Learning Outcomes
• Recapon anatomy and physiology of appendix
• Conditions affecting the appendix - appendicitis, neoplasms
• Appendicectomy - emergency vs delayed (interval)
• Appendicectomy - open vs laparoscopic
• Take Home Message
3.
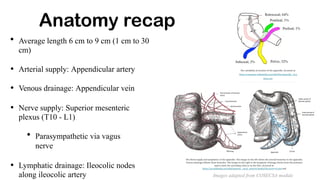
Anatomy recap
• Averagelength 6 cm to 9 cm (1 cm to 30
cm)
• Arterial supply: Appendicular artery
• Venous drainage: Appendicular vein
• Nerve supply: Superior mesenteric
plexus (T10 - L1)
• Parasympathetic via vagus
nerve
• Lymphatic drainage: Ileocolic nodes
along ileocolic artery Images adapted from COSECSA module
4.
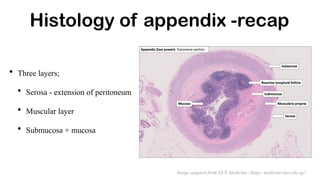
Histology of appendix-recap
• Three layers;
• Serosa - extension of peritoneum
• Muscular layer
• Submucosa + mucosa
Image adapted from NUS Medicine //https: medicine.nus.edu.sg//
5.
Physiology
• NOT avestigial organ
• It is an IMMUNOLOGIC ORGAN
• Maturation of B lymphocytes
• Actively participates in secretion of immunoglobulins especially IgA
• Reservoir to recolonise the colon with healthy bacteria
• Males >females ( 8.6% ; 6.7%)
• Incidence in general population - worldwide : 0.1 % - 0.2 %
• Incidence in Uganda - 7.7 % (AG Marion, 2018)
Appendicitis - epidemiology
AG Marion, et al, 2018, The Use of Alvarado Score In Diagnosis of Acute Appendicitis at Jinja Regional Referral Hospital
8.
Appendicitis - microbiology
•More anaerobes compared to normal appendix
• Cultures tend to grow;
- Escherichia coli
- Bacteroides species
- Fusobacterium nucleatum / necrophorum (62%)
Others: Peptostreptococcus, Pseudomonas species, Bacteroides sphlanchnicus, Bacteroides
intermedius, Lactobacillus
9.
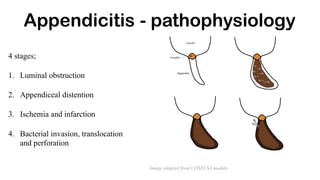
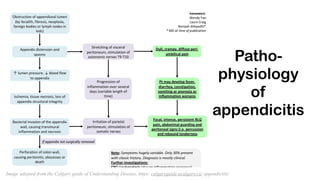
4 stages;
1. Luminalobstruction
2. Appendiceal distention
3. Ischemia and infarction
4. Bacterial invasion, translocation
and perforation
Appendicitis - pathophysiology
Image adapted from COSECSA module
• Peri-umbilical diffusepain which later localises to right lower quadrant (sens. 81%,
spec, 53%)
• Nausea
• Vomiting
• Anorexia
• Obstipation prior to pain + sensation that defecation will relieve the pain
• Diarrhea in children - related to perforation
Appendicitis - clinical features
12.
• General exam
•Altered or normal vital signs
• Slow movements - related to peritonitis
• Specific exam
• Point of maximum tenderness at
McBurney’s point
• Signs of peritonism
Appendicitis - clinical picture
Sensitive signs;
• McBurney sign
• Rovsing sign
• Obturator sign
• Psoas sign
• Dunphy sign
• Markle sign
13.
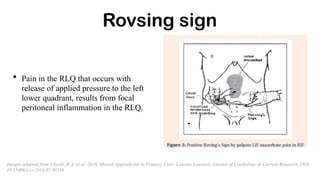
Rovsing sign
• Painin the RLQ that occurs with
release of applied pressure to the left
lower quadrant, results from focal
peritoneal inflammation in the RLQ.
Images adapted from Ubaidi, B A, et al, 2016, Missed Appendicitis in Primary Care: Lessons Learned, Journal of Cardiology & Current Research, DOI:
10.15406/jccr.2016.07.00256
14.
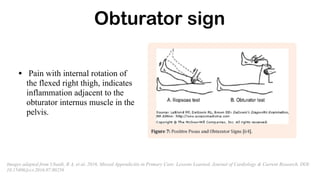
Obturator sign
• Painwith internal rotation of
the flexed right thigh, indicates
inflammation adjacent to the
obturator internus muscle in the
pelvis.
Images adapted from Ubaidi, B A, et al, 2016, Missed Appendicitis in Primary Care: Lessons Learned, Journal of Cardiology & Current Research, DOI:
10.15406/jccr.2016.07.00256
15.
Psoas sign
• Painwith right hip flexion, can be seen
with a retrocecal appendix due to
inflammation adjacent to the iliopsoas
muscle group.
Images adapted from Ubaidi, B A, et al, 2016, Missed Appendicitis in Primary Care: Lessons Learned, Journal of Cardiology & Current Research, DOI:
10.15406/jccr.2016.07.00256
16.
Dunphy sign
• Increasedabdominal pain on coughing
• This is due to jostling of inflamed peritoneum
• More specific in paediatric age group
Appendicitis in young
•Presentation: Diffuse abdominal pain
• Clinically: Generalized lymphadenopathy + voluntary guarding + tenderness
• Specific signs and rigidity are RARE
• Paed specific signs: pain with percussion, pain on coughing, hopping / refusal to use
right lower limb
• Negative appendicectomy rates: < 5 years - 25%, 5 - 12 years - 10%
• Appendiceal rupture rates: < 5 years : 46%, 5 - 12 years : 20%
• Differential diagnosis: Acute mesenteric adenitis
• Management: Immediate appendicectomy (if ruptured), early appendicectomy (if
20.
Appendicitis in theelderly
• Presentation: Lower abdominal pain
• Clinically: Localization of right lower quadrant tenderness IS NOT common
• Differential diagnoses: - Acute diverticulitis
- Perforating carcinoma of caecum / sigmoid colon
• Investigations - Contrasted CT scan of abdomen
- Internal surveillance of colon - colonoscopy / barium enema
Management : Laparoscopic appendicectomy preferred (if temp > 38C, left shift of
leucocytes in anorexic male with long duration of pain prior to admission)
21.
Appendicitis in pregnant
•Incidence: 1 in 766 live births
• Can occur at any time in pregnancy but is rare in 3rd trimester
• Clinical features: Sudden onset right sided abdominal pain
• Investigations: MRI scan of abdomen
• Management: Appendicectomy
• Risks of appendicectomy: Laparoscopic - 2.31 increased risk of fetal loss compared to
open
• Risk of fatal loss after appendicectomy: 4%
• Risk of early delivery after appendicectomy: 7% - 10%
22.
• Incidence: 0.5%
•Increased risk of appendiceal rupture (43% at presentation)
• Clinical features: - Peri-umbilical pain radiating to right lower quadrant
(91%)
-Rebound tenderness (74%)
+/ - Fever
• Investigations: Relative leucocytosis
• Differential diagnosis: Opportunistic infections + neutropenic enterocolitis
(typhilitis)
Appendicitis in HIV population
Alvarado score [5]
•Score < 3: Low likelihood of
appendicitis
• Score : 4 - 6: consider
further imaging
• Score >=7 : High likelihood of
appendicitis
• Inconsistent in children and
women
• Sensitivity for ruling out > ruling in
Component Maximum score
Migration of pain to right
lower quadrant
Anorexia
Nausea / Vomiting
Fever > 37.3 C
Right iliac fossa tenderness
Rebound tenderness
Leucocytosis > 10 x 10
^9 Left shift of neutrophils
MAXIMUM TOTAL
1
1
1
1
2
1
2
1
10
25.
Tzanakis score [9]
•Circa 2005
• Score > 8 = diagnostic of
acute appendicitis
• Sensitivity:95.4%
• Specificity: 97.4%
Parameter Score
Presence of right
lower abdominal 4
tenderness
Rebound tenderness 3
Laboratory findings:
WBC > 12,000
2
Ultrasound finding:
Indicative of 6
appendicitis
Total 15
26.
Appendicitis Inflammatory
Response Score(AIRS) [11]
• 0 - 4: Low probability - OPD
follow-up
• 5 - 8: Indeterminate - Active
observation / Diagnostic
laparoscopy
• 9-12: High probability - Surgical
exploration
Findings Score
Vomiting 1
Right inferior fossa pain 1
Rebound tenderness /
muscular defence
Light : 1
Medium : 2
Strong : 3
Body temp >= 38.5 C 1
Polymorphonuclear
leucocytes
70% - 84% :1
>= 85% : 2
White Blood Cell count
10.0 - 14.9 x 10^9 : 1
>=15 x 10^9 :
2
C-reactive protein
concentration
10 - 49 : 1
>=50 : 2
MAXIMUM TOTAL 12
27.
RIPASA Score
[12]
• Includes;age, gender, duration of symptoms
prior to presentation.
• Circa 2014
• More accurate among Asian population
• Sensitivity = 96.7%
• Specificity = 93%
• Diagnostic accuracy = 95.1 %
• Score > 7.5 - significant for appendicitis
28.
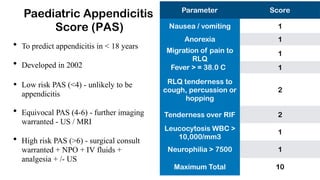
Paediatric Appendicitis
Score (PAS)
•To predict appendicitis in < 18 years
• Developed in 2002
• Low risk PAS (<4) - unlikely to be
appendicitis
• Equivocal PAS (4-6) - further imaging
warranted - US / MRI
• High risk PAS (>6) - surgical consult
warranted + NPO + IV fluids +
analgesia + /- US
Parameter Score
1
1
1
1
Nausea / vomiting
Anorexia
Migration of pain to
RLQ
Fever > = 38.0 C
RLQ tenderness to
cough, percussion or
hopping
2
2
1
Tenderness over RIF
Leucocytosis WBC >
10,000/mm3
Neurophilia > 7500 1
Maximum Total 10
29.
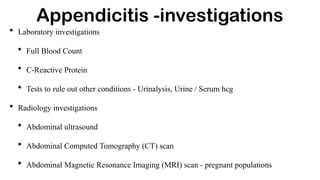
• Laboratory investigations
•Full Blood Count
• C-Reactive Protein
• Tests to rule out other conditions - Urinalysis, Urine / Serum hcg
• Radiology investigations
• Abdominal ultrasound
• Abdominal Computed Tomography (CT) scan
• Abdominal Magnetic Resonance Imaging (MRI) scan - pregnant populations
Appendicitis -investigations
30.
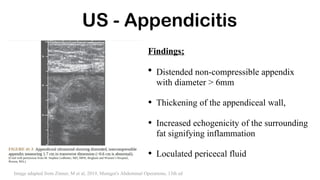
US - Appendicitis
Findings;
•Distended non-compressible appendix
with diameter > 6mm
• Thickening of the appendiceal wall,
• Increased echogenicity of the surrounding
fat signifying inflammation
• Loculated pericecal fluid
Image adapted from Zinner, M et al, 2019, Maingot's Abdominal Operations, 13th ed
31.
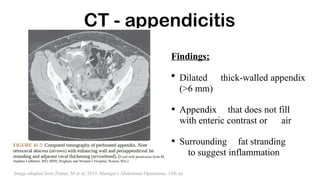
CT - appendicitis
Findings;
•Dilated thick-walled appendix
(>6 mm)
• Appendix that does not fill
with enteric contrast or air
• Surrounding fat stranding
to suggest inflammation
Image adapted from Zinner, M et al, 2019, Maingot's Abdominal Operations, 13th ed
32.
• Resuscitation
• IVantibiotics
• Appendicectomy - urgent vs emergency
• Open appendicectomy
• Laparoscopic appendicectomy
• NOTES - Natural Orifice Transluminal Endoscopic Surgery
• Incidental appendicectomy
Appendicitis - management
33.
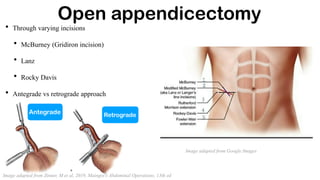
• Through varyingincisions
• McBurney (Gridiron incision)
• Lanz
• Rocky Davis
• Antegrade vs retrograde approach
Open appendicectomy
Image adapted from Zinner, M et al, 2019, Maingot's Abdominal Operations, 13th ed
Antegrade Retrograde
Image adapted from Google Images
34.
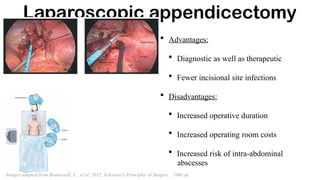
Laparoscopic appendicectomy
• Advantages:
•Diagnostic as well as therapeutic
• Fewer incisional site infections
• Disadvantages:
• Increased operative duration
• Increased operating room costs
• Increased risk of intra-abdominal
abscesses
Images adapted from Brunicardi, C , et al, 2015, Schwartz's Principles of Surgery, 10th ed
35.
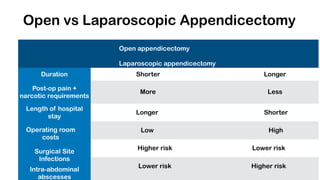
Open vs LaparoscopicAppendicectomy
Open appendicectomy
Laparoscopic appendicectomy
Duration
Post-op pain +
narcotic requirements
Length of hospital
stay
Operating room
costs
Surgical Site
Infections
Intra-abdominal
abscesses
Shorter Longer
More Less
Longer Shorter
Low High
Higher risk Lower risk
Lower risk Higher risk
36.
• Performed toprevent one from developing appendicitis
• Indicated for some special populations;
• Children about to begin chemotherapy
• Disabled who cannot describe symptoms / react normally to abdominal pain
• Patients with Crohn’s disease with normal caecum
• Individuals going to travel to remote places where there in no access to medical or
surgical care
• During Ladd’s procedure for malrotations / other abdominal procedures
Neither clinically nor economically appropriate
Incidental appendicectomy
37.
NOTES appendicectomy
• Accessto appendix is via naturally existing external orifice
• Most common routes;
• Trans-vaginally
• Trans-gastrically
• Advantages: Reduction of post-op wound pain; no abdominal scar; shorter
convalescence; avoidance of wound infection
• Disadvantages: Complications associated with closure of enterotomy
38.
What is chronicappendicitis?
• Incidence : 1.5 % of all appendicitis cases
• Inflammation persists > 3 weeks
• Usually females; patients managed non-operatively
Criteria;
• No alternative diagnosis
• Pathologic evidence of chronic inflammation / fibrosis
• Complete relief of symptoms after appendicectomy
39.
What is recurrentappendicitis?
• Incidence: 10%
Causes;
• Partial luminal obstruction
• Missed diagnosis
• Atypical presentation
• Prior treatment with antibiotics
• Management: Appendicectomy
Appendicular carcinoid
• Mostcommon site of carcinoid tumor (2nd -
small bowel, 3rd - rectum)
• Most commonly found at tip of appendix
• Do not usually have carcinoid features until
metastases are widespread
• Macroscopic appearance: firm, yellow,
bulbar mass
• Average size: 2.5 cm
• Management depends on size and location of
carcinoid
Feature of carcinoid Management tenet
< 1cm
1 - 2 cm
> 2cm
Appendicectomy
Depends on location,
presence of
mesenteric spread,
lymphatic invasion
Right hemicolectomy
Image adapted from COSECSA module
43.
Appendicular adenocarcinoma
• 3types;
• Mucinous type
• Colonic type
• Signet-ring type
• Worst prognosis = signet-ring type
• Symptoms - similar to acute appendicitis
• Clinical features: ascites + palpable RIF mass
• Management - right hemicolectomy
• Survival: 55% overall but varies by stage, grade and histological type
44.
Appendicular mucocele
• Obstructivedilatation of intraluminal
accumulation of mucoid material.
Management options
- Appendicectomy - if unruptured
• Processes by which mucoceles form;
- Right hemicolectomy /
ileocecectomy
• Retention cysts
• Mucosal hyperplasia
• Cystadenoma
• Cystadenocarcinomas
Appendicular lymphoma
• Extra-nodalsite for non-Hodgkin’s lymphoma
• Primary lymphoma of appendix = 1-3% of GI lymphomas
• Diagnosis = CT abdominal scan - tumor >= 2.5 cm + soft tissue thickening
• Management - depends on location of tumor
• Tumor confined to appendix - appendicectomy
• Tumor extending to caecum / mesentery - right hemicolectomy = adjuvant
therapy
47.
Take Home Message
•Mainstay of management of appendicitis is APPENDICECTOMY
• Remember OCHSNER SCHERREN management for patients with RIF
mass
• Scoring systems and further imaging aid in reducing negative
appendicectomy rates
48.
References
1. Zinner, Met al, 2019, Maingot's Abdominal Operations, 13th ed, pp. 1814 -64
2. Brunicardi, C , et al, 2015, Schwartz's Principles of Surgery, 10th ed, pp 1240 -59
3. The Appendix - COSECSA module
4. AG Marion, et al, 2018, The Use of Alvarado Score In Diagnosis of Acute
Appendicitis at Jinja Regional Referral Hospital,
5. Alvarado, A, 1986, A Practical Score For Early Diagnosis of Acute Appendicitis,
Annals of Emergency Medicine, 15(5), pp 557 -64
49.
6. Bharath, Bet al, 2020, A Comparative Study of Tzanakis Score Versus Alvarado Score in Acute Appendicitis t
a Rural Hospital, Journal of Evidence Based Medicine and Health, pISSN -2349-2562, eISSN 2349 - 2570,vol
7, (35) DOI: 10.8410/jebmh/2020/384
7. Mattei, P et al, 1994, Chronic and Recurrent Appendicitis are Uncommon Entities Often Misdiagnosed, Journal
of American College of Surgeons, 178 (4); pp 385-9
8. Samuel, M, 2002, Pediatric Appendicitis Score, Journal of Paediatric Surgery, Vol 37, No 6, pp 887 - 881
9. Tzanakis, NE et al, 2005, A New Approach to Accurate Diagnosis of Acute Appendicitis, World Journal
of Surgery; 29(9), pp 1151 - 1156
10.Ubaidi, B A, et al, 2016, Missed Appendicitis in Primary Care: Lessons Learned, Journal of Cardiology &
Current Research, DOI: 10.15406/jccr.2016.07.00256
11. Von-Muhlen, B, et al, 2015, AIR Score Assessment for Acute Appendicitis, Arq Bras Cir Dig, 28(3); pp 171-3,
doi: 10.1590/s0102-67202015000300006
12.Nanjundaiah, N et al, 2014, A Comparative Study of RIPASA Score and Alvarado score in Diagnosis of Acute
Appendicitis, Jounral of Clinical and diagnostic Research, 8 (11), doi: 10.7860/JCDR/2014/9055.5170
References - cont.



![Alvarado score [5]
• Score < 3: Low likelihood of
appendicitis
• Score : 4 - 6: consider
further imaging
• Score >=7 : High likelihood of
appendicitis
• Inconsistent in children and
women
• Sensitivity for ruling out > ruling in
Component Maximum score
Migration of pain to right
lower quadrant
Anorexia
Nausea / Vomiting
Fever > 37.3 C
Right iliac fossa tenderness
Rebound tenderness
Leucocytosis > 10 x 10
^9 Left shift of neutrophils
MAXIMUM TOTAL
1
1
1
1
2
1
2
1
10](https://image.slidesharecdn.com/appendixpresentation-250708080442-23131049/85/Appendix-power-point-presentation-pptx-24-320.jpg)
![Tzanakis score [9]
• Circa 2005
• Score > 8 = diagnostic of
acute appendicitis
• Sensitivity:95.4%
• Specificity: 97.4%
Parameter Score
Presence of right
lower abdominal 4
tenderness
Rebound tenderness 3
Laboratory findings:
WBC > 12,000
2
Ultrasound finding:
Indicative of 6
appendicitis
Total 15](https://image.slidesharecdn.com/appendixpresentation-250708080442-23131049/85/Appendix-power-point-presentation-pptx-25-320.jpg)
![Appendicitis Inflammatory
Response Score (AIRS) [11]
• 0 - 4: Low probability - OPD
follow-up
• 5 - 8: Indeterminate - Active
observation / Diagnostic
laparoscopy
• 9-12: High probability - Surgical
exploration
Findings Score
Vomiting 1
Right inferior fossa pain 1
Rebound tenderness /
muscular defence
Light : 1
Medium : 2
Strong : 3
Body temp >= 38.5 C 1
Polymorphonuclear
leucocytes
70% - 84% :1
>= 85% : 2
White Blood Cell count
10.0 - 14.9 x 10^9 : 1
>=15 x 10^9 :
2
C-reactive protein
concentration
10 - 49 : 1
>=50 : 2
MAXIMUM TOTAL 12](https://image.slidesharecdn.com/appendixpresentation-250708080442-23131049/85/Appendix-power-point-presentation-pptx-26-320.jpg)
![RIPASA Score
[12]
• Includes; age, gender, duration of symptoms
prior to presentation.
• Circa 2014
• More accurate among Asian population
• Sensitivity = 96.7%
• Specificity = 93%
• Diagnostic accuracy = 95.1 %
• Score > 7.5 - significant for appendicitis](https://image.slidesharecdn.com/appendixpresentation-250708080442-23131049/85/Appendix-power-point-presentation-pptx-27-320.jpg)