- The document discusses blindness, its definitions, causes, and prevention efforts. It defines blindness according to the WHO as a visual acuity of less than 3/60 or the inability to count fingers from 3 meters away. The major causes of blindness globally and in India are cataract (62.6% in India), refractive error, and glaucoma.
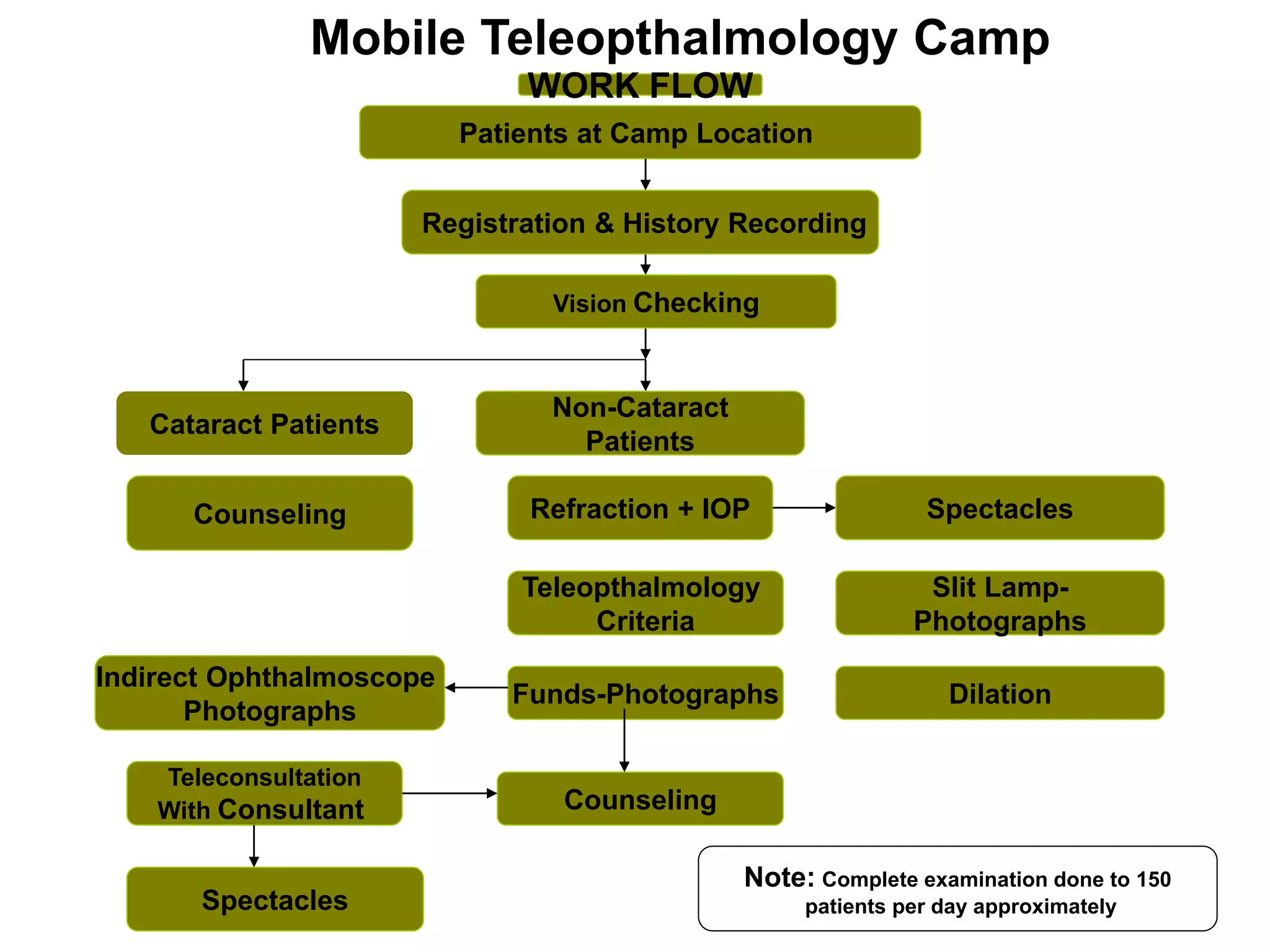
- The National Programme for Control of Blindness was launched in 1976 with goals of reducing blindness prevalence and expanding eye care coverage. It focuses on establishing facilities, training professionals, and increasing cataract surgeries. Recent efforts aim to address additional causes like childhood blindness and expand services through vision centers and mobile units. Ongoing challenges include epidemiological


![0.95%
3.05%
1.89%
1.52%
1.55%
1.61%
1.78%
2.28%
1.61%
1.42%
1.38%
1.19%
1.40%
1.16%
1.13%
1.07%
1.05%
1.01%
1.41%
0.94%
0.78%
0.78%
0.56%
0.78%
0.77%
0.74%
0.70%
0.65%
Prevalence of Blindness
State wise blindness prevalence [%]
National Survey [2001-02] [2003-04]
High Prevalence
Medium Prevalence
Low Prevalence](https://image.slidesharecdn.com/blindness-221126040853-63fdfda5/75/BLINDNESS-ppt-7-2048.jpg)