Downloaded 123 times


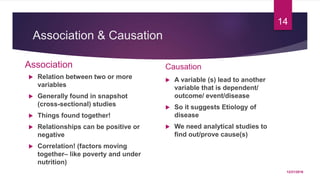
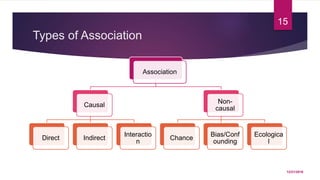
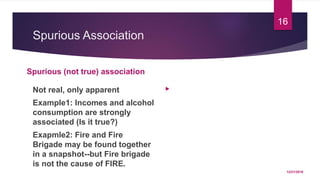
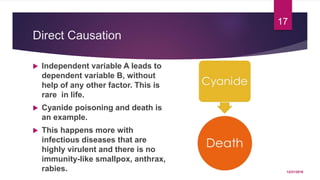
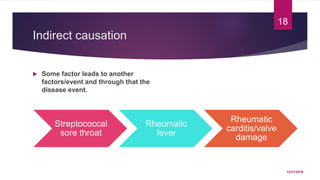
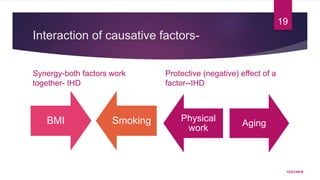
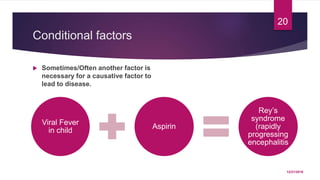
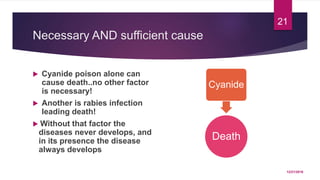
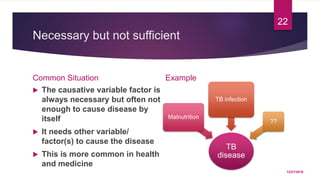
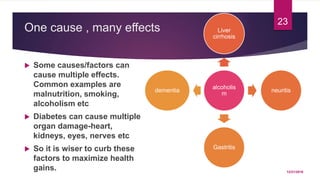
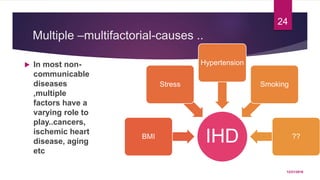
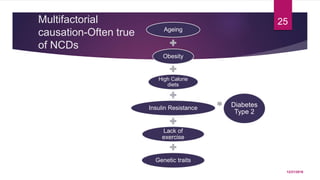
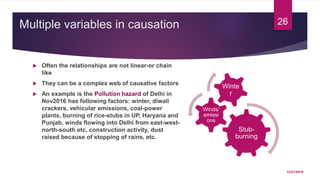

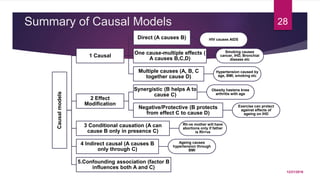


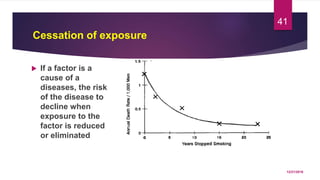
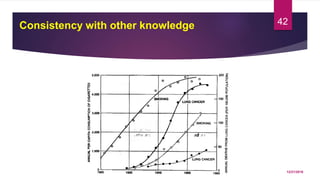

The document discusses key concepts in establishing causation in epidemiology, including the difference between association and causation. It explains that causation requires determining if a factor A truly causes outcome B rather than being a spurious relationship. Several of Hill's criteria for establishing a causal relationship are described, such as strength of association, consistency of findings, specificity of the relationship, and examining alternative explanations through study design and accounting for potential confounding factors. The document emphasizes that multiple factors often interact to cause outcomes, and that proving causation involves considering the strength and consistency of evidence rather than any single study.




























































































