Downloaded 33 times


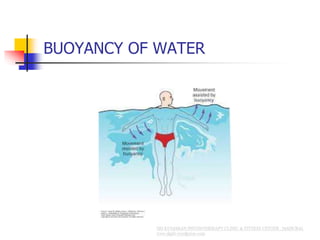


Active movement refers to voluntary movement performed with one's own strength or energy. Assisted exercise involves applying an external force to help compensate for muscle deficiencies and ensure maximum effort from the weakened muscles. The principles of assisted exercise include applying assistance in the direction of muscle action, starting from a position of minimal tension in antagonistic muscles, and decreasing assistance as muscle power increases. The goal is for the patient to achieve controlled active movement without assistance over time through strengthening and retraining coordination.



































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


















