Definition
• Amputation
- procedureof removal of limb or part of the
limb through a bone or multiple bones.
• Disarticulation
- removal of whole limb or part of the limb
through a joint.
3.
• Requires whenthe vitality of the part is
destroyed by injury or disease or when the life
of the patient is threatened by infective,
ischemic or malignant pathology.
• Also indicated for deformed or paralysed limb
that is of little functional use to patient,
particularly in instances where a prosthetic limb
would be of greater value.
4.
Common causes:
• Trauma:
-road traffic accidents, industrial accidents etc. are common
causes.
-when there is extensive loss of tissue and disruption of blood
supply, amputation is performed.
• Peripheral vascular insufficiency : Irreversible loss of vascularity
due to diseases like
-Berger’s disease,
-atherosclerosis,
-embolism,
-arterial thrombosis,
- trauma are indications for amputation.
5.
1) Malignant tumours: Amputation is considered for
extensive malignancy. This is done to prevent recurrence.
2) Nerve injuries & infections :
-Anaesthetic limb often develops ulceration, infection
& severe tissue damage.
-When ulceration & infection persists, and fail to
respond to the medical treatment, amputation is performed.
-Some infections like gas gangrene, chronic infections
like osteomyelitis etc. may also need amputation.
6.
• 3) Congenitalanomalies :
-accessory thumb,
-congenital absence of bones etc. requires amputation.
• 4) Extreme heat or cold :
-Injuries following electrical burns, accidental burns as
well as exposure of the limb to extreme cold conditions may
need amputation.
-Thermal injuries may sometimes lead to extensive tissue
destruction & deformities.
-Prolonged exposure of the limb to extreme cold conditions
results in blockage of blood circulation leading to gangrene.
7.
Levels of amputation
•In a limb an amputation is carried out at a level which
will give the stump an optimum length to facilitate
subsequent prosthetic fitting.
• The level of amputation is determined by the viability
of the tissues.
• It is ,however, important that the stump should be
well healed and non tender.
• A joint must always be preserved whenever possible.
8.
Technical Aspects
Skin andmuscle Flaps:
1. Keep flaps thick
2. Avoid unnecessary dissection
3. Scar should not be in contact with bone
4. Divide muscle at least 5cm distal to
bone
5. Myodesis: suturing muscle/tendon to
bone
9.
Technical Aspects
Haemostasis
1. Usetourniquet unless ischaemic limb
2. Elevate limb before applying tourniquet
3. Major blood vessels individually ligated
10.
Technical Aspects
Nerves
• Neuromaforms after nerve divided and
becomes painful if subjected to repeated
trauma
• Pull nerve gently and cut cleanly with a
sharp knife so that it retracts
• Ligate large nerves to prevent bleeding
11.
Technical Aspects
Bone
• Avoidexcessive periosteal stripping
• Bony prominences should be padded by
soft tissue
• Rasp bony end to form a smooth contour
12.
Upper extremity amputations
•Finger and hand
• Transcarpal
• Disarticulation of wrist
• Forearm
• Transhumeral
• Disarticulation of shoulder
• Forequarter
13.
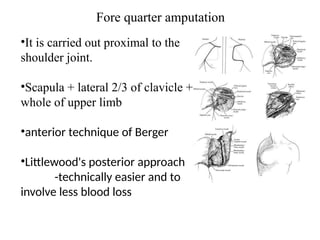
Fore quarter amputation
•Itis carried out proximal to the
shoulder joint.
•Scapula + lateral 2/3 of clavicle +
whole of upper limb
•anterior technique of Berger
•Littlewood's posterior approach
-technically easier and to
involve less blood loss
14.
Shoulder disarticulation
•Amputation throughthe humeral neck preserves
the normal contours of the shoulder and is
preferable to the more proximal amputations unless
they are specifically indicated.
•Amputations through the glenohumeral and
scapulothoracic articulations are uncommon.
•Tumor control remains the primary indication for
amputation at this level despite efforts at limb
salvage made possible by more accurate methods
of preoperative localization, modern adjuvant
therapy, and advances in tissue banking
15.
Above elbow amputation
•Itis an Amputation through the Arm.
•A 20 cm long stump as measured from
the tip of acromion is ideal.
•The vast majority of amputations
through the humerus or elbow joint
result from trauma.
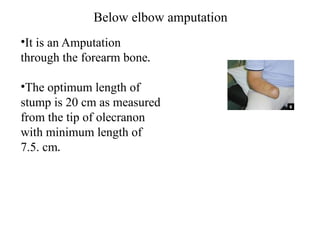
Below elbow amputation
•Itis an Amputation
through the forearm bone.
•The optimum length of
stump is 20 cm as measured
from the tip of olecranon
with minimum length of
7.5. cm.
18.
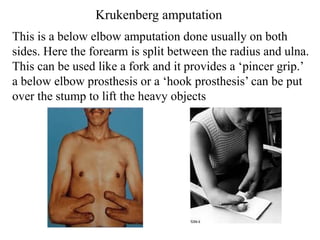
Krukenberg amputation
This isa below elbow amputation done usually on both
sides. Here the forearm is split between the radius and ulna.
This can be used like a fork and it provides a ‘pincer grip.’
a below elbow prosthesis or a ‘hook prosthesis’ can be put
over the stump to lift the heavy objects
19.
Wrist disarticulation
•It isan Amputation through the radio-carpal joint.
•Palmar and dorsal flaps in a 2:1 ratio are developed to
provide adequate tissue for closure
•The styloid processes need to be contoured enough to
create a symmetrical limb for fitting of the prosthesis.
•The main vessel groups that must be identified are the
ulnar, radial, anterior and posterior interossei.
20.
• The nervesthat must be identified are the
median, ulnar, posterior interosseous, and
radial sensory.
• Specifically, the transected end of the radial
sensory nerve should lie beneath the
brachioradialis muscle belly in order to protect
its neuroma from mechanical trauma during
prosthesis use.
21.
• Amputation offingers is most commonly
undertaken for severe trauma in which there
is skin loss combined with additional bone,
vessel or tendon damage.
• Every effort must be made to preserve as
much of the thumb as circumstances will
allow, as it is of pre-eminent importance in the
hand.
22.
• In general,amputation through the base of a
phalanx is preferable to disarticulation at the
joint immediately proximal, as this preserves
the attachments of tendons and intrinsic
muscles and results in a stronger grip.
23.
TYPES OF LOWERLIMB AMPUTATIONS
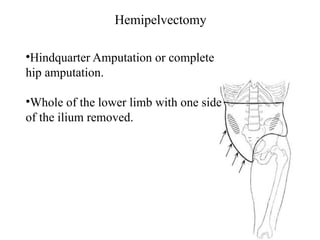
• Hemipelvictomy
• Hip disarticulation
• Trans femoral amputation
• Knee disarticulation
• Transtibial amputation
• Foot amputation
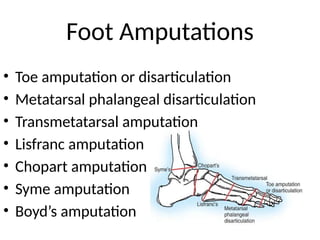
Hindfoot and ankleamputations
• Syme
- at the distal tibia and fibula 0.6 cm
proximal to the periphery of ankle joint
and passing through the dome of the
ankle centrally
26.
• Modified Syme’sAmputations( sarmiento)
-transection of the tibia and fibula approx.
1.3cm proximal to the ankle joint and excision
of the medial and lateral malleoli
Amputations of lowerextremity
• 85% of all amputations
• 85% of these due to peripheral vascular
disease and diabetes
1. Transtibial – below knee
2. Disarticulation of knee
3. Transfemoral – above knee
Disarticulation of knee
Endbearing stump
• End bearing surface of femur is preserved
• Long lever arm controlled by strong muscles is
created
• Prosthetic knee mechanisms available
• Ideal for non ambulating patients because
there is adequate length for sitting support
and balance. Knee flexion contractures and
distal ulcers are avoided
31.
Transfemoral
• 2nd
in frequencyafter transtibial
• As knee joint is lost, important for the
stump to be as long as possible to
provide a strong lever arm for control of
the prosthesis
• Section of the femur should be at least
10 cm from the knee to allow room for
the prosthetic knee joint
32.
Other lower limbamputations
• Disarticulation of hip
• Hemipelvectomy
complications
1) Hematomas :This delays the wound healing and acts as a
culture media for the growth of the organisms
2) Infections : This is more common in peripheral vascular
disease and diabetics.
3) Necrosis of the skin flaps are usually due to insufficient
circulation and require revision amputation.
36.
4) Contractures :This is largely preventable by positioning
the stump properly. Flexion contractures of hip and knee
are very common.
5) Neuromas form always at the end of a cutaneous nerve
and any pain from a neuroma is usually caused by
traction on a nerve when it is embedded within the scar
tissue.
6) Abnormality of residual limb : dog ear appearance
37.
•7) Phantom sensation: This is a pseudo feeling of the
presence of the amputated limb. It could be of a painless or a
painful variety. The reasons why someone will still perceive
the amputed body part are as follows :
• Firstly, the nerves have been severed, causing injury to
nerve tissue, and thus pain messages are sent to the brain.
• Secondly, the brain has an area of tissue dedicated to that
part & will expect sensory information. This area of brain is
not removed during limb amputation & still tries to process
information which is perceived as pain.









































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)






