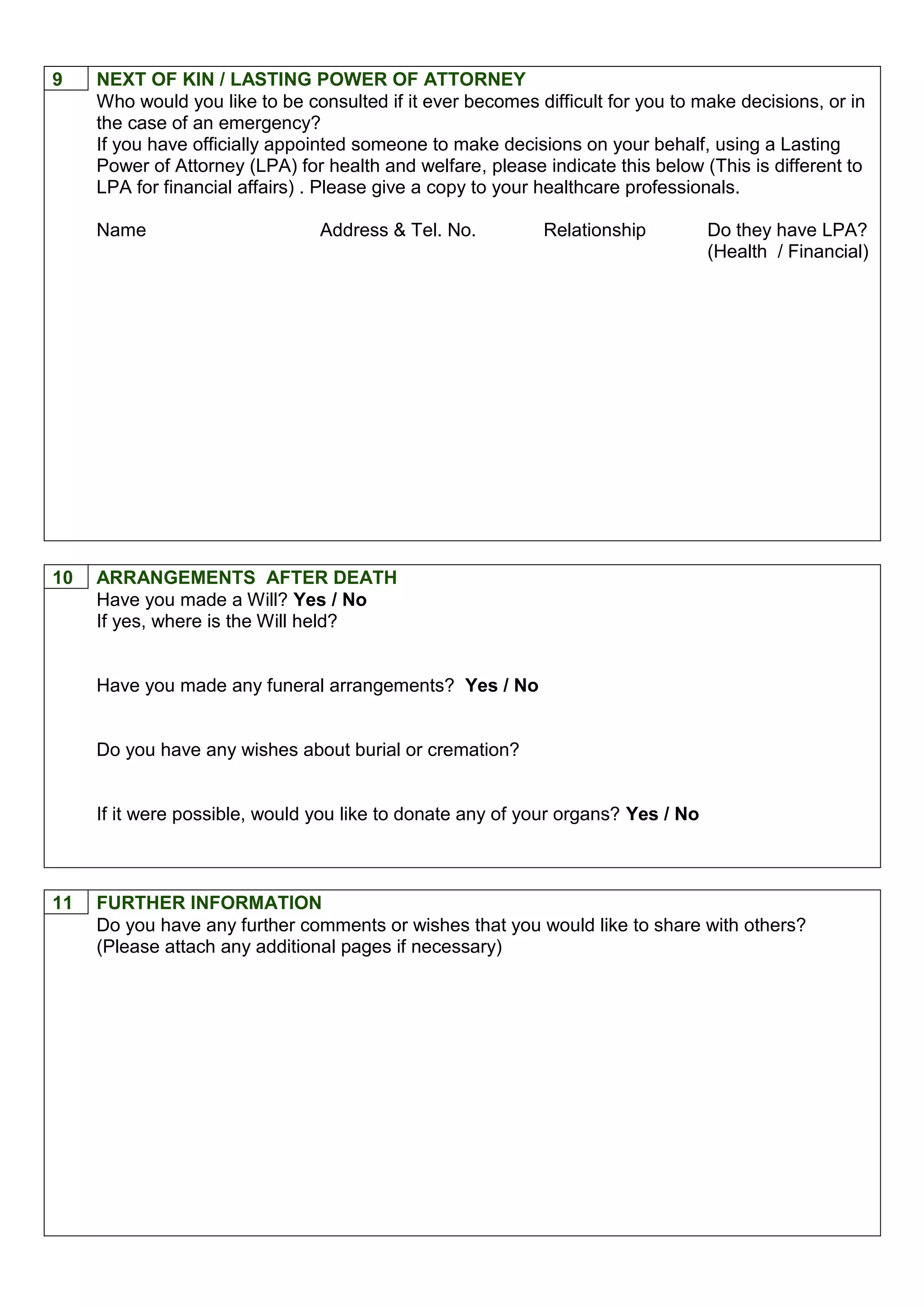
This document is a care plan for an individual to outline their wishes and preferences for future health care. It allows the person to think ahead and provide guidance to medical professionals and family on topics like preferred place of care, end of life wishes, spiritual beliefs, and funeral arrangements. The plan emphasizes that an individual's wishes may change over time and can be updated. It also provides space for medical history, contact information for family, and signatures to document discussions.