Downloaded 71 times











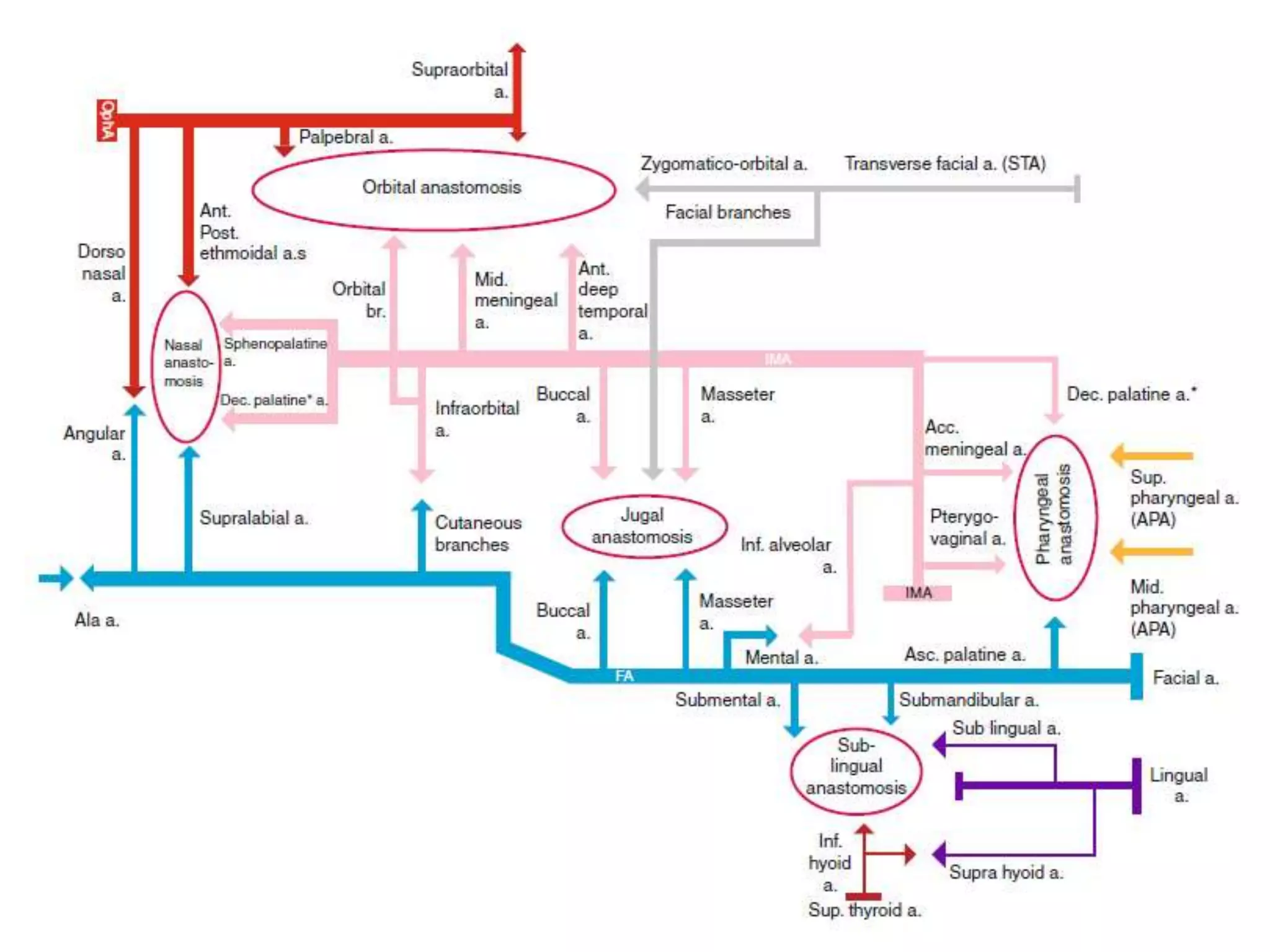

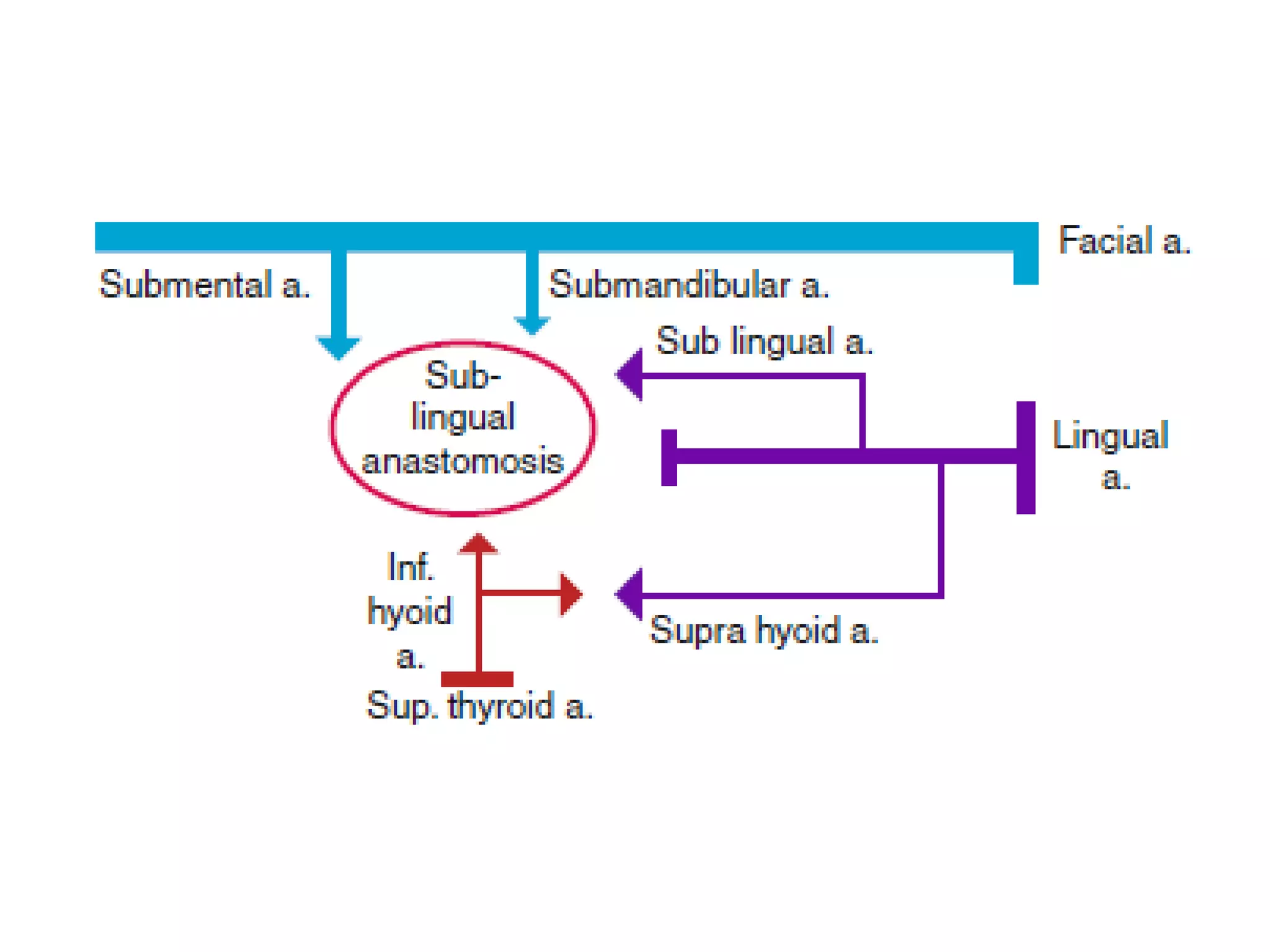

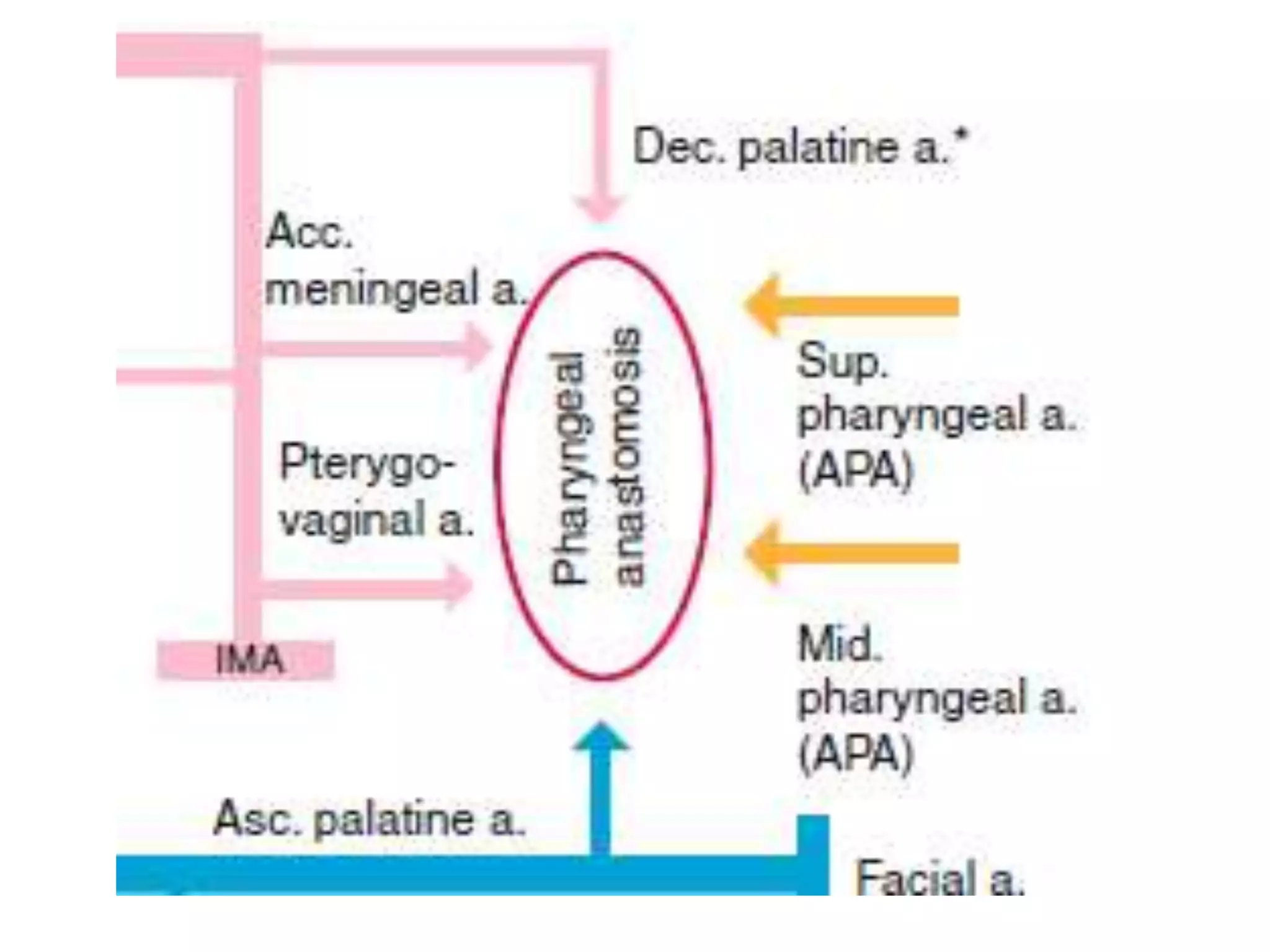


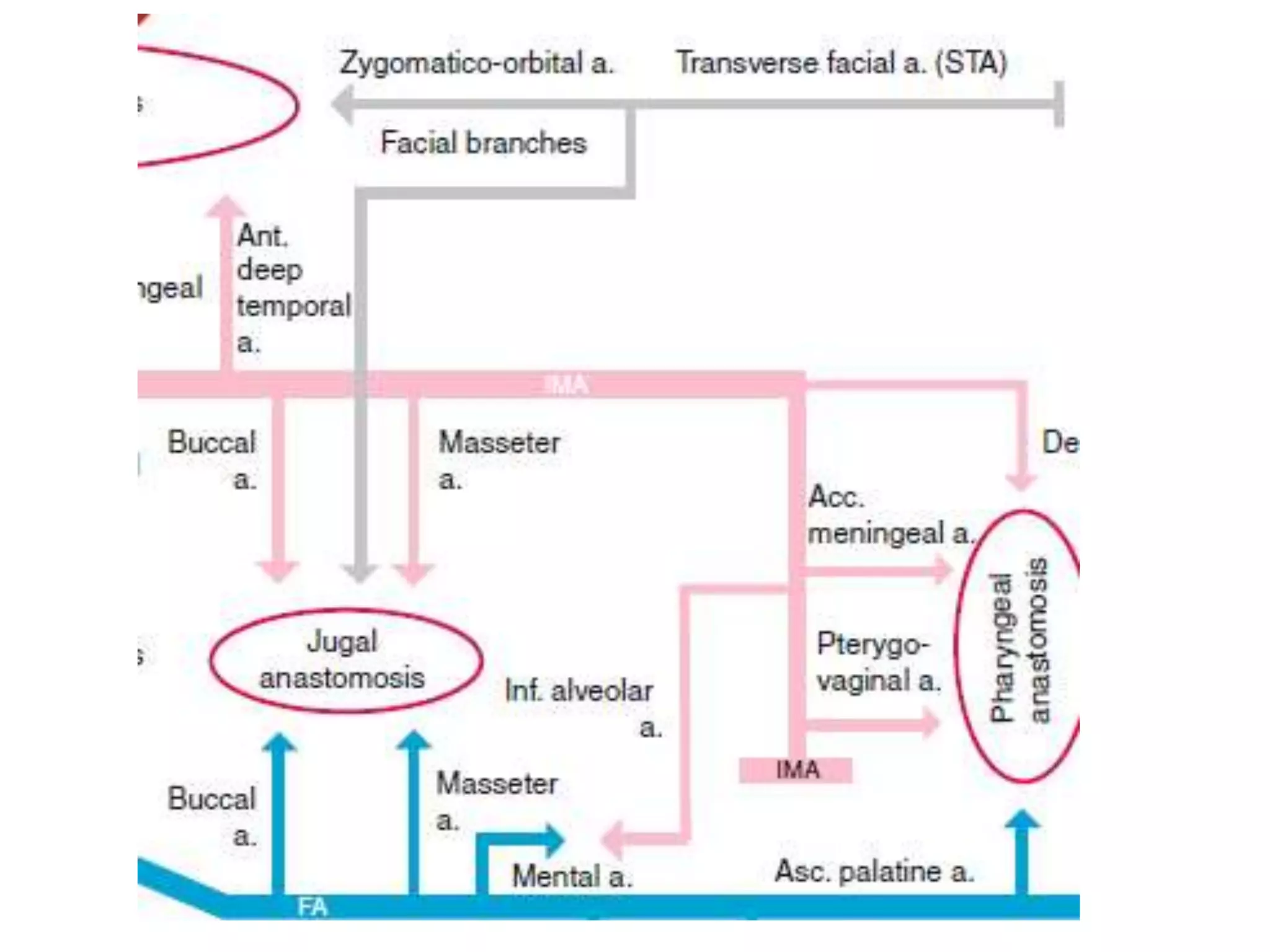



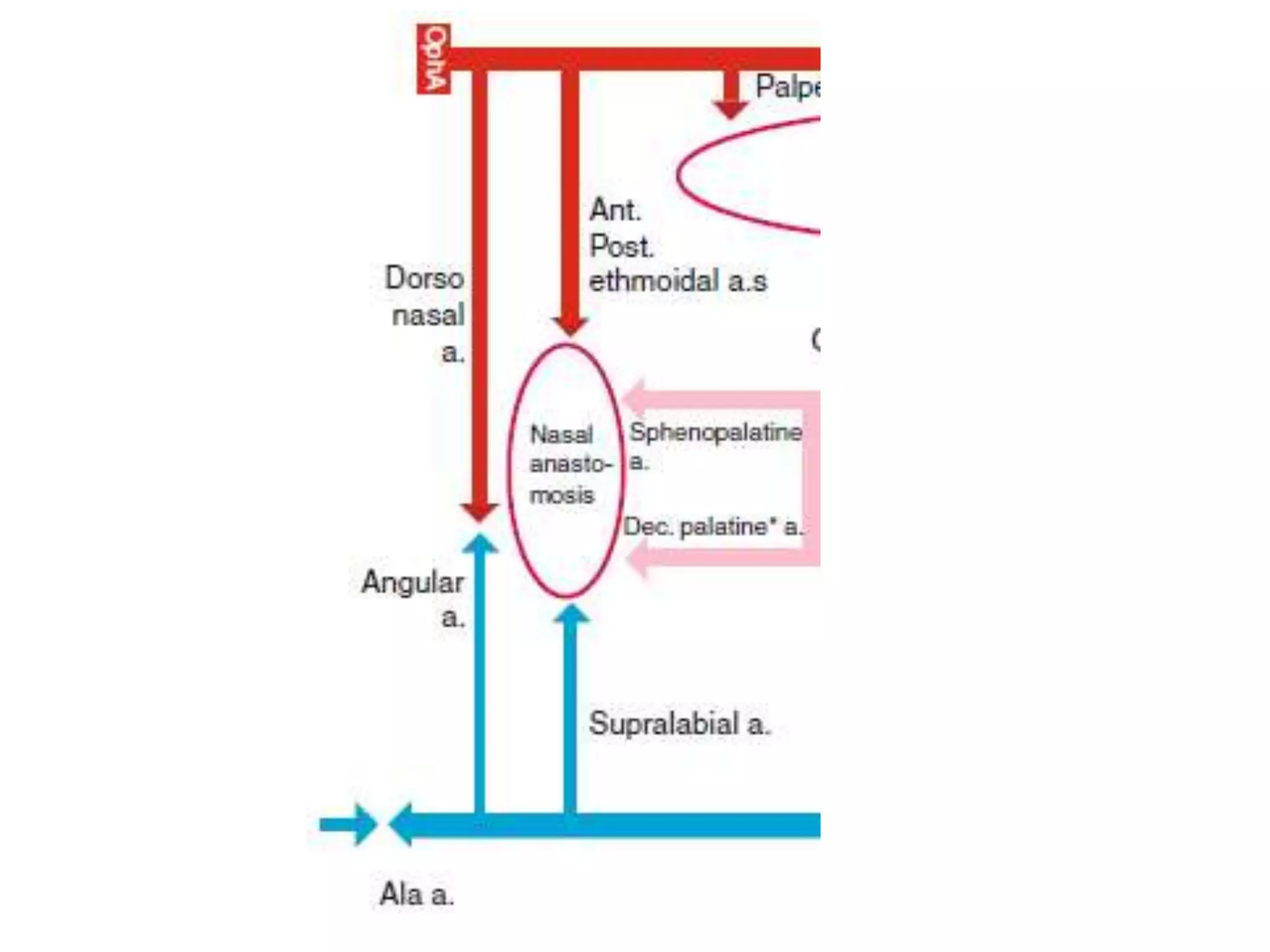


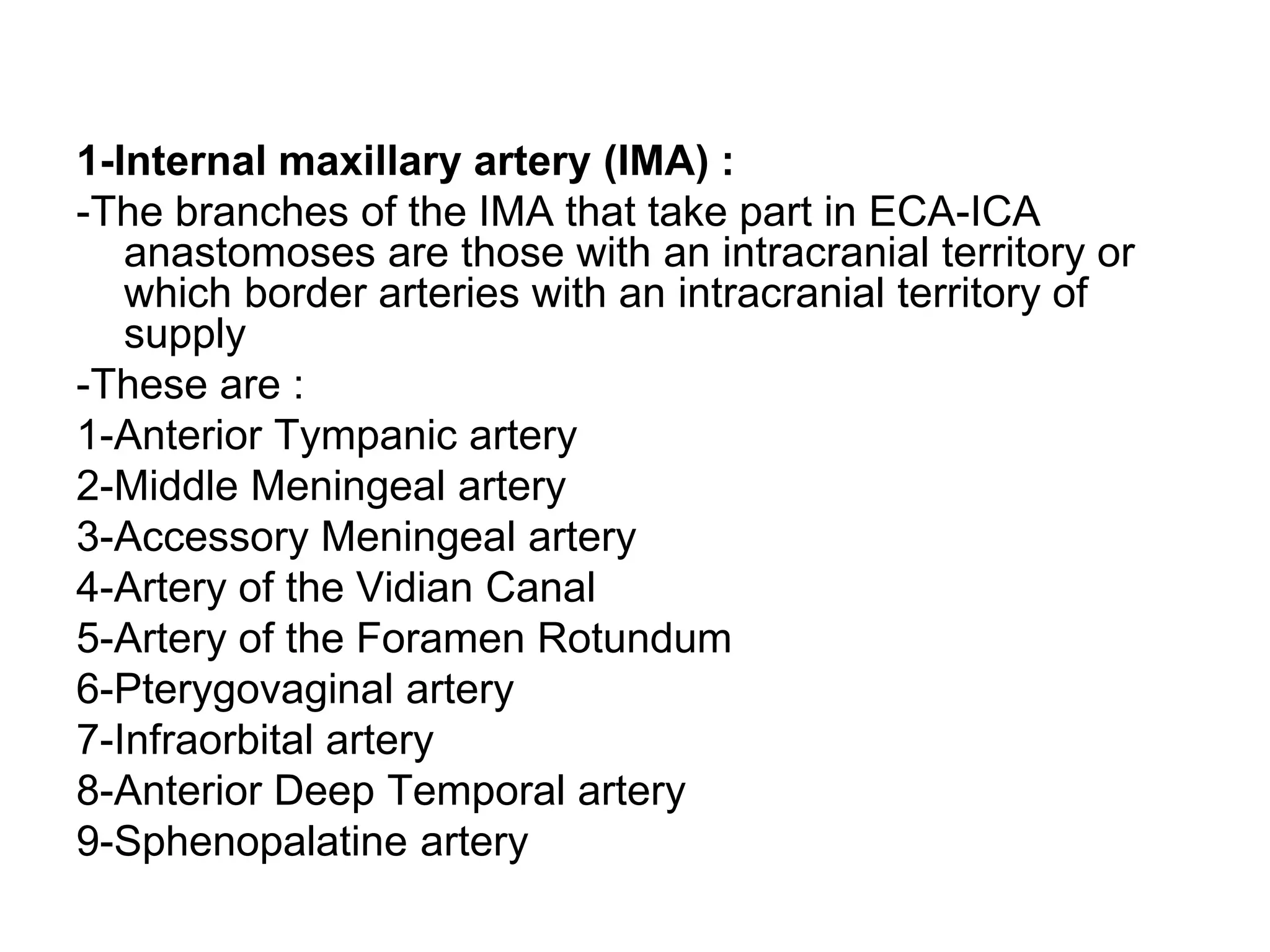





































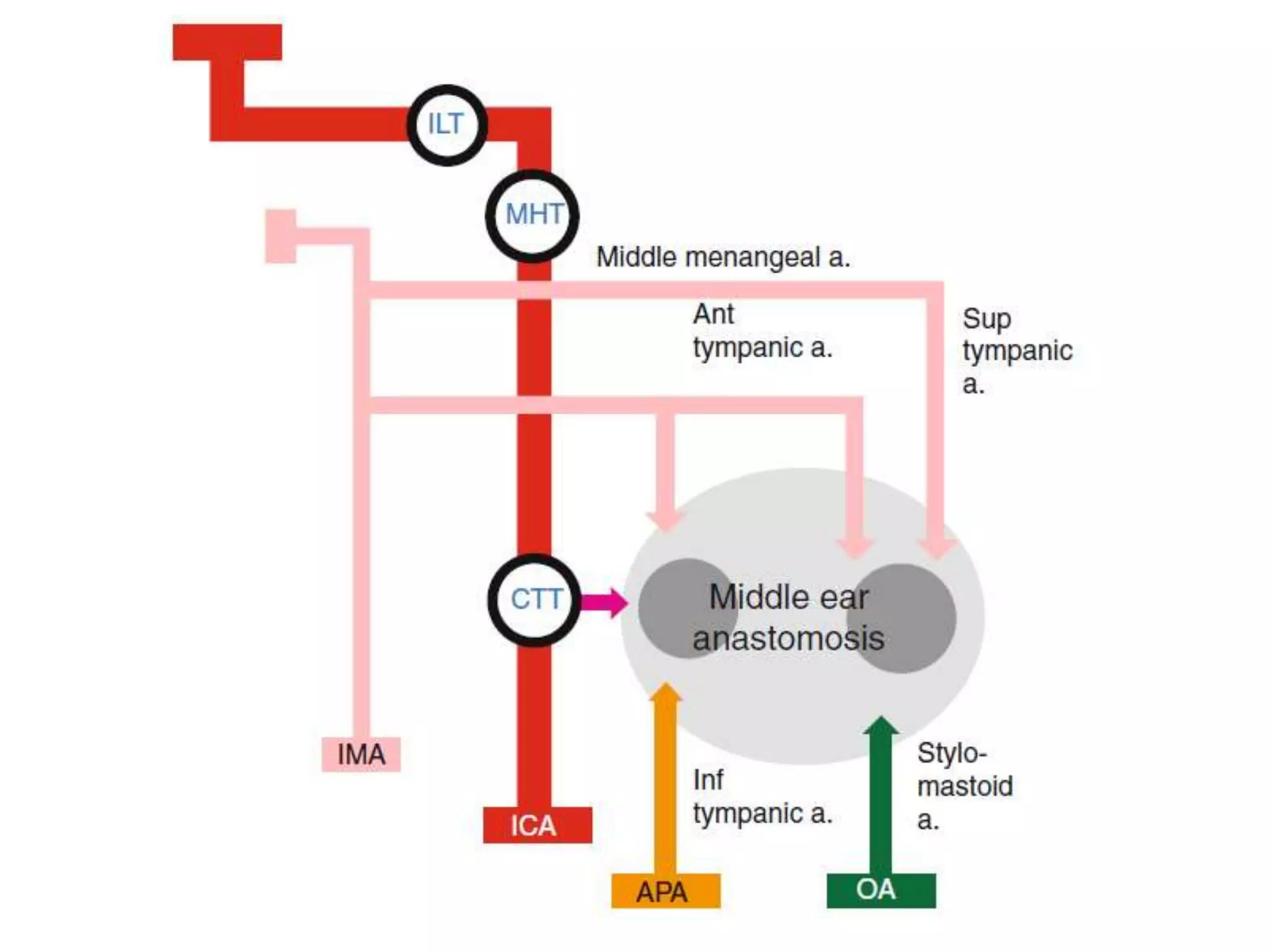















The document outlines cranial anastomoses and dangerous vascular connections involving the external carotid artery (ECA) and its branches, emphasizing their potential implications for interventional neuroradiology. It describes various anastomotic zones and connections between superficial and deep branches of the ECA, detailing the blood supply to critical anatomical regions such as the face and pharynx. The text serves as a comprehensive resource for understanding vascular structures crucial for surgical planning and interventions.























































































