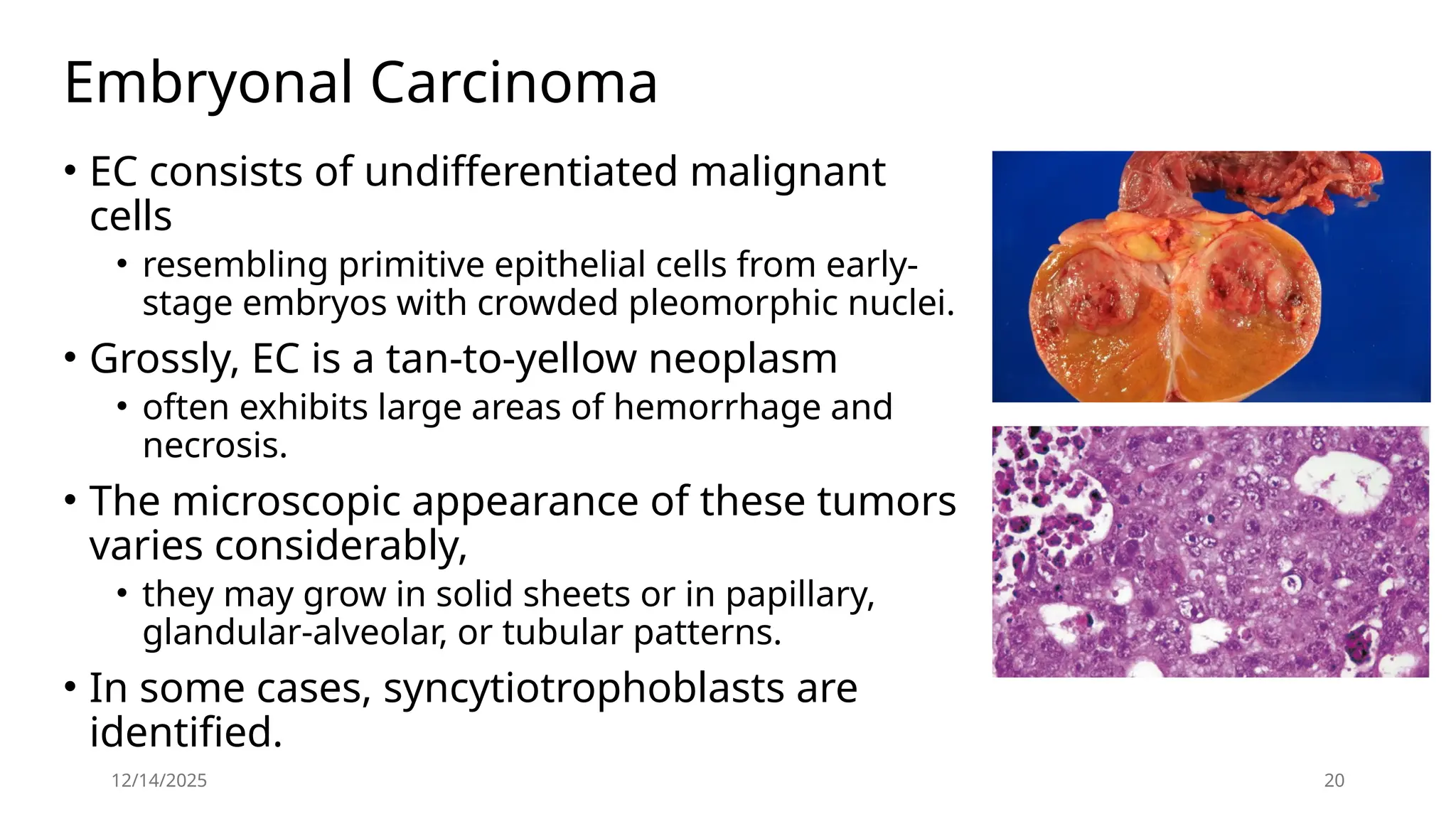
Embryonal Carcinoma
•EC consists of undifferentiated malignant
cells
• resembling primitive epithelial cells from early-
stage embryos with crowded pleomorphic nuclei.
• Grossly, EC is a tan-to-yellow neoplasm
• often exhibits large areas of hemorrhage and
necrosis.
• The microscopic appearance of these tumors
varies considerably,
• they may grow in solid sheets or in papillary,
glandular-alveolar, or tubular patterns.
• In some cases, syncytiotrophoblasts are
identified.
21.
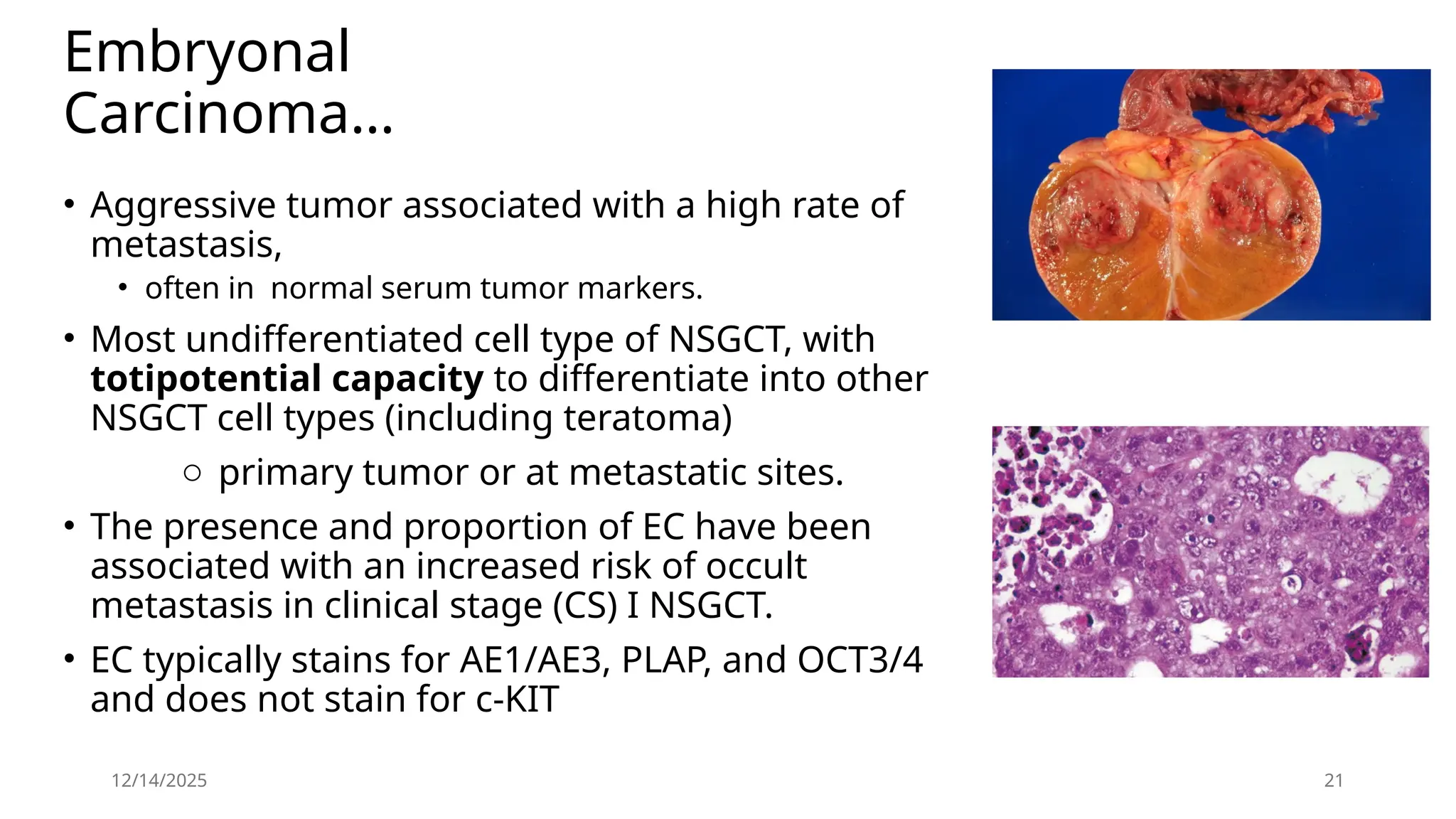
Embryonal
Carcinoma…
• Aggressive tumorassociated with a high rate of
metastasis,
• often in normal serum tumor markers.
• Most undifferentiated cell type of NSGCT, with
totipotential capacity to differentiate into other
NSGCT cell types (including teratoma)
o primary tumor or at metastatic sites.
• The presence and proportion of EC have been
associated with an increased risk of occult
metastasis in clinical stage (CS) I NSGCT.
• EC typically stains for AE1/AE3, PLAP, and OCT3/4
and does not stain for c-KIT
12/14/2025 21
22.
12/14/2025 22
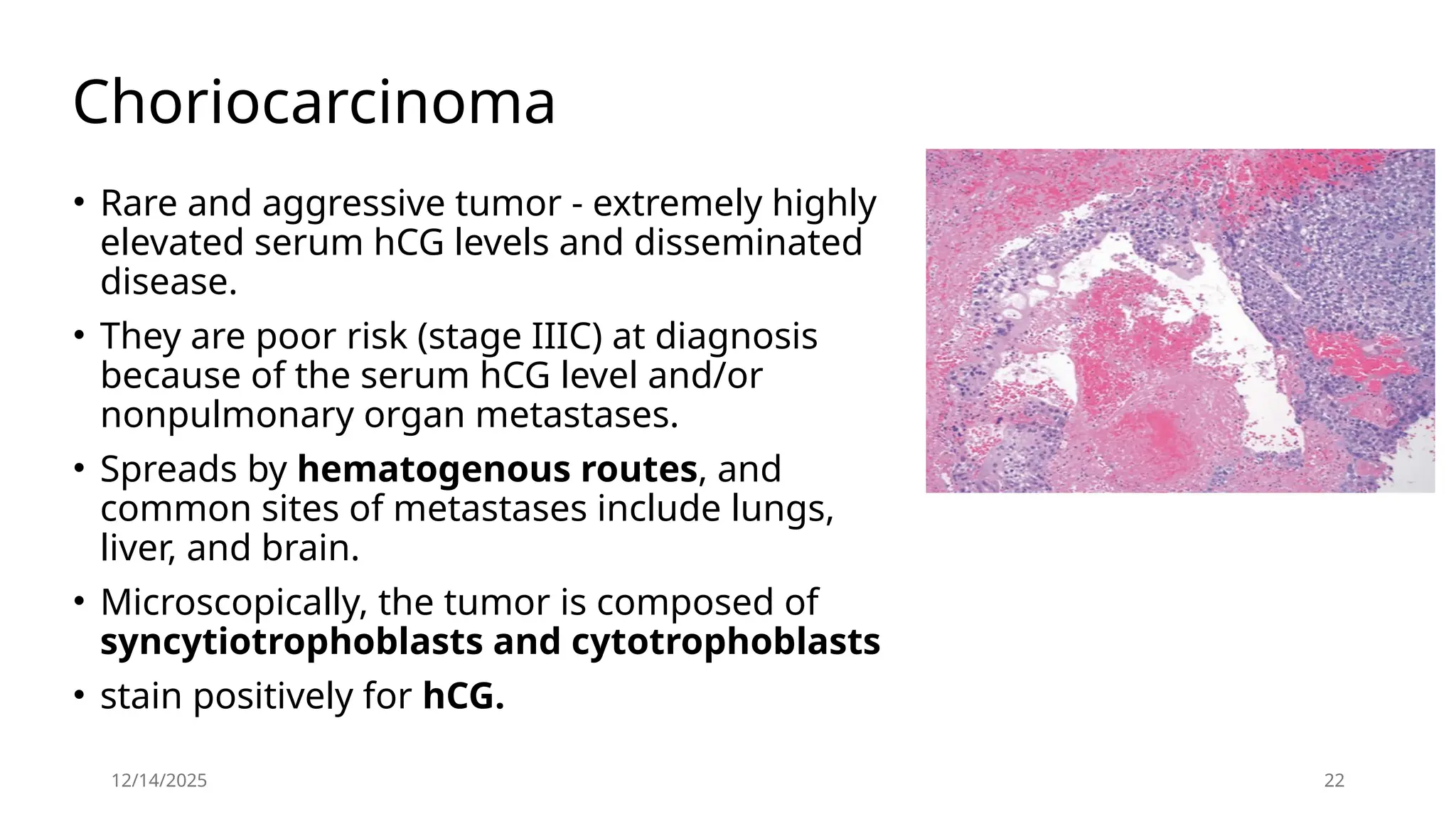
Choriocarcinoma
• Rareand aggressive tumor - extremely highly
elevated serum hCG levels and disseminated
disease.
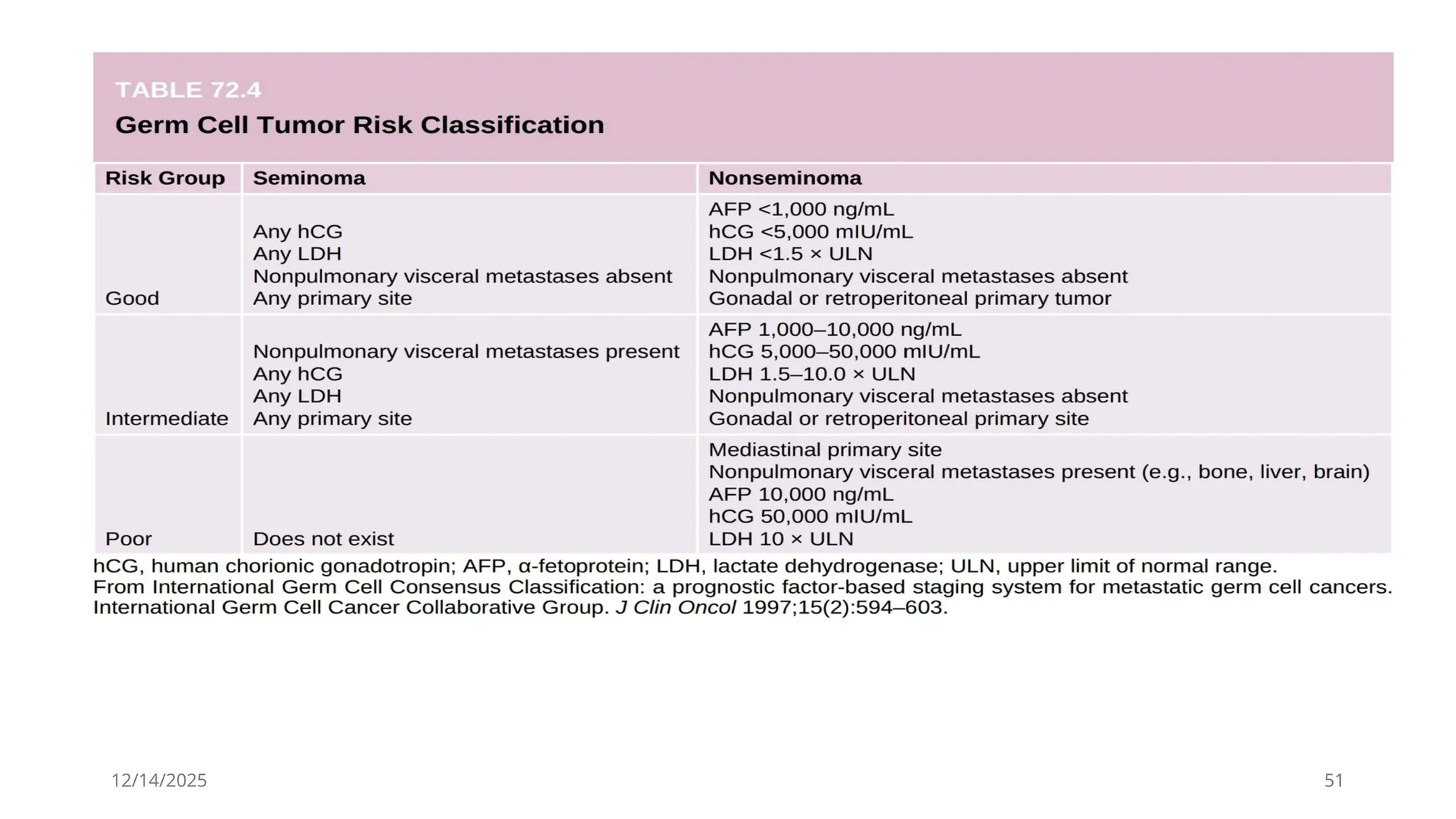
• They are poor risk (stage IIIC) at diagnosis
because of the serum hCG level and/or
nonpulmonary organ metastases.
• Spreads by hematogenous routes, and
common sites of metastases include lungs,
liver, and brain.
• Microscopically, the tumor is composed of
syncytiotrophoblasts and cytotrophoblasts
• stain positively for hCG.
23.
12/14/2025 23
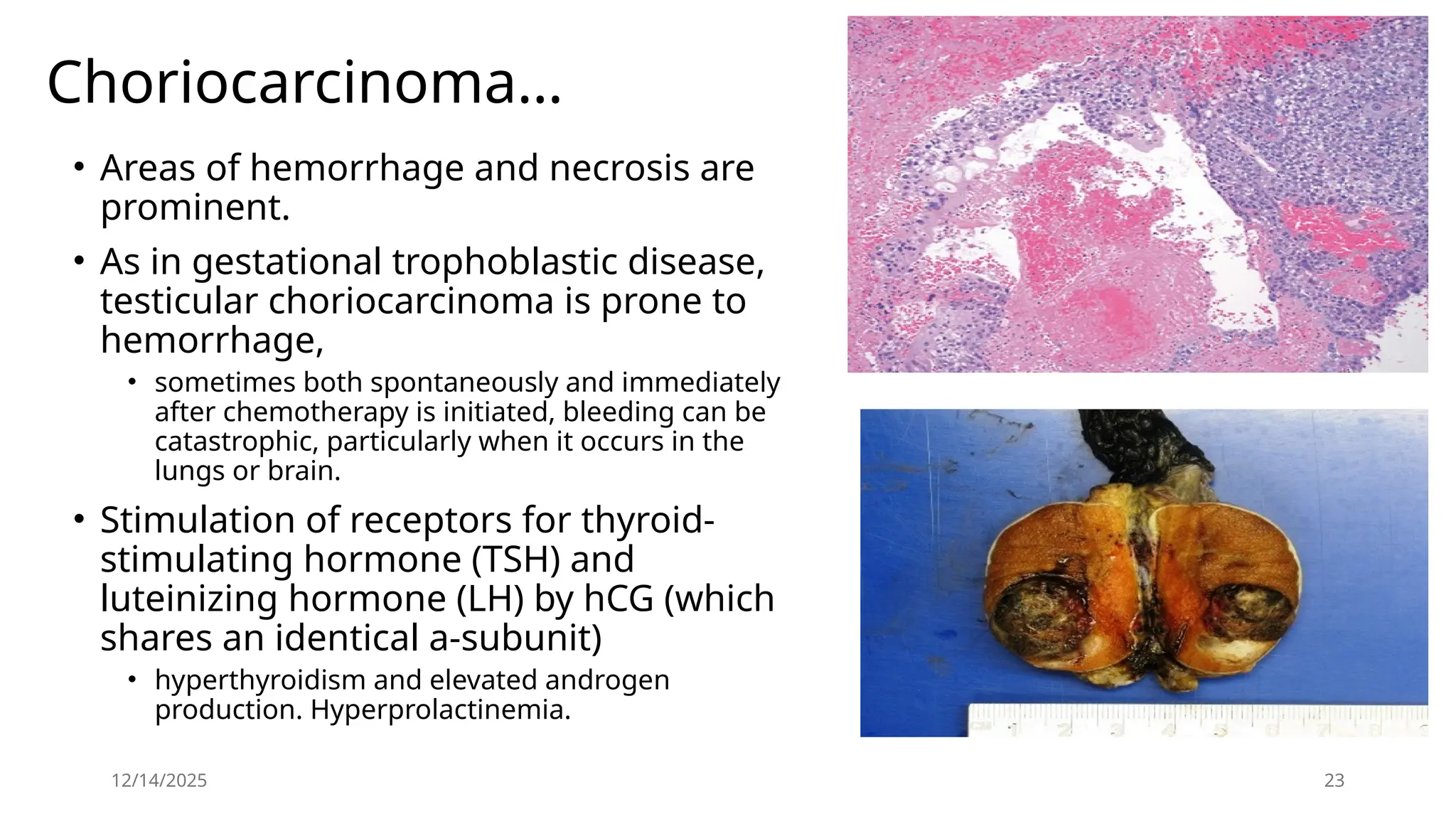
Choriocarcinoma…
• Areasof hemorrhage and necrosis are
prominent.
• As in gestational trophoblastic disease,
testicular choriocarcinoma is prone to
hemorrhage,
• sometimes both spontaneously and immediately
after chemotherapy is initiated, bleeding can be
catastrophic, particularly when it occurs in the
lungs or brain.
• Stimulation of receptors for thyroid-
stimulating hormone (TSH) and
luteinizing hormone (LH) by hCG (which
shares an identical a-subunit)
• hyperthyroidism and elevated androgen
production. Hyperprolactinemia.
24.
12/14/2025 24
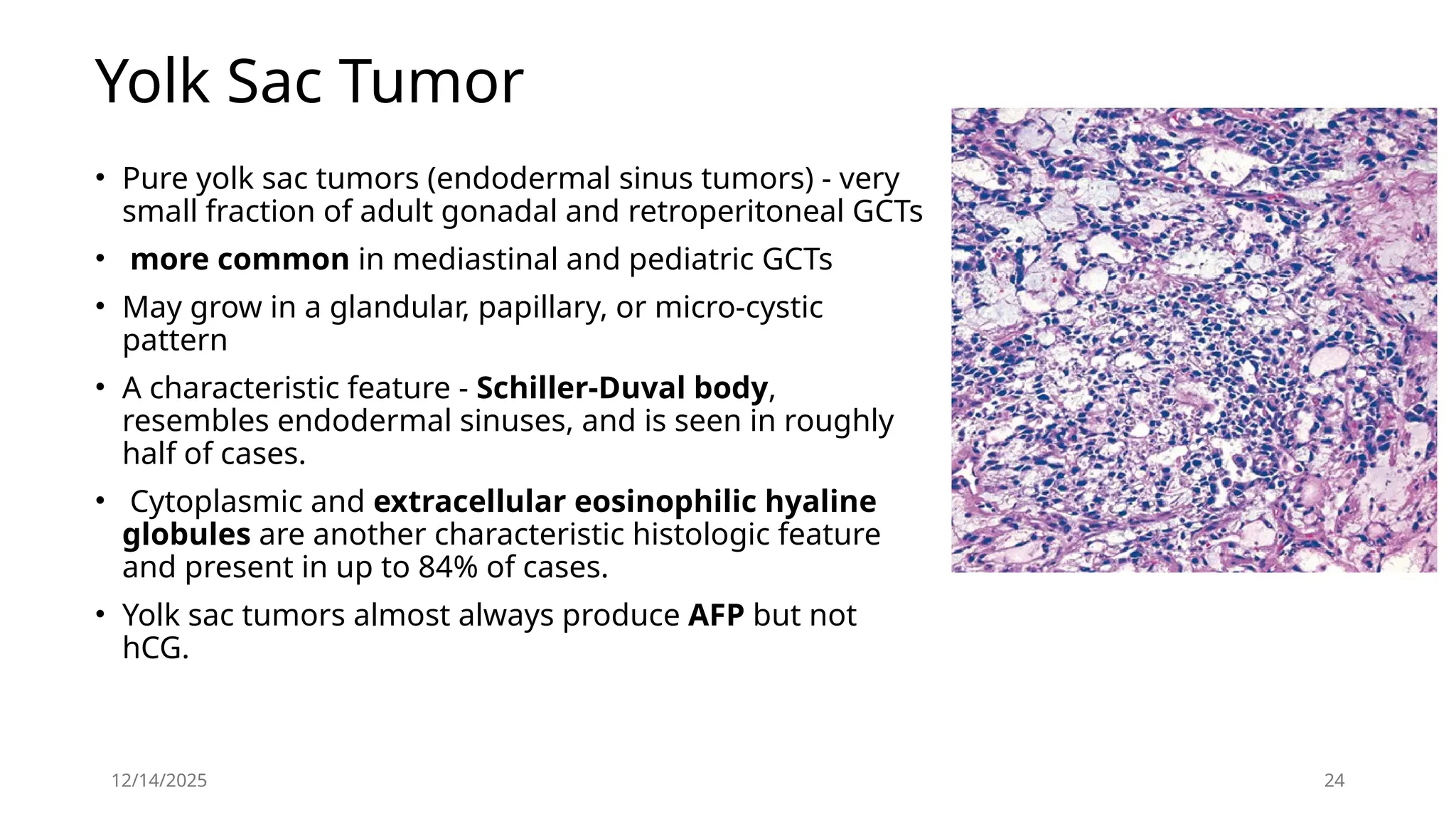
Yolk SacTumor
• Pure yolk sac tumors (endodermal sinus tumors) - very
small fraction of adult gonadal and retroperitoneal GCTs
• more common in mediastinal and pediatric GCTs
• May grow in a glandular, papillary, or micro-cystic
pattern
• A characteristic feature - Schiller-Duval body,
resembles endodermal sinuses, and is seen in roughly
half of cases.
• Cytoplasmic and extracellular eosinophilic hyaline
globules are another characteristic histologic feature
and present in up to 84% of cases.
• Yolk sac tumors almost always produce AFP but not
hCG.
25.
12/14/2025 25
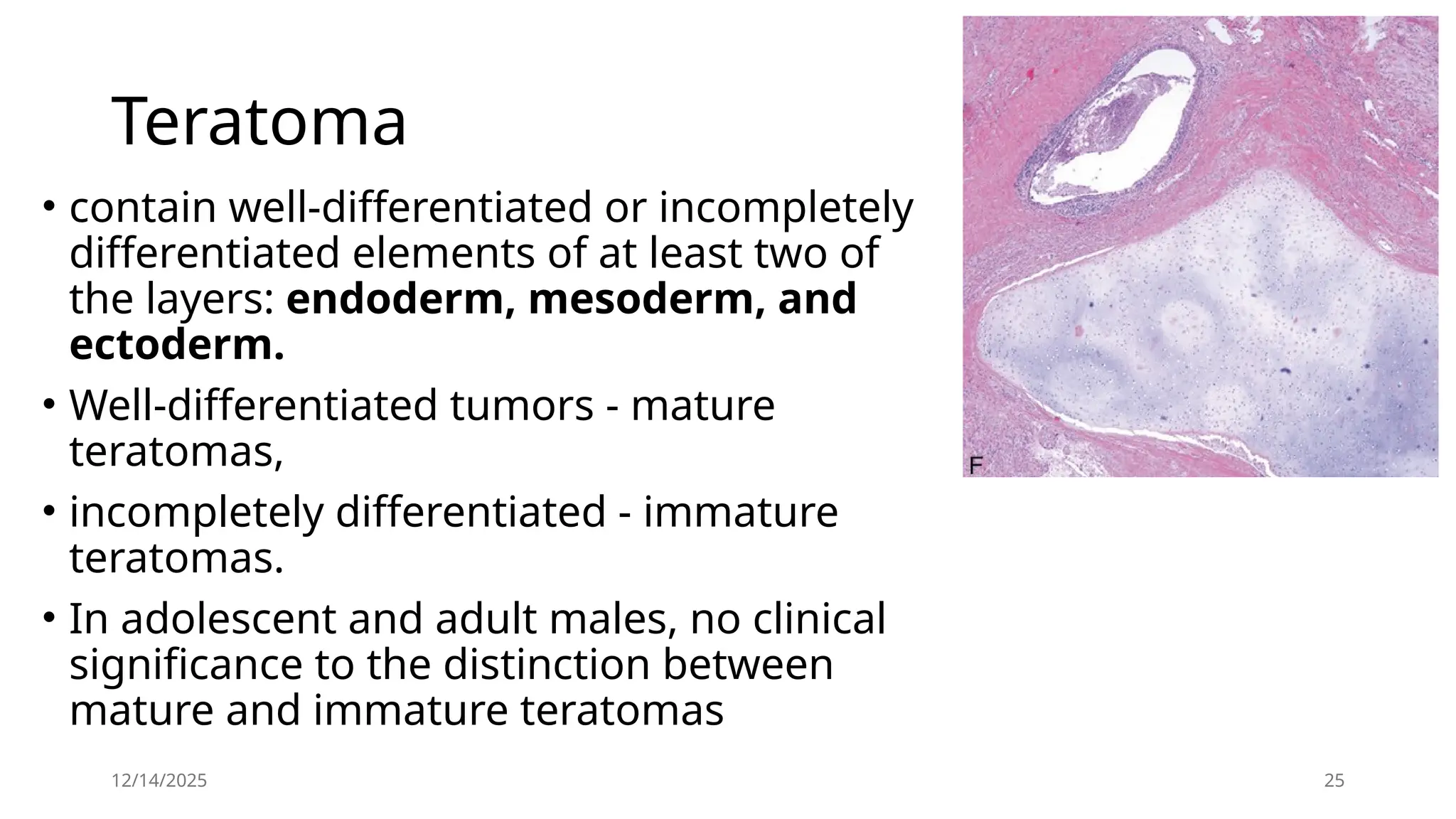
Teratoma
• containwell-differentiated or incompletely
differentiated elements of at least two of
the layers: endoderm, mesoderm, and
ectoderm.
• Well-differentiated tumors - mature
teratomas,
• incompletely differentiated - immature
teratomas.
• In adolescent and adult males, no clinical
significance to the distinction between
mature and immature teratomas
26.
12/14/2025 26
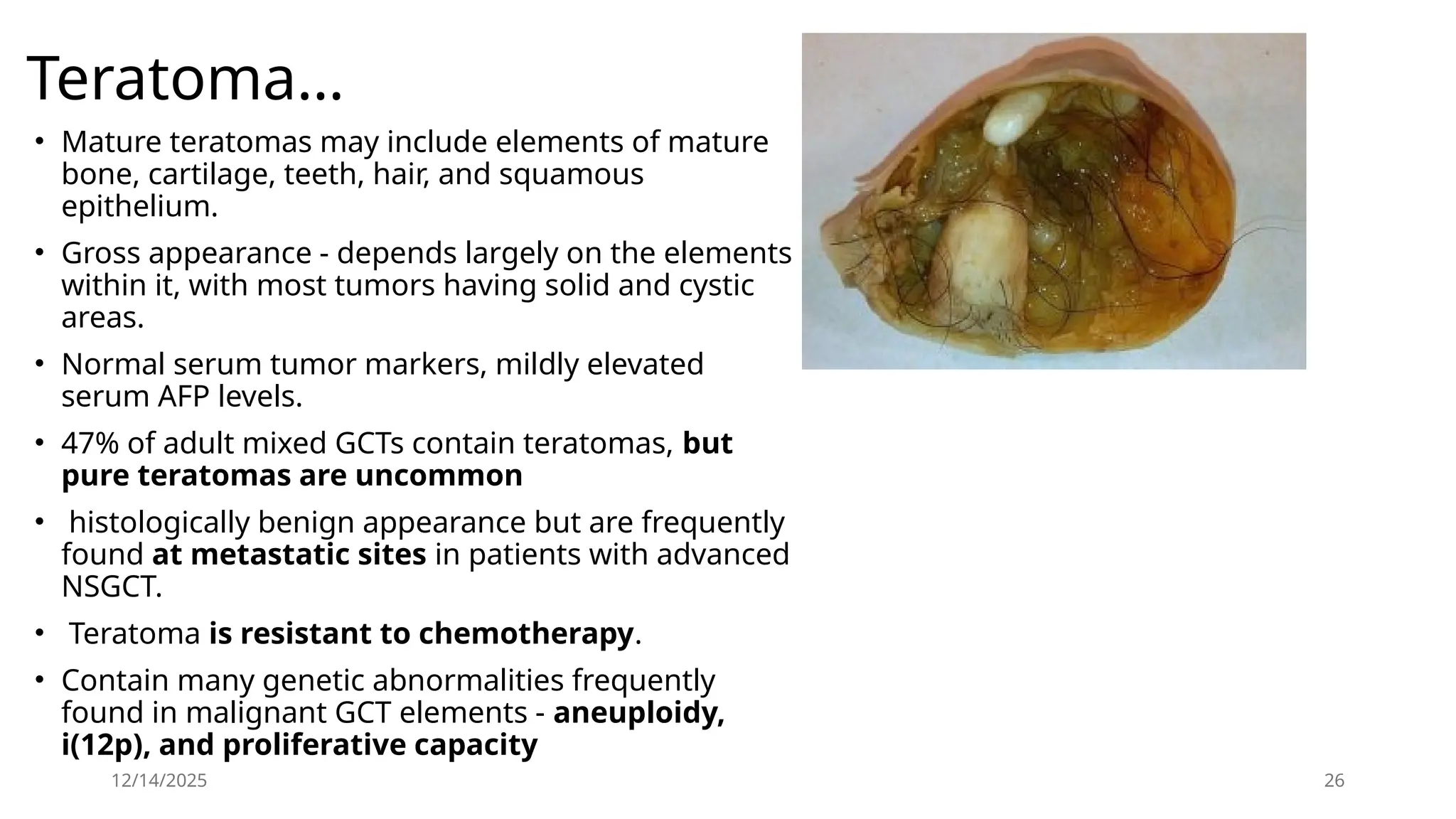
• Matureteratomas may include elements of mature
bone, cartilage, teeth, hair, and squamous
epithelium.
• Gross appearance - depends largely on the elements
within it, with most tumors having solid and cystic
areas.
• Normal serum tumor markers, mildly elevated
serum AFP levels.
• 47% of adult mixed GCTs contain teratomas, but
pure teratomas are uncommon
• histologically benign appearance but are frequently
found at metastatic sites in patients with advanced
NSGCT.
• Teratoma is resistant to chemotherapy.
• Contain many genetic abnormalities frequently
found in malignant GCT elements - aneuploidy,
i(12p), and proliferative capacity
Teratoma…
27.
12/14/2025 27
Teratoma…
• cysticfluid from teratoma contains hCG and AFP - malignant potential.
• genetic instability of teratoma - clinical implications.
• On rare occasions, teratoma may transform into a somatic malignancy such
as rhabdomyosarcoma, adenocarcinoma, or primitive
neuroectodermal tumor.
• These tumors are called teratoma with somatic-type malignancy or
teratoma with malignant transformation.
• Abnormalities of chromosome 12 or i(12p), indicating their origin from GCT.
• Malignant transformation is highly aggressive, resistant to conventional
chemotherapy - poor prognosis
• Only 4% of teratomas with somatic-type malignancy arise within the
testis.
• arise at metastatic sites, within 3 to 4 years after completion of
chemotherapy due to unresected teratoma.
• unresected teratomas in patients with advanced NSGCT may result in late
relapse
Clinical Presentation
Mostcommon - Painless testicular mass
Acute testicular pain less common; due to rapid expansion
from intratumoral hemorrhage or infarction - (NSGCT)
Vague scrotal discomfort / heaviness
History of trauma
Frequently reported
Usually incidental — brings mass to attention
Symptoms from metastasis (10-20%)
Regional/distant metastasis rates at diagnosis NSGCT: ~66%
; Seminoma: ~15%
12/14/2025 29
12/14/2025 31
P/E
• Testicularor extra testicular masses.
• Atrophy of the affected or contralateral testis, particularly in
cryptorchidism.
• A hydrocele may accompany a testis cancer and impair ability to
evaluate the testis.
• In this case, a scrotal ultrasound to evaluate the testis
• Any evidence of palpable abdominal mass or pain,
• Inguinal lymphadenopathy (particularly prior inguinal or scrotal
surgery)
• Gynecomastia
• supraclavicular lymphadenopathy, and auscultation of the chest for
intrathoracic disease
32.
12/14/2025 32
Differential Diagnosis
•Epididymo-orchitis,
• torsion,
• hematoma,
• para-testicular neoplasm (benign or malignant).
• Other diagnostic possibilities include hernia, varicocele, or
spermatocele, though these usually can be distinguished
from a testis mass by physical examination.
• A firm intratesticular mass should be considered cancer
until proven otherwise and should be evaluated further with
a scrotal ultrasound
33.
Diagnostic Delay
• Patientfactor - typically, young and may be less
inclined to seek medical evaluation for symptoms
because of denial, ignorance, or limited access.
• Physician factor – misdiagnosed
• The interval of delay is associated with advanced
clinical stage, sub optimal response to
chemotherapy, and diminished survival.
12/14/2025 33
34.
12/14/2025 34
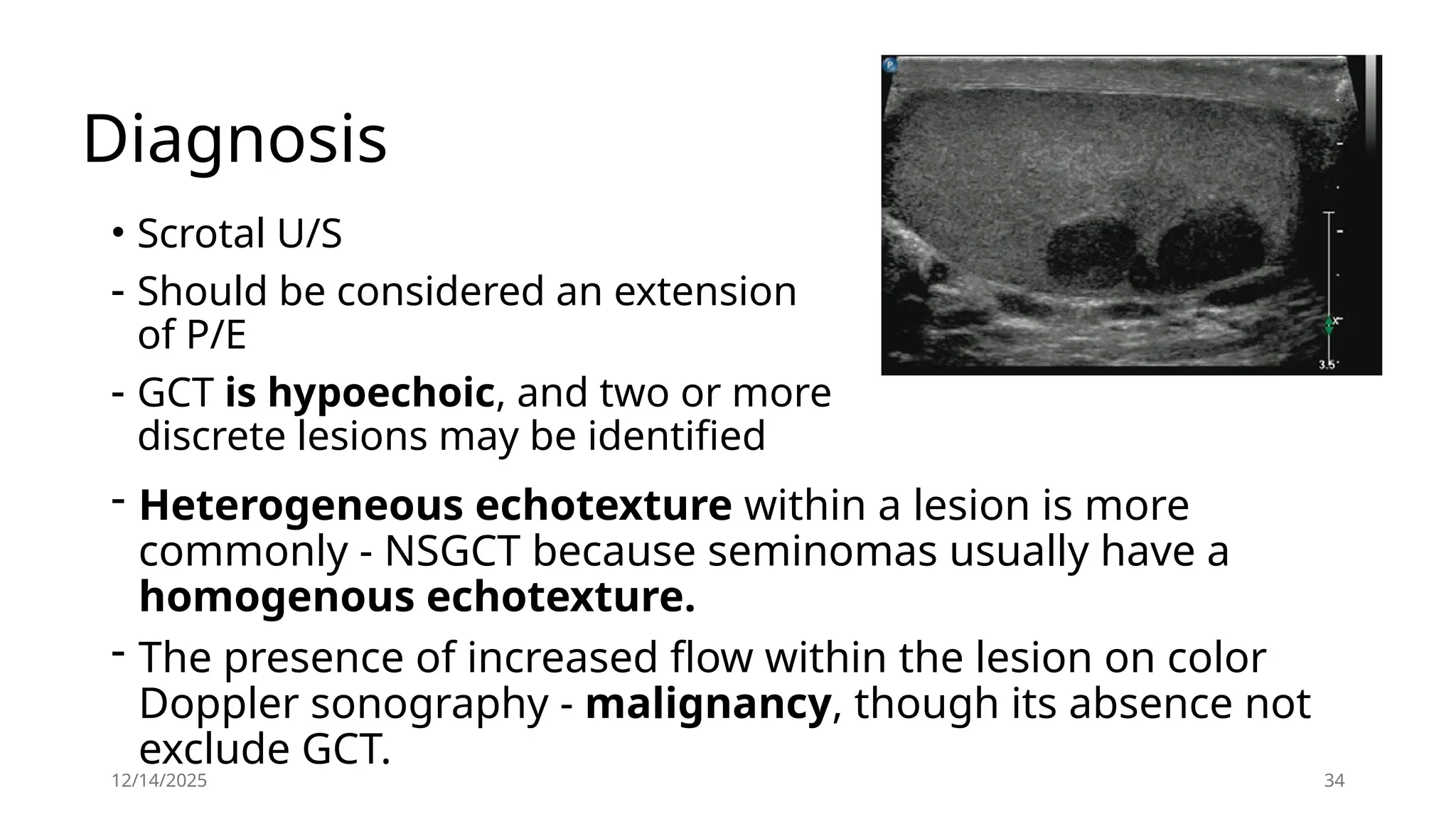
Diagnosis
• ScrotalU/S
- Should be considered an extension
of P/E
- GCT is hypoechoic, and two or more
discrete lesions may be identified
- Heterogeneous echotexture within a lesion is more
commonly - NSGCT because seminomas usually have a
homogenous echotexture.
- The presence of increased flow within the lesion on color
Doppler sonography - malignancy, though its absence not
exclude GCT.
35.
12/14/2025 35
Diagnosis …
MRI
•Sonographic findings are equivocal or
suboptimal
• Testicular Vs extratesticular lesions and
• Neoplastic Vs non-neoplastic entities
36.
12/14/2025 36
Serum tumormarkers
• Few tumors associated with serum tumors
markers.
• (lactate dehydrogenase [LDH], AFP, and hCG) that
are essential in its diagnosis and management.
• at diagnosis before orchiectomy,
• after orchiectomy, to monitor for response to
chemotherapy,
• and to monitor for relapse in patients on
surveillance and after completion of therapy.
37.
12/14/2025 37
AFP
• Thehalf-life is 5 to 7 days.
• At diagnosis, AFP levels are elevated in 50-70% of low-
stage (CS I, IIA, IIB) NSGCT and 60-80% of advanced (CS
IIC, III) NSGCT.
• EC and yolk sac tumors secrete AFP.
• Choriocarcinomas and seminomas do not produce AFP.
• pure seminoma in the primary tumor with an elevated
serum AFP are considered to have NSGCT.
• High AFP in other malignancy
38.
12/14/2025 38
HCG
• Elevatedin 20-40% of low-stage NSGCT and 40-60%
of advanced NSGCT.
• The half-life of hCG is 24 to 36 hours.
• 15% of seminomas secrete hCG.
• hCG is also secreted by choriocarcinoma and EC.
• Levels >5000 IU/L are usually associated with
NSGCT.
39.
HCG …
• Thea-subunit of hCG is common to several pituitary
tumors immunoassays for hCG are directed at the b-
subunit.
• Cross-reactivity of the hCG assay with LH may cause false-
positive hCG elevations in patients with primary
hypogonadism.
• Elevated serum hCG results caused by hypogonadism will
normalize within 48 to 72 hrs after treatment.
• Marijuana use may also cause false-positive hCG results.
12/14/2025 39
40.
12/14/2025 40
LDH
• Elevated20% of low-stage GCT and 20-60% of advanced GCT.
• LDH is expressed in smooth, cardiac, and skeletal muscle.
• Of the five isoenzymes of LDH, LDH-1 is the most frequently
elevated isoenzyme in GCT.
• The magnitude of LDH elevation correlates with the bulk of
disease.
• As a nonspecific marker for GCT, its main use in prognostic
assessment of GCT at diagnosis.
• The serum half life of LDH is 24 hours.
41.
12/14/2025 41
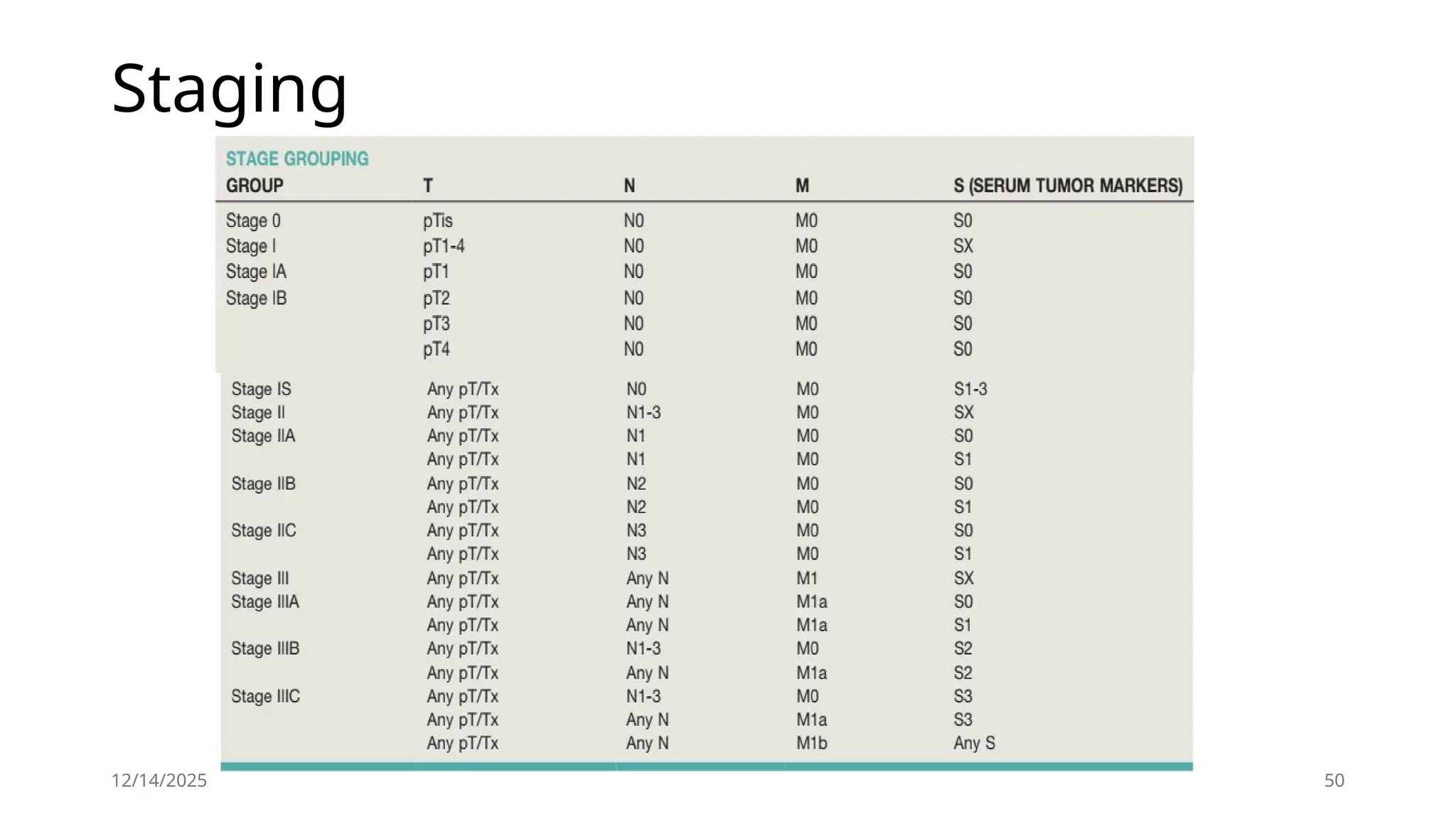
Clinical Staging
•The prognosis of GCT and initial management decisions
are dictated by the clinical stage of the disease
- Histopathological findings
- pathological stage of the primary tumor
- postorchiectomy serum tumor marker levels,
- presence and extent of metastatic disease as
determined by P/E and staging imaging studies,classified
using the Tumor, Node, Metastases (TNM) system
• CS I - clinically confined to the testis
• CS II - regional (retroperitoneal) lymph node metastasis
• CS III - nonregional lymph node and/or visceral metastasis
42.
Staging imaging
• GCTfollows a predictable pattern of metastatic
spread
• The most common route of disease dissemination is
via lymphatic channels
• Primary site --> Retroperitoneum --> Distant site
• Retroperitoneum is the initial site of metastatic
spread in 70% to 80% of GCT
42
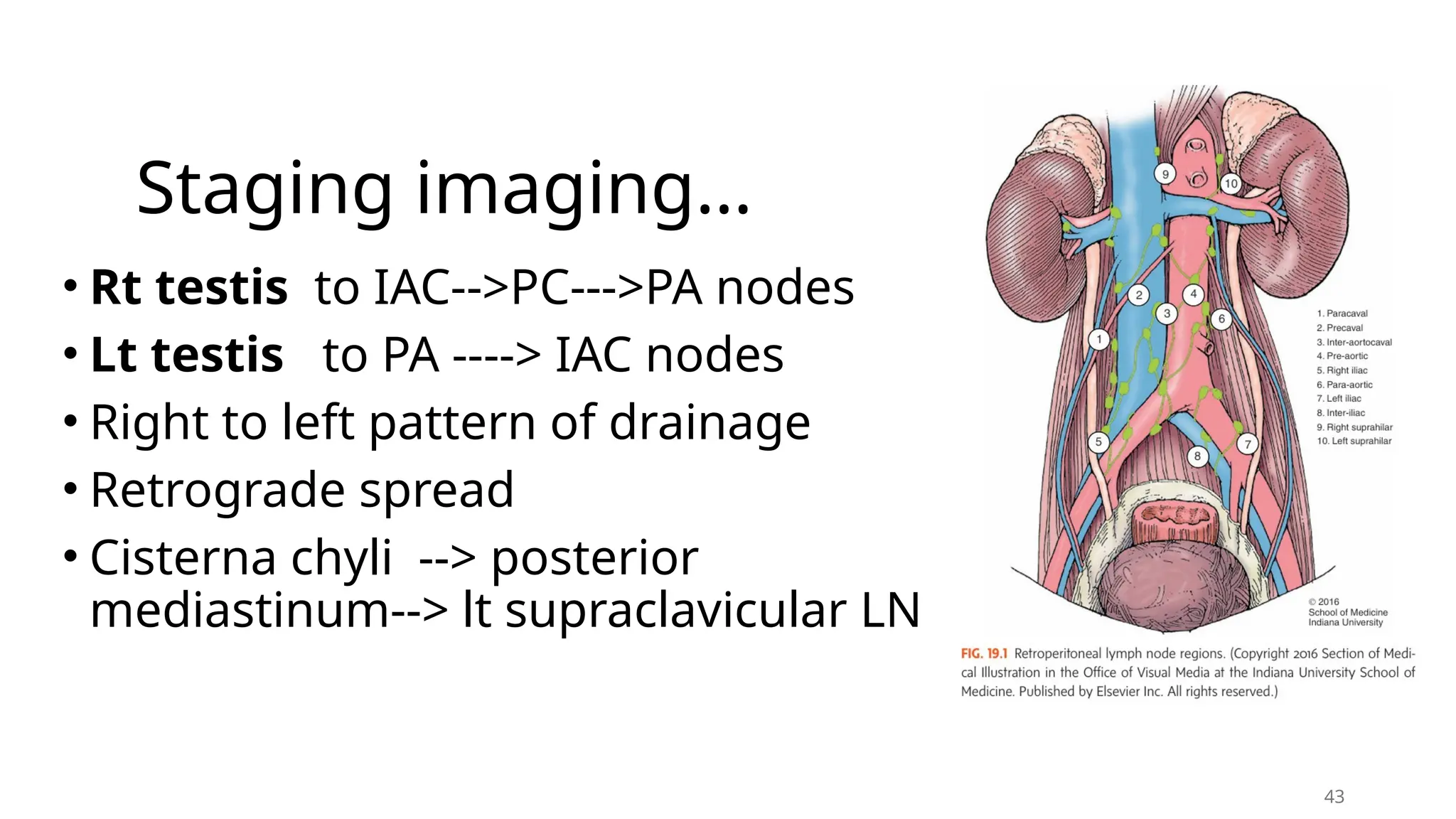
43.
Staging imaging…
• Rttestis to IAC-->PC--->PA nodes
• Lt testis to PA ----> IAC nodes
• Right to left pattern of drainage
• Retrograde spread
• Cisterna chyli --> posterior
mediastinum--> lt supraclavicular LN
43
44.
Staging imaging …
CTAbdomen and Pelvis/MRI
• Most effective, noninvasive means of staging the
retroperitoneum and pelvis
• Most difficult area to accurately stage clinically
• Positive LN in 10% to 20% of seminomas and 60% to
70% of NSGCT
• A size cutoff of 10 mm is frequently used
• False -ve 63%, False +ve 12-40%
• 5-9mm in 1° landing zone
• Sensitivity 91% and specificity of 50%
44
45.
12/14/2025 45
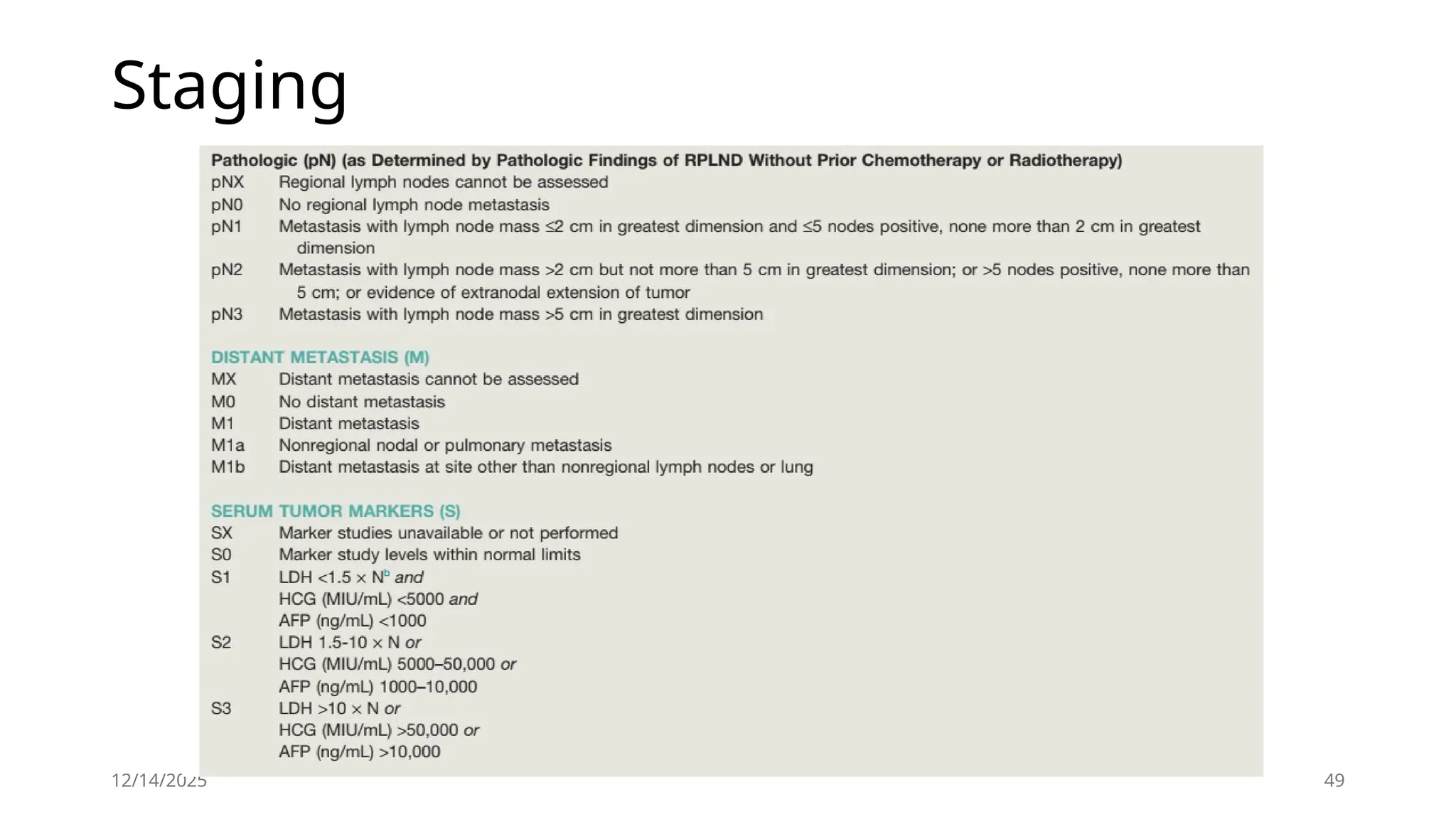
Pathological Stagingof the Abdomen and Pelvis
• Pathological N stage differs from clinical N stage in that the
former considers the number of lymph nodes involved:
• pN0: no regional lymph node metastasis;
• pN1: #5 lymph nodes involved, none >2 cm
• pN2: .5 lymph nodes involved and/or any lymph node 2 to 5
cm;
• pN3: any lymph node >5 cm.
46.
Staging imaging
Chest imaging
•Chest x-ray
Chest CT
• Post-orchiectomy elevated serum tumor markers
• Evidence of metastatic disease
• Abnormal or equivocal findings on chest x-ray
• CS I NSGCT with evidence of LVI or EC predominance
12/14/2025 46
47.
12/14/2025 47
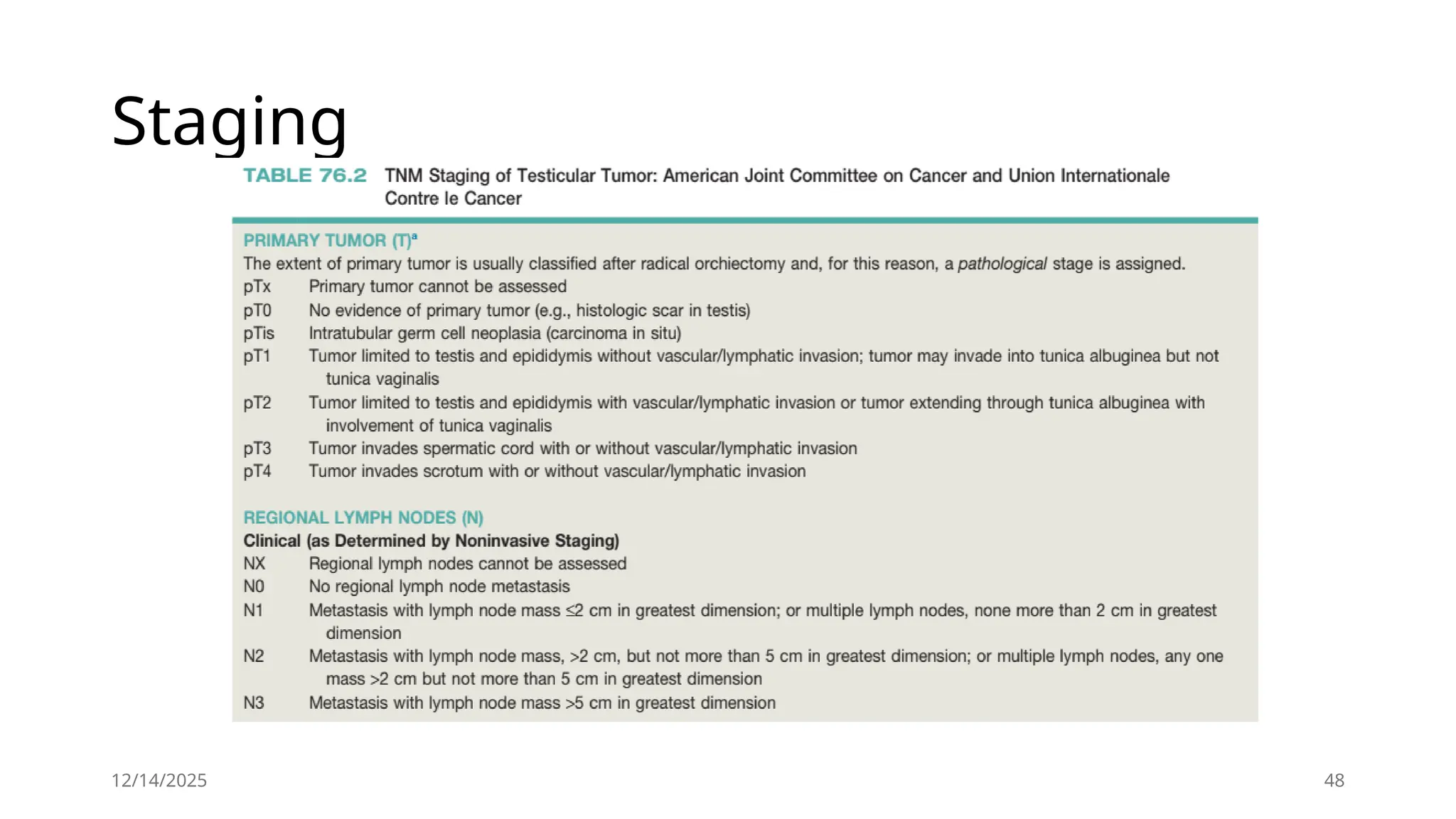
Staging
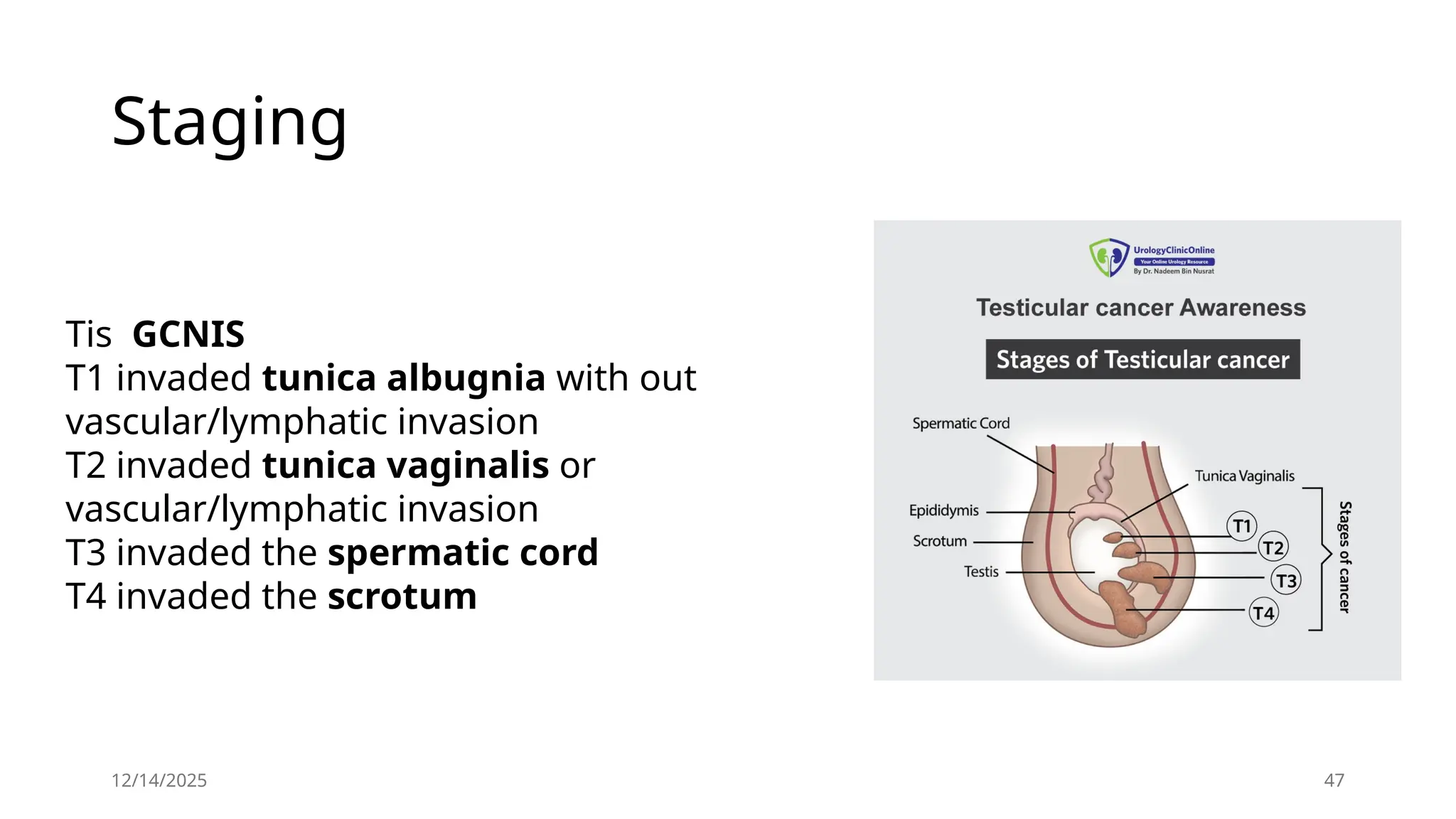
Tis GCNIS
T1invaded tunica albugnia with out
vascular/lymphatic invasion
T2 invaded tunica vaginalis or
vascular/lymphatic invasion
T3 invaded the spermatic cord
T4 invaded the scrotum
52
Summary
• 95% aregerm cell tumors
• GCTs are broadly categorized as seminoma and nonseminoma
• 95% of GCTs arise in the testis, and 5% are extragondal
• Most have good prognosis
• Cryptorchidism, Family history, and Personal history are the strongest risk factors
• Develop from arrested primordial germ cells
• The most common is a painless testicular mass
• Scrotal Ultrasound should be considered as an extension of the physical
examination
• Tumor markers are essential in its diagnosis and management
• GCT follows a predictable pattern of metastatic spread
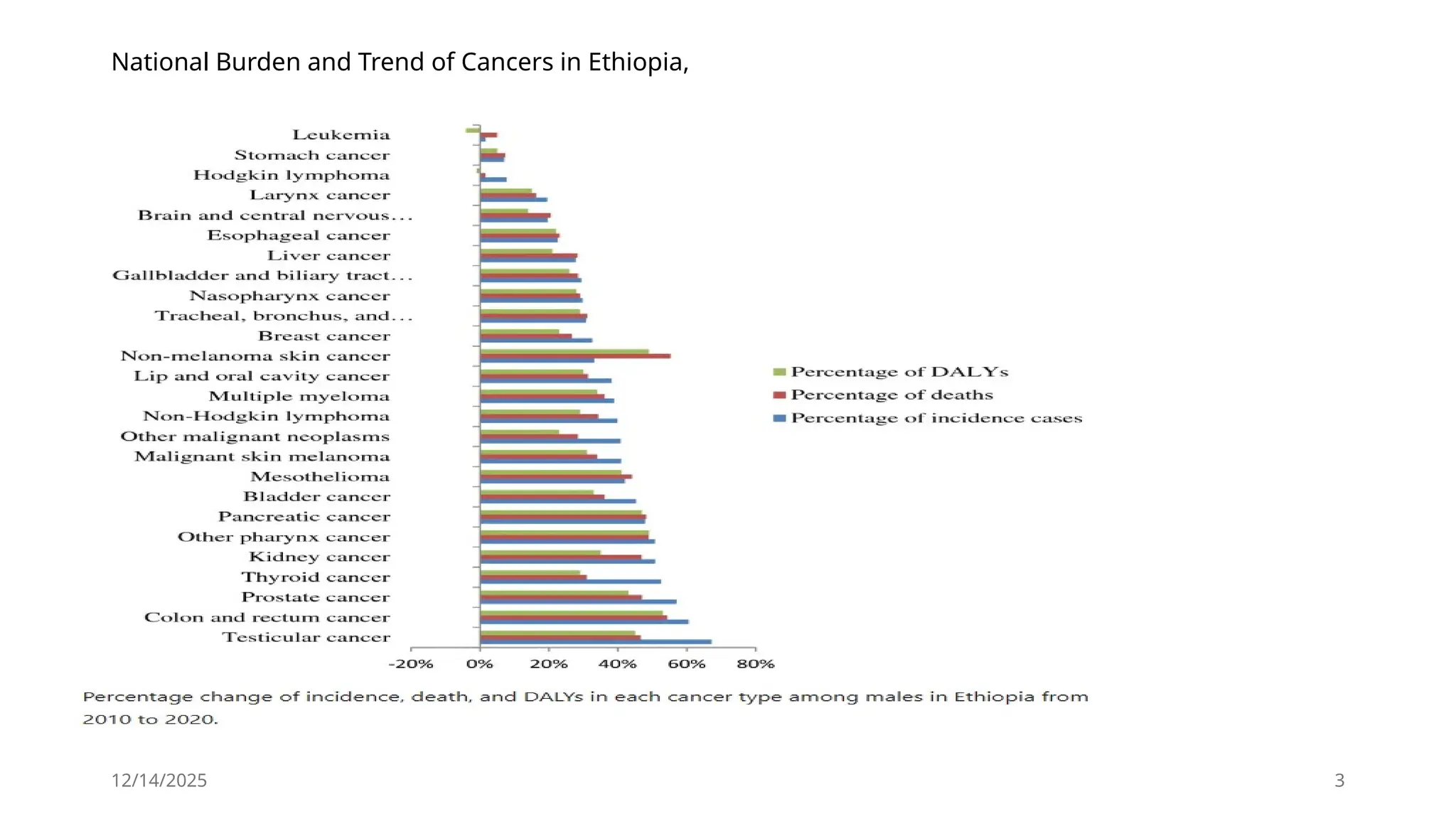
#4 Approximately 95% of GCTs arise in the testis, and 5% are extragonadal in origin. With the development of cisplatin based chemotherapy and the integration of surgery, GCTs have become a model of a curable neoplasm and serve as a paradigm for the multidisciplinary treatment of cancer (Einhorn, 1981). In the pre-cisplatin era, the cure rate for patients with advanced GCT was 5-10%. Currently, the long-term survival for males with metastatic GCT is 80-90%. With the successful cure of patients, an important treatment objective is minimizing treatment-related toxicity without compromising curability. Mortality from GCT is due to inherent resistance to platin chemotherapy and the failure to fully eradicate residual disease elements in the early course of therapy. Non-GCT tumors of the testis are rare and include sex cord– stromal tumors, lymphoid and hematopoietic tumors, tumors of the collecting duct and rete testis, and tumors of the testicular ad nexa.
#6 A stage migration of GCT has been observed in several countries caused, in part, by increased awareness and earlier diagnosis. Between 1973 and 2014, the percentage of tu mors diagnosed at a localized stage increased from 55-68% in the United States. Only about 13% of males present with distant metastatic disease
#7 Infertile and subfertile males also have a higher incidence of testis cancer. Numerous studies have reported that recent increases in testis cancer incidence can be largely attributed to birth-cohort effects, which implies that diet and/or other environmental factors play a major role in GCT carcinogenesis. Specific environmental factors have not been definitively identified, but there is evidence of an association between early exposure to endocrine-disrupting chemicals and an increased risk of testicular GCTs. Males with cryptorchidism are four to six times more likely to be diagnosed with testis cancer in the affected gonad, but the relative risk falls to two to three times if orchidopexy is per formed before puberty. A meta-analysis of cryptorchidism studies reported that the contralateral descended testis is also at slightly increased risk. Males with a first-degree relative with testis cancer have a substantially increased risk of testis cancer, and the median age at diagnosis in these patients is 2 to 3 years younger than in the general population. An individual’s RR for testis cancer is 8 to 12 with an affected brother compared to 2 to 4 in those with an affected father. Males with a history of testis cancer are at a twelvefold increased risk of developing GCT in the contralateral testis, but the 15-year cumulative incidence is only 2%. Most GCTs arise from a precursor lesion called GCNIS. Exceptions to this are prepubertal GCTs (which can rarely occur after puberty), ovarian cystic teratomas, dermoid cysts, and spermatocytic tumors (previously referred to as spermatocytic seminomas). GCNIS is present in adjacent testicular parenchyma in 80 90% of cases of invasive GCT and is associated with a 50% risk of GCT within 5 years and 70% within 7 years Between 5% and 9% of patients with GCT have GCNIS within the unaffected contralateral testis, though the incidence of contralateral GCNIS increases to about 36% in males with testicular atrophy or cryptorchidis. Gene expression profile analysis indicates that GCNIS develops before birth from an arrested gonocyte (Hussain et al., 2008; Sonne et al., 2009). In males with a history of GCT, the finding of testicular microlithiasis on ultrasound of the contralateral 1658 Chapter 79 Neop
#8 . For clinical purposes, GCNIS- derived GCTs are divided into seminoma and NSGCT, and the relative distribution of each is 52-56% and 44-48%, respectively (McGlynn et al., 2005; Powles et al., 2005). NSGCTs include embryo nal carcinoma (EC), yolk sac tumor, teratoma, and choriocarcinoma subtypes, either alone as pure forms or in combination as mixed GCT with or without seminoma. Most NSGCTs are mixed tumors that are composed of two or more GCT subtypes. GCTs that contain both NSGCT subtypes and seminoma are classified as NSGCT even if the NSGCT component represents a tiny proportion of the tumor
#11 Intratubular germ cell neoplasia is thought to derive from malig nant transformation of primordial germ cells or gonocytes during fetal development.10 Primordial germ cells migrate from the prox imal epiblast (yolk sac) through the hindgut and mesentery to the genital ridge and become gonocytes. The precise molecular events underlying transformation to ITGCN are not well understood. The most consistent genetic finding in germ cell tumors is a gain of material from chromosome 12p. The majority of NSGCT and seminomas contain i(12p), an isochromosome composed of two fused short arms of chromosome 12. The remaining i(12p)-neg ative germ cell tumors also have a gain of 12p sequences in the form of tandem duplications, which may be transposed elsewhere in the genome. Gain of 12p sequences has been found in ITGCN, indicating that it is an early event in testicular cancer pathogenesis. The acqui sition of i(12p) is not thought to be the initiating event, however, because it is preceded by polyploidization.26 Overexpressed genes on 12p are likely to be important, and there are candidate genes on 12p, including several that confer growth advantage (KRAS2, CCND2 [cyclin D2]) and others that establish or maintain the stem cell phenotype (NANOG, DPPA3, GDF3). The exact genes that are critical to this step have not yet been identified. Seminomas are usually hypertriploid, whereas NSGCT is more commonly hypotriploid.27 Other chromosome regions were found to have nonrandom gains or losses in germ cell tumors with less frequency than 12p. Single-gene mutations are uncommon in germ cell tumors. The KIT/kit ligand (KITLG) pathway has special rele vance for gonadal development. The biologic function of this path way is broad and includes development of hematopoietic cells, mela nocytes, and germ cells.28 KITLG is essential for primordial germ cell survival and motility, as are the chemokine SDF-1 (CXCL12) and its receptor CXCR4.11 Immunohistochemical markers found on primordial germ cells and gonocytes (PLAP, CD117 [KIT], OCT3/4 [POU5F1]) are also found on ITGCN, suggesting a transformation from these cells during fetal development (see Fig. 47.3). The bial lelic expression of imprinted genes in germ cell tumors has been reported, showing that they likely arose from primordial germ cells, where the genomic imprinting is temporarily erased.29 The Integrated Molecular Characterization of Testicular Germ Cell Tumors effort published in 2018 analyzed 137 primary testic ular germ cell tumors and found a relate paucity of somatic muta tions with only KIT (18%), KRAS (14%), and NRAS (4%) having a significant presence will all being present in seminoma.30 The somatic alterations in KIT found in germ cell tumors are predicted to upregulate pathway activity. KITLG plays a role in determining skin pigmentation and has undergone strong selection in Euro pean and Asian populations. Difference in the frequency of risk alleles for KITLG between European and African populations may provide an explanation for the difference in germ cell tumor inci dence between white Americans and African Americans. There is evidence that epigenetic regulation of gene expression plays a role in the pathogenesis of germ cell tumors. The DNA methylation patterns are different among histologic types. Global hypomethylation is more common in seminomas than in NSGCT.29 In a study of 16 germ cell tumors, the methylation of CpG islands in NSGCT was similar to that observed in other tumor types, whereas it was virtually absent in seminomas.31 Aberrant promoter methylation is generally associated with absent or downregulated expression of the methylated genes. This can result, for example, in the silencing of tumor suppressor genes.29 Methylation has also been correlated with germ cell tumor differentiation. The more differentiated tumors (yolk sac tumor, choriocarcinoma, and teratoma) were consistently hypermethylated, whereas seminoma and GCNIS were hypomethyl ated.32 Some of the observed methylation patterns may reflect normal development rather than germ cell tumor pathogenesis
#13 gonocytes that failed to differentiate into prespermatogonia,
#16 Spalt-like transcription factor 4 is expressed in almost all germ cell tumors and has been reported to be positive in GCNIS, classic seminoma, spermatocytic tumor, embryonal carcinoma, yolk sac tumor, choriocarcinoma, and teratoma.39,40 Octamer-binding transcription factor 3/4 is variably expressed in GCNIS, classic seminoma, embryonal carcinoma, and yolk sac tumor. Spermato cytic tumor, choriocarcinoma, and teratoma are usually negative for OCT3/4. Cluster of differentiation 117 (KIT) helps highlight GCNIS and classic seminoma. CD30, SRY-box transcription fac tor 2, and keratin are helpful in the diagnosis of embryonal car cinoma, and SALL4 and glypican-3 are often positive in yolk sac tumor.35 In tumors of unknown primary or those presenting as a retroperitoneal or mediastinal mass, SALL4, OCT3/4, CD117, SOX2, CD30, and low-molecular-weight keratins all may be use ful in distinguishing germ cell tumors from non–germ cell tumor
#17 Syncytiotropho blasts, which stain positive for human chorionic gonadotropin (hCG), can be identified in about 15% of cases but are of no clear prognostic significance (Cheville, 1999). Lymphocytic infiltrates and granulomatous reactions are often seen, and seminomas ap pear to be associated with an increased incidence of sarcoidosis (Rayson et al., 1998; Tjan-Heijnen et al., 1998). Seminomas may be confused with solid-pattern EC, yolk sac tumor, or Sertoli cell tu mors (Ulbright and Young, 2008). Although immunohistochemical staining plays a limited role in diagnosing GCTs, seminomas are typically negative for CD30, positive for CD117, and strongly positive for placental alkaline phosphatase (PLAP). Anaplastic seminoma was a previously recognized subtype of seminoma, but this distinction is of no clear biologic or clinical significance and is no longer recognized. Seminomas arise from GCNIS and are considered to be the common precursor for the other NSGCT sub types (Ulbright, 2004). This ability of seminomas to transform into NSGCT elements has important therapeutic implications for the management of seminoma (discussed later) (Ulbright, 2004)
#18 Syncytiotropho blasts, which stain positive for human chorionic gonadotropin (hCG), can be identified in about 15% of cases but are of no clear prognostic significance (Cheville, 1999). Lymphocytic infiltrates and granulomatous reactions are often seen, and seminomas ap pear to be associated with an increased incidence of sarcoidosis (Rayson et al., 1998; Tjan-Heijnen et al., 1998). Seminomas may be confused with solid-pattern EC, yolk sac tumor, or Sertoli cell tu mors (Ulbright and Young, 2008). Although immunohistochemical staining plays a limited role in diagnosing GCTs, seminomas are typically negative for CD30, positive for CD117, and strongly positive for placental alkaline phosphatase (PLAP). Anaplastic seminoma was a previously recognized subtype of seminoma, but this distinction is of no clear biologic or clinical significance and is no longer recognized. Seminomas arise from GCNIS and are considered to be the common precursor for the other NSGCT sub types (Ulbright, 2004). This ability of seminomas to transform into NSGCT elements has important therapeutic implications for the management of seminoma (discussed later) (Ulbright, 2004)
#19 Spermatocytic tumor (previously referred to as spermatocytic seminoma) used to be classified as a subtype of seminoma but is now considered a distinct entity from seminoma and other GCTs. It is rare and accounts for less than 1% of GCTs. Unlike other GCTs, spermatocytic tumor does not arise from GCNIS, is not associated with a history of cryptorchidism or bilaterality, does not demon strate i(12p), and does not occur as part of mixed GCTs (Ulbright, 2005). The lack of association of spermatocytic tumors with GSNIS is similar to juvenile yolk sac tumor and teratoma. Histopathologically, they differ from seminoma in that they do not stain for OCT 3/4, PLAP, or glycogen (periodic acid–Schiff [PAS] stain); nuclei are round; minimal lymphocytic infiltration is present; and three dis tinct cell types are present, including small lymphocyte-like cells, medium-size cells with dense eosinophilic cytoplasm and a round nucleus, and large mononucleated or multinucleated cells (Aggarwal and Parwani, 2009). The peak incidence is the sixth decade of life (Chung et al., 2004; Eble, 1994). It is a benign tumor (only three documented cases of metastases) and is almost always cured with orchiectomy (Chung et al., 2004; Horn et al., 2011). Exceptions to this rule are the rare cases of “spermatocytic tumor with sarcoma,” which exhibits elements of sarcomatous differentiation, and an anaplastic variant, both of which are associated with widely metastatic chemotherapy-resistant disease and poor prognosis
#23 . In addition, choriocarcinomas are associated with hormonal disturbances, most likely caused by highly elevated serum hCG. Stimulation of receptors for thyroid-stimulating hormone (TSH) and luteinizing hormone (LH) by hCG (which shares an identical a-subunit) can result in hyperthyroidism and elevated androgen pro duction (Ulbright, 2005). Hyperprolactinemia has also been reported.
#24 Mixed GCTs often include elements of yolk sac tumor, which consists of a reticular network of medium-sized cuboidal cells with cytoplasmic and extra-cytoplasmic, eosinophilic, hyaline-like globules (Epstein, 2010). Yolk sac tumors may grow in a glandular, papillary, or micro-cystic pattern. A character istic feature is the Schiller-Duval body, which resembles endodermal sinuses, and is seen in roughly half of cases (Fig. 79.1E). Cytoplasmic and extracellular eosinophilic hyaline globules are another characteris tic histologic feature and are present in up to 84% of cases. Yolk sac tumors almost always produce AFP but not hCG
#26 Mature teratomas may in clude elements of mature bone, cartilage, teeth, hair, and squamous epithelium, a fact that most likely explains the name teratoma, which roughly means “monster tumor” in Greek (Fig. 79.1F). The gross appearance of a teratoma depends largely on the elements within it, with most tumors having solid and cystic areas. Teratomas are generally associated with normal serum tumor markers, but they may cause mildly elevated serum AFP levels. Approximately 47% of adult mixed GCTs contain teratomas, but pure teratomas are uncommon (Geldart et al., 2002; Leibovitch et al., 1995). In males, teratomas have a histologically benign appearance but are frequently found at metastatic sites in patients with advanced NSGCT. Teratoma is resistant to chemotherapy. Thus, given its frequent presence at metastatic sites in advanced NSGCT, patients with residual masses after chemotherapy require consolidative surgi cal resection. The inherent chemo-resistance of teratoma is a limita tion to treatment strategies for NSGCT that use chemotherapy alone. Despite their benign histologic appearance, teratomas contain many genetic abnormalities frequently found in malignant GCT elements, including aneuploidy, i(12p), and widely variable prolif erative capacity (Castedo et al., 1989; Sella et al., 1991). Studies have also shown that cystic fluid from teratoma frequently contains hCG and AFP, confirming its malignant potential (Beck et al., 2004; Sella et al., 1991). The genetic instability of teratoma has important clinical implications. Teratomas may grow uncontrollably, invade surrounding structures, and become unresectable (Logothetis et al., 1982). On rare occasions, teratoma may transform into a somatic malignancy such as rhabdomyosarcoma, adenocarcinoma, or primitive neuroectodermal tumor (Comiter et al., 1998; Little et al., 1994; Motzer et al., 1998). These tumors are called teratoma with somatic-type malignancy or teratoma with malignant transformation. These tumors frequently have abnormalities of chromosome 12 or i(12p), indicating their origin from GCT. Malignant transformation is highly aggressive, resistant to conventional chemotherapy, and associated with a poor prognosis (Comiter et al., 1998; El Mesbahi et al., 2007). Only 4% of teratomas with somatic-type malignancy arise within the testis. The majority arise at metastatic sites, usually within 3 to 4 years after completion of chemotherapy as a conse quence of unresected teratoma (Magers et al., 2014; Rice et al., 2014). Lastly, unresected teratomas in patients with advanced NSGCT may result in late relapse (Sheinfeld, 2003). All of these events may have lethal consequences. Accurate characterization of GCTs is essential for successful treat ment, and consideration for expert pathology review may be con sidered. A study of orchiectomy specimens reviewed at Indiana University from outside institutions revealed a 31% discrepancy in histologic subtype and a change in lymphovascular invasion status in 22% of cases (Harari et al., 2017). These differences in patho logical assessment between expert and community pathologists may have important treatment implications
#29 . Patients frequently report a history of testicular trauma, though incidental trauma is likely responsible for bringing the testis mass to the patient’s attention for the first time. Patients may also complain of vague scrotal discomfort or heaviness. Regional or distant metastasis at diagnosis is present in approximately two thirds of NSGCT and 15% of pure seminomas, and symptoms related to metastatic disease are the presenting complaint in 10-20% of patients. Bulky retroperitoneal metastasis may cause a palpable mass, abdominal pain, flank pain caused by ureteral obstruction, back pain caused by involvement of the psoas muscle or nerve roots, lower extremity swelling caused by compression of the inferior vena cava, or gastrointestinal (GI) symptoms. Pulmo nary metastasis may present with dyspnea, chest pain, cough, or hemoptysis. Metastasis to supraclavicular lymph nodes may present as a neck mass. Approximately 2% of males have gynecomastia, resulting from either elevated serum hCG levels, decreased andro gen production, or increased estrogen levels (most commonly seen in patients with Leydig cell tumors). Although approximately two-thirds of males with GCT have diminished fertility, it is an uncommon initial presentation
#31 The physician should carefully examine the affected and the normal contralateral testis, noting their relative size and consistency and palpating for any testicular or extratesticular masses. Atrophy of the affected or contralateral testis is common, particularly in patients with a history of cryptorchidism. Any firm area within the testis should be considered suspicious for malignancy and should prompt further investigations. A hydrocele may accompany a testis cancer and impair the examiner’s ability to evaluate the testis. In this case, a scrotal ultrasound to evaluate the testis is warranted. The patient should also be examined for any evidence of palpable abdominal mass or pain, inguinal lymphadenopathy (particularly if he has had prior inguinal or scrotal surgery), gynecomastia, supraclavicular lymphadenopathy, and auscultation of the chest for intrathoracic disease
#33 tumors are initially misdiagnosed as epididymitis or hydrocele (Bosl et al., 1981). For patients who present with signs or symptoms from metastatic GCT, these may become the focus of the treating physician, resulting in the failure to diagnose GCT. These patients may be subjected to inappropriate treatment, diagnostic tests, and unnecessary surgery with subsequent delays in definitive therapy. Case reports describe patients undergoing exploratory laparotomy, neck dissection, or mastectomy for unsuspected metastatic GCT. The interval of delay is associated with advanced clinical stage, sub optimal response to chemotherapy, and diminished survival. Moul et al. reported a decrease in survival in GCT patients treated from 1970 to 1987 with a diagnostic delay greater than 16 weeks, though a significant survival difference was not observed among patients treated in the cisplatin era (Moul et al., 1990). Stephenson et al. reported a higher proportion of males requiring intensive chemotherapy (multiple regimens, high dose, and salvage chemotherapy) among those with a treatment delay greater than 30 days because of unnecessary exploratory laparotomy (Stephenson et al., 2004). Diagnostic delay can be avoided by efforts to improve patient and physician education. Physicians must consider the diagnosis of GCT in any male age 15 to 50 years with a firm testis mass, midline retroperitoneal mass, or mass in the left supraclavicular fossa
#37 At diagnosis, AFP levels are elevated in 50-70% of low-stage (CS I, IIA, IIB) NSGCT and 60-80% of advanced (CS IIC, III) NSGCT. EC and yolk sac tumors secrete AFP. Choriocarcinomas and seminomas do not produce AFP. Patients with pure semi noma in the primary tumor with an elevated serum AFP are considered to have NSGCT. The half-life of AFP is 5 to 7 days. AFP levels may also be raised in patients with hepatocellular carcinoma; cancers of the stomach, pancreas, biliary tract, and lung; nonmalig nant liver disease (infectious, drug-induced, alcohol-induced, auto immune); ataxic telangiectasia; and hereditary tyrosinemia.
#38 hCG levels are elevated in 20-40% of low-stage NSGCT and 40-60% of advanced NSGCT. Approximately 15% of seminomas secrete hCG. hCG is also secreted by choriocarcinoma and EC. Levels .5000 IU/L are usually associated with NSGCT. The half-life of hCG is 24 to 36 hours. hCG levels may be elevated in cancers of the liver, biliary tract, pancreas, stomach, lung, breast, kidney, and bladder. The a-subunit of hCG is common to several pituitary tu mors; thus, immunoassays for hCG are directed at the b-subunit. Cross-reactivity of the hCG assay with LH may cause false-positive hCG elevations in patients with primary hypogonadism. Elevated serum hCG results caused by hypogonadism will normalize within 48 to 72 hours after the administration of testosterone, and this can be done to distinguish between true- and false-positive hCG results. Marijuana use may also cause false-positive hCG results
#41 The prognosis of GCT and initial management decisions are dictated by the clinical stage of the disease, which is based on the histopathological findings and pathological stage of the primary tumor, postorchiectomy serum tumor marker levels, and the pres ence and extent of metastatic disease as determined by physical examination and staging imaging studies. In 1997, an international consensus classification for GCT was developed by the American Joint Committee on Cancer (AJCC) and Union Internationale Con tre le Cancer (UICC) (see Table 79.2). The AJCC and UICC staging systems for GCT are unique because, for the first time, a serum tu mor marker category (S) based on postorchiectomy AFP, hCG, and LDH levels is used to supplement the prognostic stages as defined by anatomic extent of disease. The AJCC and UICC staging systems were updated in 2002, and the new systems consider the presence of LVI in the primary as pT2 in an otherwise organ-confined tu mor. CS I is defined as disease clinically confined to the testis, CS II indicates the presence of regional (retroperitoneal) lymph node metastasis, and CS III represents nonregional lymph node and/or visceral metastasis.
#44 All patients with GCT should undergo staging imaging studies of the abdomen and pelvis. Computed tomography (CT) imaging with oral and intravenous contrast is the most effective, noninvasive means of staging the retroperitoneum and pelvis. CT imaging also provides a detailed anatomic assessment of the retroperitoneum to identify anomalies that may complicate subsequent RPLND, such as a circum-aortic or retro-aortic left renal vein, lower pole renal artery, or retrocaval right ureter. MRI is an alternative to CT, though it is associated with longer examination times, higher cost, and less availability. Enlarged retroperitoneal lymph nodes are found on CT in ap proximately 10-20% of seminomas and 60-70% of NSGCTs. The retroperitoneum continues to be the most difficult area to accurately stage clinically. A consistent 25-35% rate of pathologically involved retroperitoneal lymph nodes has been reported for CS I NSGCT in the presence of a “normal” CT scan despite the improvements in CT imaging over the past four decades (Fernandez et al., 1994). There is no consensus regarding size criteria for retro peritoneal lymph nodes that constitutes a “normal” CT scan. A size cutoff of 10 mm is frequently used to identify enlarged lymph nodes, but false-negative rates up to 63% have been reported when this size criterion is used. Among patients with CS IIA and IIB dis ease, clinical overstaging by CT (i.e., pathologically negative lymph nodes at RPLND despite enlarged lymph nodes on CT) is reported in 12-40% of patients. An understanding of the primary drainage sites for left- and right-sided tumors has led to efforts to increase the sensitivity of abdominal-pelvic CT imaging by decreasing the size criteria for clinically positive lymph nodes in the primary landing zone. Leibo vitch et al. showed that using a size cutoff of 4 mm in the primary landing zone and 10 mm outside this region was associated with a sensitivity and specificity for pathological stage II disease of 91% and 50%, respectively (Leibovitch et al., 1995). In a similar study, Hilton et al. reported a sensitivity and specificity of 93% and 58%, respectively, using a cutoff of 4 mm for lymph nodes in the primary landing zone that were anterior to a horizontal line bisecting the aorta (Hilton et al., 1997). Based on this evidence, retroperitoneal lymph nodes 5 to 9 mm in size in the primary landing zone should be viewed with suspicion for regional lymph node metas tasis, particularly if they are anterior to the great vessels on trans axial images (Fig. 79.3). Because of the rapid growth of GCT, it is advisable to base management decisions on CT imaging studies performed within 4 weeks of the initiation of treatment. In patients with normal serum tumor markers (hCG and AFP) and equivocal imaging findings for metastasis, clinicians may consider repeat im aging in 6 to 8 weeks to clarify the extent of disease before making a treatment recommendation. Malignant GCTs accumulate fluorodeoxyglucose (FDG), and several studies have investigated positron emission tomography (PET) in the staging of GCT at diagnosis and assessing response Fig. 79.3. Postorchiectomy CT abdomen-pelvis in a patient with right tes ticular nonseminoma germ cell tumor showing 7-mm lymph node in primary landing zone. The lymph node was involved with teratoma at retroperitoneal l
![12/14/2025 19
Spermatocytic
Tumor
• Spermatocytic tumor used to be classified as a
subtype of seminoma.
• Rare and accounts for less than 1% of GCTs.
• Do not arise from GCNIS, not associated with
cryptorchidism or bilaterality, does not
demonstrate i(12p),
• Do not stain for OCT 3/4, PLAP, or glycogen
(periodic acid–Schiff [PAS] stain)
• The peak incidence is the sixth decade of life.
• It is a benign tumor and is almost always cured
with orchiectomy.
• Exceptions - “spermatocytic tumor with sarcoma,”](https://image.slidesharecdn.com/41-251214180933-8435fa9e/75/creat-60-slides-from-the-pdf-for-acadamic-presentation-for-urology-resident-include-images-from-standard-urology-books-and-mention-video-links-from-youtube-to-be-included-in-the-slides-19-2048.jpg)
![12/14/2025 36
Serum tumor markers
• Few tumors associated with serum tumors
markers.
• (lactate dehydrogenase [LDH], AFP, and hCG) that
are essential in its diagnosis and management.
• at diagnosis before orchiectomy,
• after orchiectomy, to monitor for response to
chemotherapy,
• and to monitor for relapse in patients on
surveillance and after completion of therapy.](https://image.slidesharecdn.com/41-251214180933-8435fa9e/75/creat-60-slides-from-the-pdf-for-acadamic-presentation-for-urology-resident-include-images-from-standard-urology-books-and-mention-video-links-from-youtube-to-be-included-in-the-slides-36-2048.jpg)