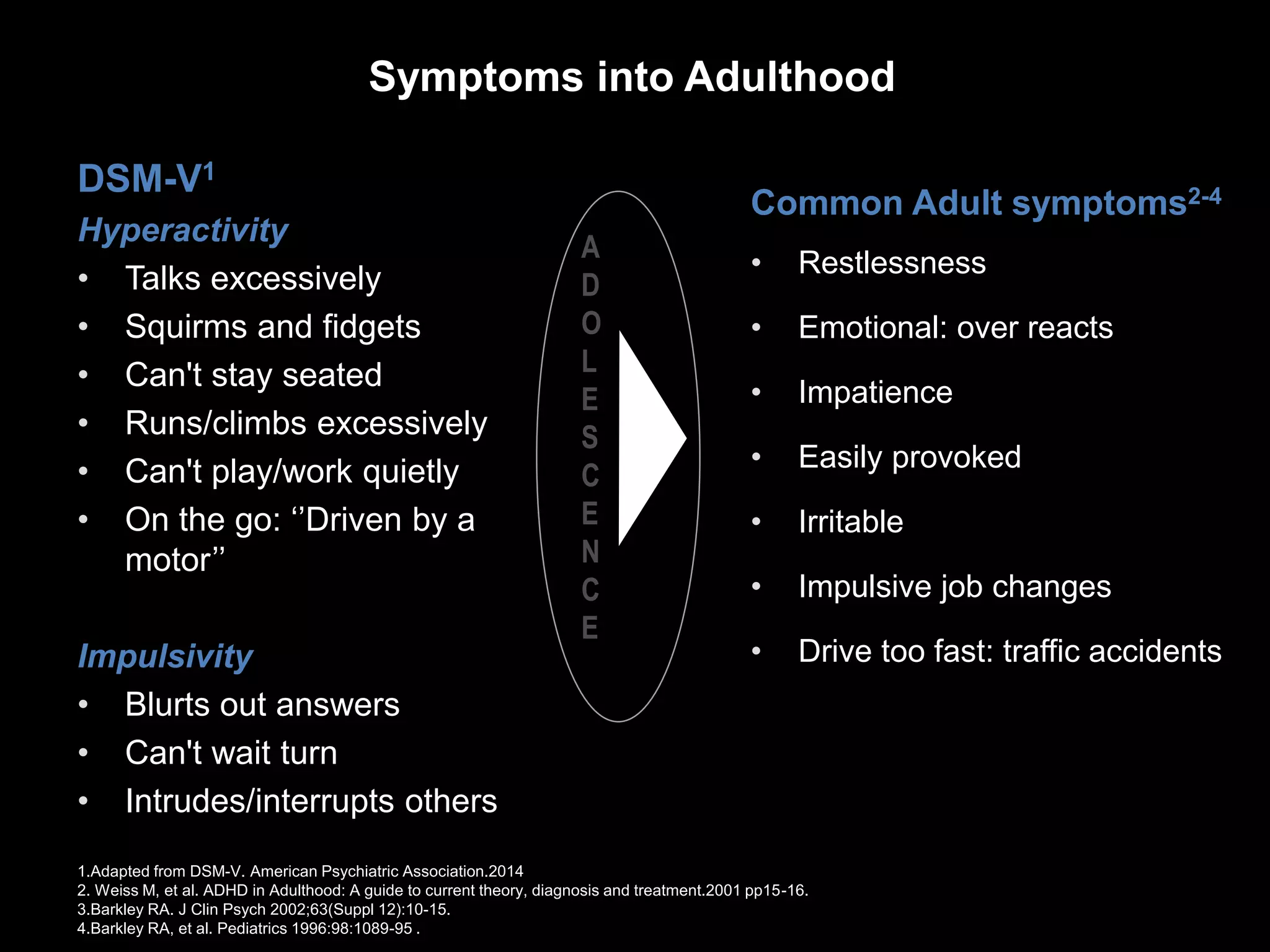
The document discusses ADHD in adolescents, highlighting its symptoms, prevalence rates, and long-term consequences such as academic difficulties, emotional challenges, and increased risk of antisocial behavior and substance abuse. It emphasizes the importance of organized treatment protocols and effective transition services to improve outcomes for those affected. The current service landscape reveals significant gaps, particularly in transitioning from child to adult care, which needs addressing to meet the needs of patients and families.