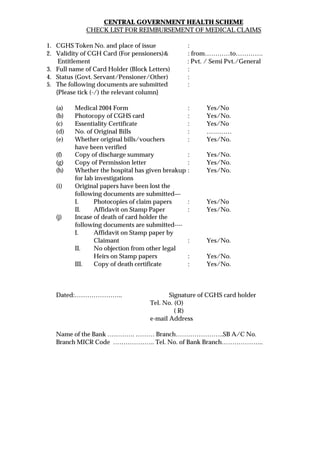
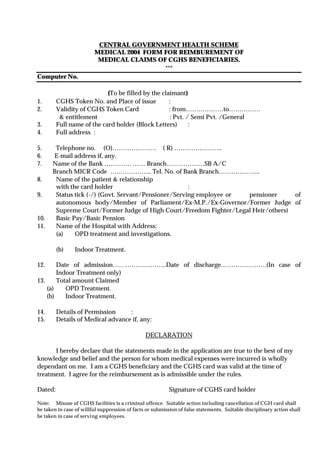
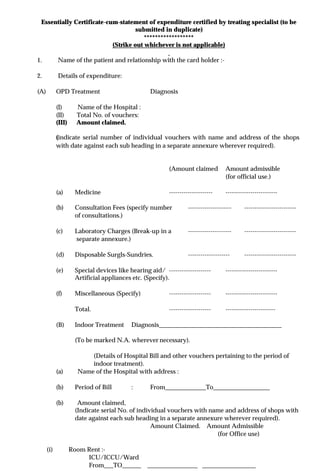
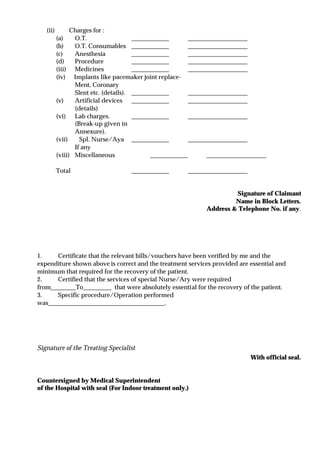
The document provides a checklist and guidelines for CGHS beneficiaries seeking reimbursement of medical claims from the Central Government Health Scheme. It outlines the required documents to submit such as medical forms, bills, lab reports, permission letters, and affidavits in some cases. It also lists information to include in the forms such as patient and card holder details, hospital details, treatment dates and costs. Beneficiaries must submit verified original bills and papers along with essentiality certificates from treating specialists to receive reimbursement according to approved rates.