Embryology of ArterialDevelopment
(Lower Limb)
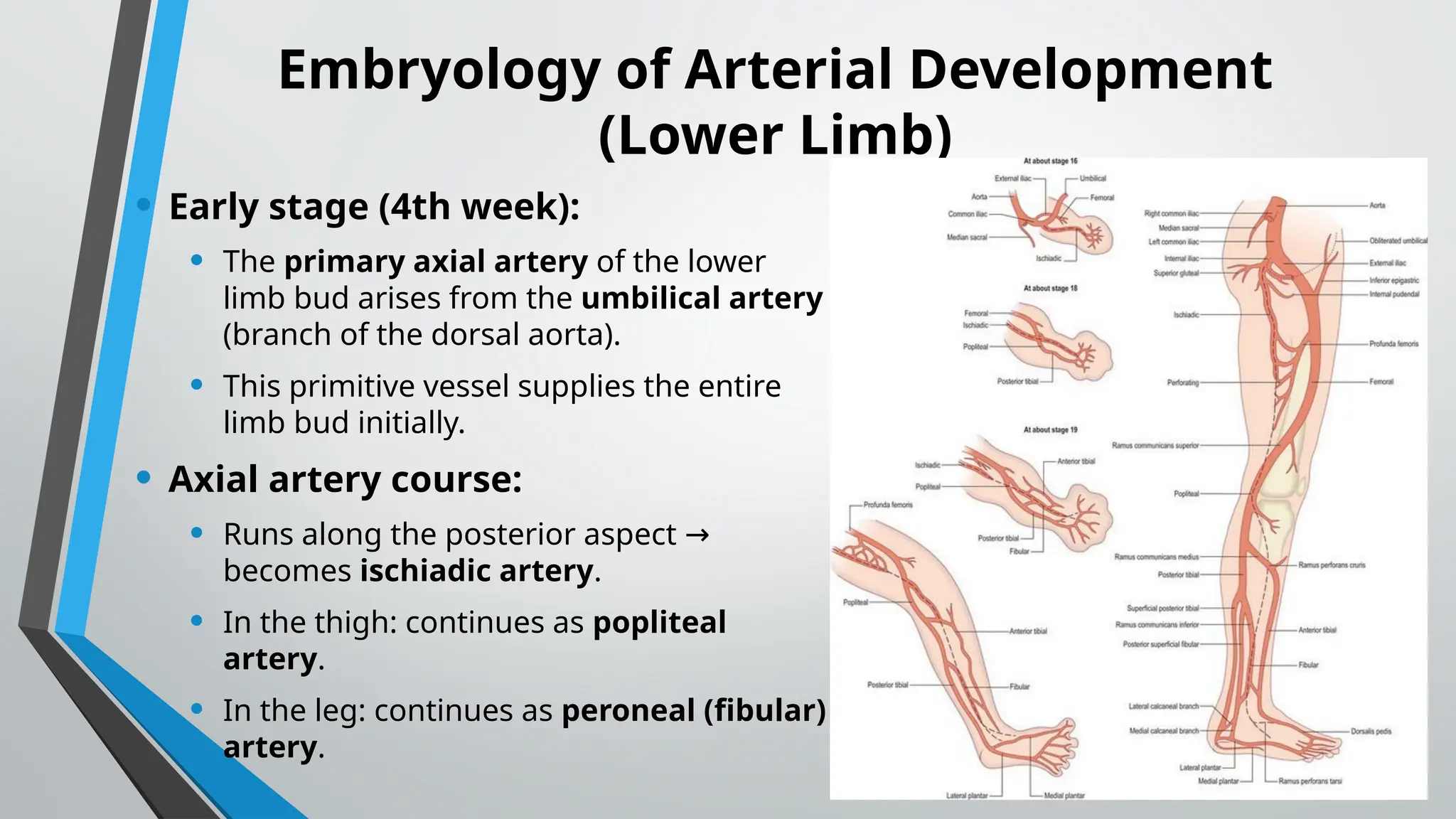
• Early stage (4th week):
• The primary axial artery of the lower
limb bud arises from the umbilical artery
(branch of the dorsal aorta).
• This primitive vessel supplies the entire
limb bud initially.
• Axial artery course:
• Runs along the posterior aspect →
becomes ischiadic artery.
• In the thigh: continues as popliteal
artery.
• In the leg: continues as peroneal (fibular)
artery.
4.
• Later remodeling(6th–8th weeks):
• Femoral artery develops as a new channel from the
external iliac artery.
• Femoral artery enlarges and takes over as the main
supply.
• Distal connections between femoral and popliteal
arteries persist.
• The original axial artery regresses, but remnants persist
as:
• Inferior gluteal artery (from internal iliac)
• Part of popliteal artery
• Fibular (peroneal) artery
• Adult arterial tree = remodeled system:
• External iliac femoral becomes dominant.
→
• Axial artery contributes to deep branches and fibular
artery.
5.
Embryology of VenousDevelopment
(Lower Limb)
• Early stage (5th week):
• Two longitudinal veins develop:
• Marginal vein (along lateral border)
• Axial vein (posterior, accompanies axial artery)
• Remodeling:
• Cranial portion of axial vein femoral vein
→ .
• Caudal portion of axial vein popliteal & posterior tibial
→
veins.
• Marginal vein great saphenous vein (medial side) and
→
small saphenous vein (lateral side).
• Final venous anatomy:
• Superficial system = derived from marginal vein.
• Deep system = derived from axial vein.
• Numerous anastomoses perforators (important in varicose
→
vein pathology).
6.
ARTERIES OF LOWERLIMB
• The main artery of the lower limb is the
Femoral artery.
• It is a continuation of the External iliac
artery (terminal branch of the abdominal
aorta).
• The external iliac becomes the femoral
artery when it crosses under the inguinal
ligament and enters the femoral triangle.
7.
In the femoraltriangle, the profunda
femoris artery arises from the
posterolateral aspect of the femoral artery.
• Perforating branches - Consists of three
or four arteries that perforate the
adductor magnus, contributing to the
supply of the muscles in the medial and
posterior thigh.
• Lateral femoral circumflex artery -
Wraps round the anterior, lateral side of
the femur, supplying some of the muscles
on the lateral aspect of the thigh.
• Medial femoral circumflex artery -
Wraps round the posterior side of the
femur, supplying Its neck and head. In a
fracture of the femoral neck this artery can
easily be damaged, and avascular necrosis
of the femur head can occur.
8.
• After exitingthe femoral triangle, the
femoral artery continues down the
anterior aspect of the thigh, through
a tunnel known as the adductor
canal. During its descent, the artery
supplies the anterior thigh muscles.
• The adductor canal ends at an
opening in the adductor magnus,
called the adductor hiatus. The
femoral artery moves through this
opening, and enters the posterior
compartment of the thigh, proximal
to the knee. The femoral artery is
now known as the popliteal artery
9.
Arteries of LowerLimb – Knee & Leg
• The popliteal artery descends down the
posterior thigh, giving rise to genicular
branches that supply the knee joint. It moves
through the popliteal fossa, exiting between
the gastronemius and popliteus muscles.
• At the lower border of the popliteus, the
popliteal artery terminates by dividing into
the anterior tibial artery and the tibio-
peroneal trunk.
• The tibio-peroneal trunk bifurcates into the
posterior tibial and fibular arteries.
10.
Arteries of LowerLimb - Leg
• Posterior tibial artery - continues inferiorly, along
the surface of the deep posterior leg muscles (such
as tibialis posterior). It enters the sole of the foot
via the tarsal tunnel, accompanying the tibial nerve.
• Fibular (peroneal) artery - descends posteriorly to
the fibula, within the posterior compartment of the
leg. it gives rise to perforating branches, which
penetrate the intermuscular septum to supply
muscles in the lateral compartment of the leg.
• The other division of the popliteal artery, the
anterior tibial artery, passes anteriorly between the
tibia and fibula, through a gap in the interosseous
membrane. It then moves inferiorly down the leg. It
runs down the entire length of the leg, and into the
foot, where it becomes the dorsalis pedis artery
11.
ANTERIOR TIBIAL ARTERY
Arterypresent in the anterior compartment of leg.
Passes anteriorly between Tibia and Fibula & runs
down anterolateral aspect of Tibia
Origin: branch of popliteal artery
Course: runs in the anterior compartment of leg -
deep peroneal nerve
Termination: Continues as dorsalis pedis artery at
the ankle joint Branches:
Anterior and posterior tibial recurrent arteries
Muscular arteries
Medial and Lateral malleolar arteries
12.
POSTERIOR TIBIAL ARTERY
Situatedin the posterior compartment
of leg
• Origin: Branch of popliteal artery
• Course: Runs down in the posterior
compartment of leg between superficial
and deep muscles
• Accompanied by tibial nerve
• CT Angiography(CTA)
Gold standard non-invasive
modality for peripheral arterial
mapping.
Protocol:
• Thin slices, bolus-tracking (arterial
phase).
• Run-off from aorta feet.
→
Strengths: high-resolution,
calcifications, 3D reconstructions
(MIP, VR).
Uses: PAD, trauma, aneurysm, pre-
surgical planning.
Lower-extremity CT angiography
showed occlusion of the right popliteal
artery
16.
• MR Angiography(MRA)
Good for patients with renal
failure (non-contrast TOF, PC
techniques) or contrast (CE-
MRA).
Strengths: no radiation, soft-
tissue detail.
Limitations: motion artifacts,
metallic implants, longer exam
time.
17.
• Digital SubtractionAngiography
(DSA)
Gold standard invasive technique.
Advantages: high-resolution,
dynamic flow.
Key role: not just diagnostic but
therapeutic angioplasty, stenting,
→
thrombolysis, embolization.
Classic angiographic signs in PAD:
• Tapering occlusion, collaterals, string
sign.
Digital subtraction angiography
image shows focal, well-defined,
severe stenosis and lateral deviation
of popliteal artery bilaterally (arrows).
18.
• Pathologies onImaging
oAtherosclerotic PAD – most common.
oAcute limb ischemia – thromboembolism, trauma.
oAneurysms – especially popliteal (most common peripheral aneurysm).
oArteriovenous malformations/fistulas – congenital or traumatic.
oEntrapment syndromes – e.g., Popliteal artery entrapment.
oDiabetic angiopathy – distal small vessel involvement.
19.
Lower Limb VenousDrainage
The venous drainage of the lower limb is divided into:
• Superficial veins (outside the deep fascia)
• Deep veins (accompany arteries, venae comitantes)
• Perforator veins (connect superficial to deep system, with valves to ensure
unidirectional flow)
• Clinical importance in Radiology:
Varicose veins, DVT, venous insufficiency, venous mapping before
bypass grafting, Doppler evaluation.
20.
Factors helping venousreturn
• Negative intra-thoracic pressure.
• Transmitted pulsations from adjacent arteries. Valves maintain
unidirectional flow.
• Valves in perforating veins prevent reflux into low pressure
superficial veins.
• Calf Pump—Peripheral Heart.
• Vis-a-tergo produced by contraction of heart. Suction action of
diaphragm during inspiration.
21.
Dorsal Venous Archof Foot
• It lies in the subcutaneous tissue over
the heads of metatarsals with convexity
directed distally.
• It is formed by union of 4 dorsal
metatarsal veins.
• Each dorsal metatarsal vein receives
blood in the clefts from dorsal digital
veins and proximal & distal perforating
veins conveying blood from plantar
surface of sole.
22.
PLANTAR VENOUS ARCHFOOT
•Formation – plantar digital veins →
plantar metatarsal veins → form the
deep plantar venous arch in the
sole.
•Drainage – gives rise to medial &
lateral plantar veins, which unite
behind the medial malleolus →
posterior tibial veins.
•Connections – communicates with
dorsal venous arch via perforators
(deep → superficial in foot).
•Function – drains deep sole veins,
helps in venous return with plantar
muscle pump.
23.
GREAT SAPHENOUS VEIN
•Longest vein in the body.
• COURSE-
Begins from the medial side of dorsal venous arch.
Supplemented by medial marginal vein
Ascends 2.5 cm anterior to medial malleolus.
Passes posterior to medial border of patella.
Ascends along medial thigh.
Penetrates deep fascia of femoral triangle:
Pierces the Cribriform fascia & Saphenous opening.
Drains into femoral vein.
24.
Great Saphenous VeinTributaries
These veins typically join near the
saphenofemoral junction (SFJ) and along the
thigh, draining into the femoral vein.
Superficial epigastric vein
Superficial circumflex iliac vein
Superficial external pudendal vein
Deep external pudendal vein
Anterior (accessory) saphenous vein (AASV)
Posterior accessory saphenous vein (PASV)
Posterior arch vein
Medial marginal vein
Giacomini vein
Perforators - Cockett (lower leg), Boyd (knee
level), Dodd (thigh) connect GSV with deep
veins.
Valves: 10–20, important for competency in
25.
SHORT SAPHENOUS VEIN
Drainslateral side of dorsal venous arch.
Passes posterior to lateral malleolus.
Accompanies sural nerve. Ascends along midline of
calf.
Empties into popliteal vein in popliteal fossa.
• Imaging relevance:
GSV & SSV often used for CABG grafts.
Varicosity most common in GSV distribution.
26.
• Type A:normal SPJ located , 5 cm above the crease (83%): Type A1: without
a common trunk with the medial gastrocnemial veins (62%); Type A2: with
a common trunk with the medial gastrocnemial veins (21%). Type B: high
SPJ, 5 cm above the crease (6%); Type C: no SPJ, SSV extension by
≥
Giacomini vein (5%); Type D: no SPJ, short termination at the level of the leg
(1%);Type E:no SPJ, plexiform deep termination in the thigh muscles (5%)
27.
DEEP VEINS
• Presentwithin the deep fascia surrounded
by powerful muscles.
• Blood flow in greater pressure and volume.
• Accounts for 80 -90% venous return.
• Accompany arteries
• Paired venae comitantes accompany
arteries below knee.
• Unpaired veins above knee.
28.
• Foot andLeg
The main venous structure of the foot is
the dorsal venous arch, which mostly
drains into the superficial veins. Some
veins from the arch penetrate deep into
the leg, forming the anterior tibial vein.
On the plantar aspect of the
foot, medial and lateral plantar veins
arise. These veins combine to form the
posterior tibial and fibular veins.
The posterior tibial vein accompanies
the posterior tibial artery, entering the leg
posteriorly to the medial malleolus.
On the posterior surface of the knee, the
anterior tibial, posterior tibial and fibular
veins unite to form the popliteal vein.
The popliteal vein enters the thigh via the
adductor canal.
29.
• Thigh
Once thepopliteal vein has entered
the thigh, it is known as the femoral
vein. It is situated anteriorly,
accompanying the femoral artery.
The deep vein of the thigh (profunda
femoris vein) is the other main venous
structure in the thigh. Via perforating
veins, it drains blood from the thigh
muscles. It then empties into the
distal section of the femoral vein.
The femoral vein leaves the thigh by
running underneath the inguinal
ligament, at which point it is known as
the external iliac vein.
30.
PERFORATORS
• Connect superficialto deep system.
• Contain valves (direct blood deep system)
→
• Fairly constant in position:
1. 1 lateral ankle perforators
2. 3 Medial ankle perforators
a) Posteroinferior to medial malleolus
b) 10 cm above medial malleolus
c) 15 cm above medial malleolus
3. Gastrocnemius perforators of Boyd around knee
4. Mid thigh perforators of Dodd
5. Hunterian perforator in thigh
31.
• Venous Valves
Presentin both superficial & deep
veins.
Function: Prevent reflux, direct
blood toward heart.
Clinical: Valve incompetence →
varicose veins.
Doppler: demonstrated by reflux
>0.5 sec.
32.
Venous Communications inLower Limb
1. Foot (Sole Dorsum)
↔
Deep Superficial
→
• In the sole, we mainly have deep veins:
• Plantar digital plantar metatarsal
→ → plantar venous arch
• These drain into deep veins (medial & lateral plantar veins posterior tibial
→
vein).
But: perforating veins pass from deep plantar veins dorsal
→
venous arch (superficial system).
• Thus, in the foot: flow is Deep Superficial
→ (through perforators in sole).
This is opposite to the leg & thigh.
33.
2. Leg andThigh
Here, the superficial deep
→ connection predominates.
Superficial veins (GSV, SSV) connect to deep veins (femoral,
popliteal, tibial veins) via perforators.
Flow:
• From superficial deep system
→
• Ensured by valves in perforators (prevent reflux).
Examples:
• Cockett’s perforators (leg)
• Boyd’s perforator (below knee)
• Dodd’s & Hunterian (thigh)
34.
• Doppler Ultrasound-
First-linefor evaluation
of DVT, reflux,
mapping.
Uses:
• Compression
technique for DVT.
• Color Doppler for
flow direction &
reflux.
• Spectral Doppler for
augmentation,
Valsalva.
35.
• CT /MR Venography-
Used in pelvic vein thrombosis, venous anomalies, pre-surgical mapping.
MRV: no radiation, contrast or non-contrast (TOF, PC).




















































![Lymphatic system [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/lymphaticsystemautosaved-180608144519-thumbnail.jpg?width=640&height=640&fit=bounds)




































































