Downloaded 93 times
![Emergency Equipment for Sedation
[American Society of Anesthesiologists - 2002; 96:1004–17]
• Intravenous equipment
• Basic airway management equipment
• Source of compressed oxygen (tank with regulator or pipeline supply with flowmeter)
• Source of suction
• Suction catheters [pediatric suction catheters]
• Yankauer-type suction
• Face masks [infant/child]
• Self-inflating breathing bag-valve set [pediatric]
• Oral and nasal airways [infant/child-sized]
• Lubricant](https://image.slidesharecdn.com/anaesthesiaforcathlabprocedures-180117153033/85/role-of-anesthesiologist-in-cathlab-9-320.jpg)
![Emergency Equipment for Sedation
[American Society of Anesthesiologists - 2002; 96:1004–17]
• Advanced airway management
equipment
• Laryngeal mask airways [pediatric]
• Laryngoscope handles (tested)
• Laryngoscope blades [pediatric]
• Endotracheal tubes
• Cuffed 6.0, 7.0, 8.0 mm ID
• [Uncuffed 2.5, 3.0, 3.5, 4.0, 4.5, 5.0, 5.5,
6.0 mm ID]
• Stylet (appropriately sized for endotracheal
tubes)
• Pharmacologic Antagonists
• Naloxone
• Flumazenil
• Emergency medications
• Epinephrine
• Ephedrine
• Vasopressin
• Atropine
• Nitroglycerin (tablets or spray)
• Amiodarone
• Lidocaine
• Glucose, 50% [10 or 25%]
• Diphenhydramine
• Hydrocortisone, methylprednisolone, or
dexamethasone
• Diazepam or midazolam](https://image.slidesharecdn.com/anaesthesiaforcathlabprocedures-180117153033/85/role-of-anesthesiologist-in-cathlab-10-320.jpg)

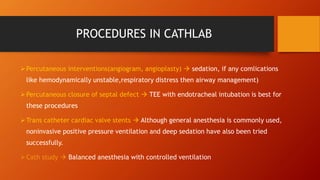
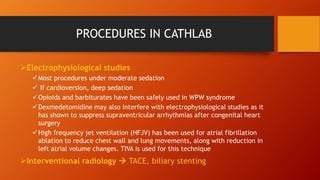


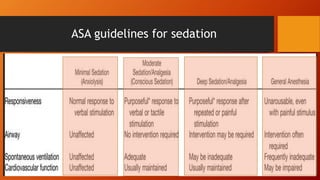
This document discusses the role of anesthesiologists during cath lab procedures and the types of anesthesia used. It outlines the necessary equipment, medications, monitoring, and considerations for different procedures. Anesthesiologists must plan carefully with cardiologists and be prepared to manage airways and treat potential complications while patients are sedated or anesthetized for cath lab exams and interventions.































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)



