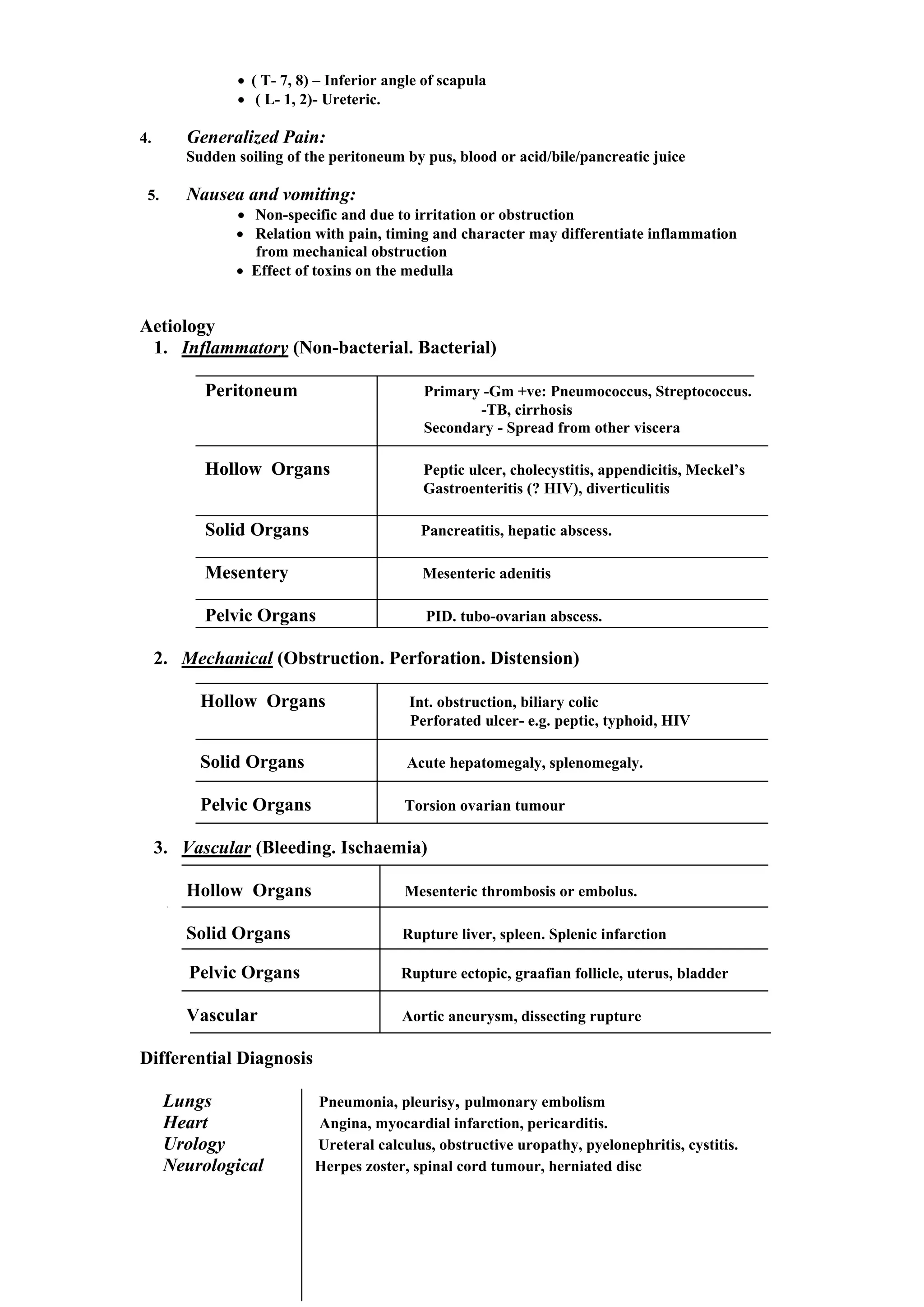
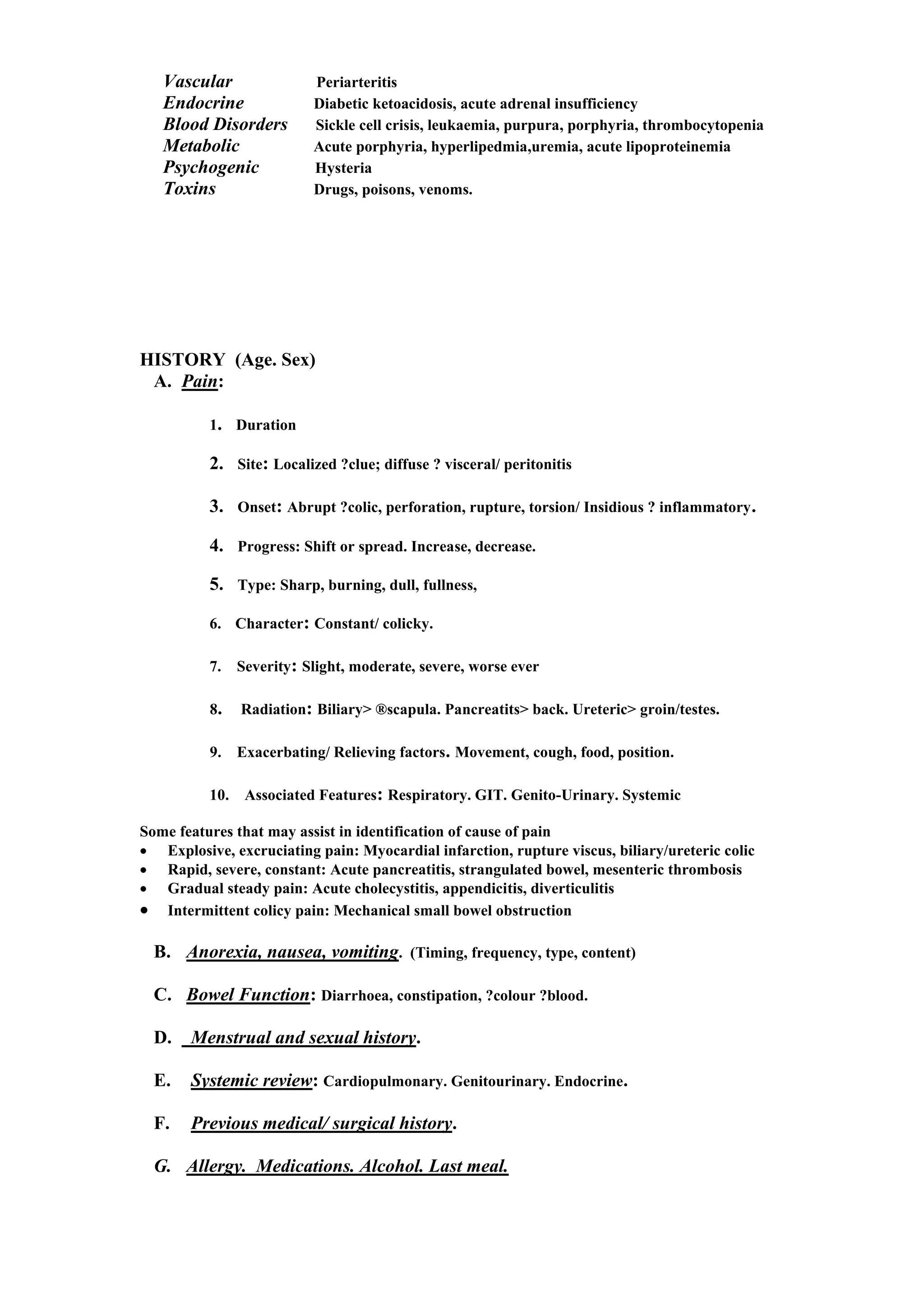
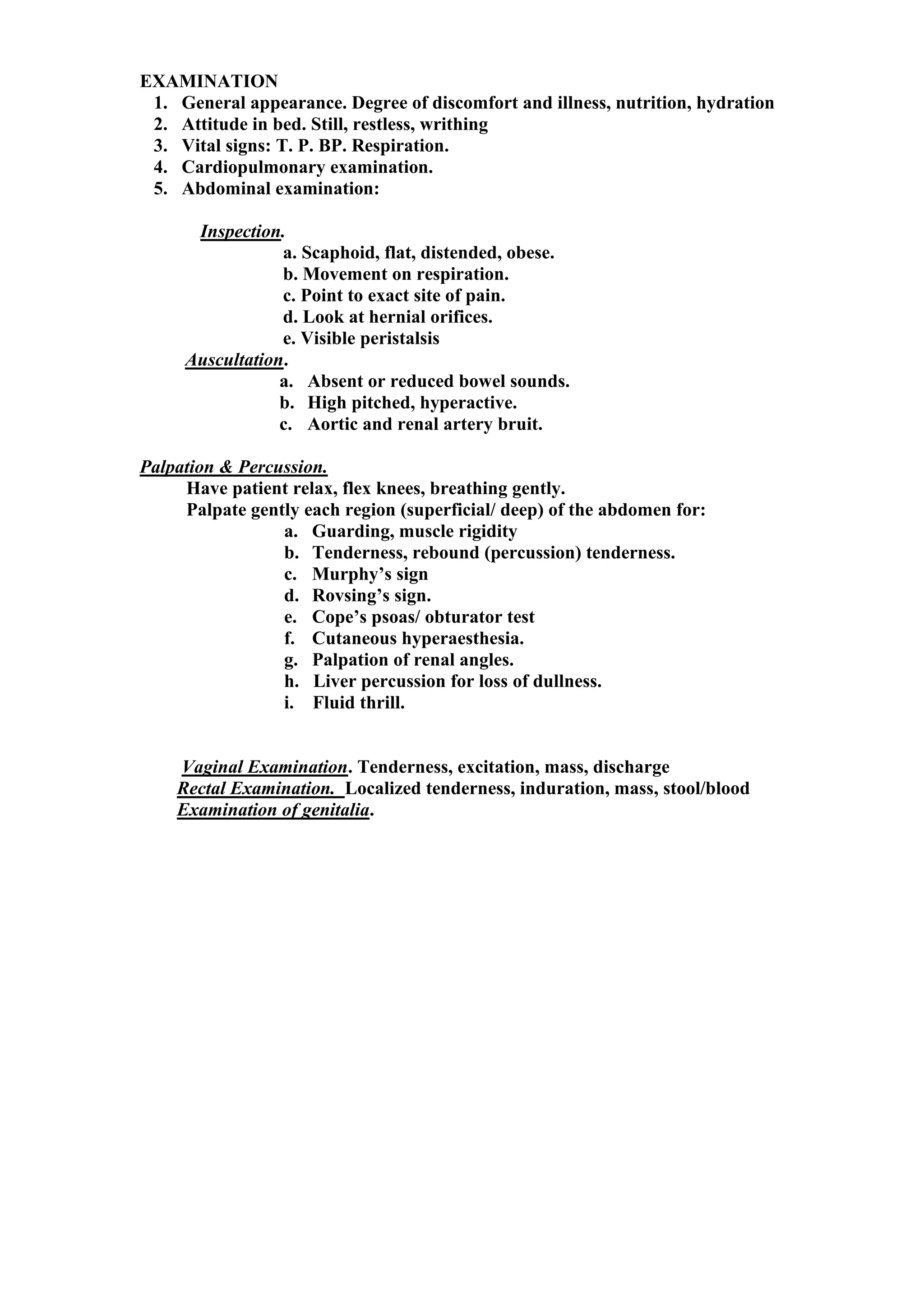
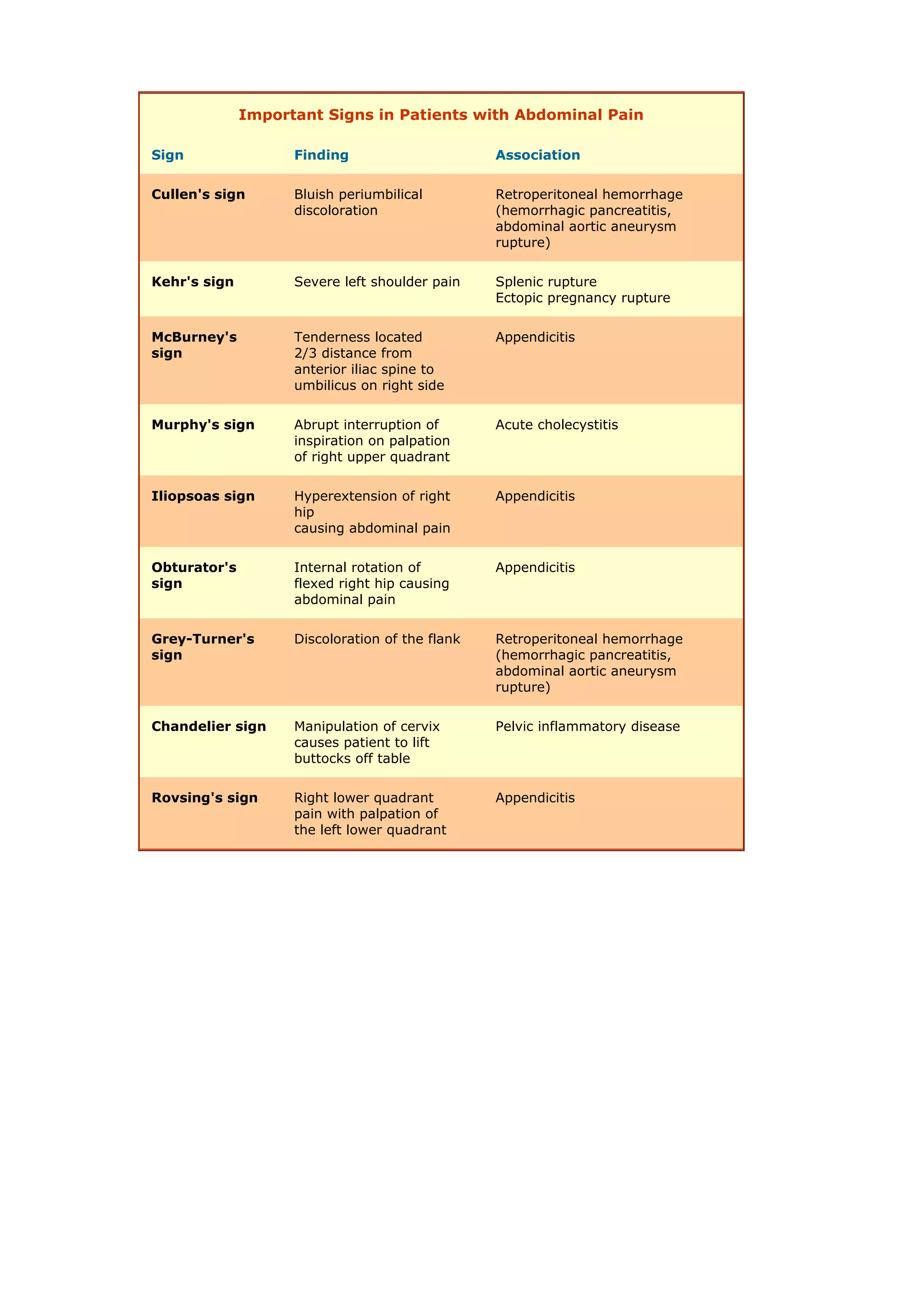
The document outlines the definition, diagnosis, and management of acute abdomen, characterized by rapid onset abdominal pain and associated symptoms like nausea and vomiting. It categorizes abdominal pain into visceral, parietal, referred, generalized, and discusses various causes including inflammatory, mechanical, and vascular origins. It also highlights the importance of thorough history taking, physical examination, and investigations to guide treatment, which may include surgery, observation, or conservative management.

![ACUTE ABDOMEN
Definition: Rapid onset of ABDOMINAL PAIN (in a patient previously well)
+/- NAUSEA and VOMITING.
“Acute abdomen” => Early diagnosis => Management
Types of Abdominal Pain ( thru sympathetic [splanchnic ] nerves)
1. Visceral Pain:
• Caused by stimulation of visceral afferents on distension, contraction,
ischaemia, chemical irritation
• Usually colicky and relieved by pressure.
• Diffuse, poorly localized, and difficult to describe.
• May be referred to a distant region.
• Midline:
Structure Nerves/ Sensory level Site
Foregut Coeliac ( T6-8) Epigastrium
Midgut Sup. Mesenteric ( T10-11) Umbilical
Hindgut Inf. Mesenteric (T11-L1) Hypogastrium
• May be associated with nausea, vomiting and reflex hypotension
2. Parietal Pain:
• Irritation of parietal peritoneum by blood, inflammatory exudates, content of
hollow viscus e.g. bile, acid, pancreatic juice
• Constant, sharp and localized to site of irritation.
• Aggravated by pressure and movement.
• Associated with reflex rigidity, reduced bowel activity.
3. Referred Pain:
Pain of visceral disease referred to a superficial area of body
derived from the same segment of cord as the viscus
• ( C- 3, 4, 5) - Diaphragm](https://image.slidesharecdn.com/acuteabdomen-221121164128-9bb83939/75/Acute-Abdomen-pdf-2-2048.jpg)