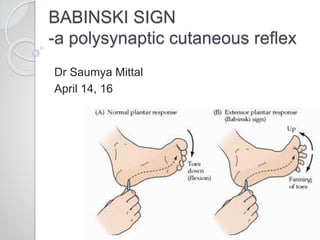
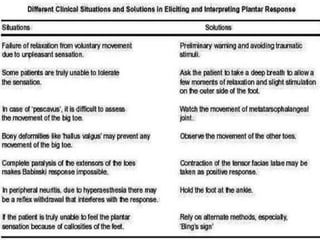
This document provides information about Babinski's sign, including its history, description, elicitation, types, problems, and other signs described by Babinski. It notes that Babinski sign is a polysynaptic cutaneous reflex first described by Joseph Babinski in 1896 for differentiating organic from psychogenic disorders. The document describes Babinski's background and contributions to neurology. It provides detailed instructions on properly eliciting the plantar reflex and discusses various characteristics and classifications of Babinski sign responses. It also outlines problems in interpretation and conditions where Babinski sign may be absent or present without CNS pathology.






































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)






![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)











