MỤC TIÊU HỌCTẬP
1. Nêu được phân loại và cơ chế tác dụng chính của retinoids hệ thống.
2. Nêu được các chỉ định chính của retinoid hệ thống.
3. Nêu được các tác dụng phụ chính của retinoids và một số biện pháp để
phòng tránh các tác dụng phụ thường gặp đó.
4.
Nội dung trìnhbày
Phần 1
Phân loại
Phần 2
Chỉ định
Phần 3
Liều lượng
Phần 4
Tác dụng phụ
PHÂN LOẠI
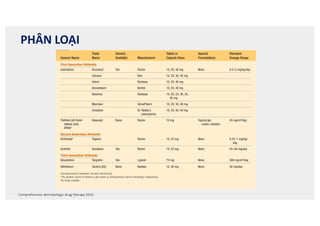
Comprehensive dermatologicdrug therapy 2020
Systemic Retinoids
Generic Name
Trade
Name
Generic
Available Manufacturer
Tablet or
Capsule Sizes
Special
Formulations
Standard
Dosage Range
First-Generation Retinoids
Isotretinoin Accutanea Yes Roche 10, 20, 40 mg None 0.5–2 mg/kg/day
Claravis Barr 10, 20, 30, 40 mg
Sotret Ranbaxy 10, 20, 40 mg
Amnesteem Bertek 10, 20, 40 mg
Absorica Ranbaxy 10, 20, 25, 30, 35,
40 mg
Myorisan VersaPharm 10, 20, 30, 40 mg
Zenatane Dr. Reddy’s
Laboratories
10, 20, 30, 40 mg
Tretinoin (all-trans-
retinoic acid,
ATRA)b
Vesanoid None Roche 10 mg Topical gel,
cream, solution
45 mg/m2/day
Second-Generation Retinoids
Etretinatec Tegison Roche 10, 25 mg None 0.25–1 mg/kg/
day
Acitretin Soriatane Yes Roche 10, 25 mg None 25–50 mg/day
Third-Generation Retinoids
Bexarotene Targretin Yes Ligand 75 mg None 300 mg/m2/day
Alitretinoin Toctino (EU) None Basilea 10, 30 mg None 30 mg/day
aAccutane brand of isotretinoin has been discontinued.
bThis systemic version of tretinoin is also known as ATRA (primarily used for hematologic malignancies).
cNo longer available.
TABLE
22.1
Isotretinoin, first synthesized in 1955, had been studied in
Europe since 1971 (Table 22.1). Initially studied for disorders
of keratinization,3 isotretinoin was subsequently studied for acne
vulgaris and was noted to dramatically improve acne in patients
with severe disease, as well as to induce prolonged remissions. In
the late 1970s isotretinoin was confirmed to be highly effective
on the mechanisms of action of the second-generation retinoids is
derived from etretinate data.
Systemic bexarotene was approved for the cutaneous manifes-
tations of certain cases of cutaneous T-cell lymphoma (CTCL) in
1999. The approval of a topical formulation of bexarotene fol-
lowed soon after.5
7.
CƠ CHẾ TÁCDỤNG
stero
some
recep
enco
wher
126.2
RA
act a
a var
horm
cross
retin
and
seque
prom
ded r
How
tiona
of co
the c
tiona
the t
the d
mech
In
of re
effect
genes
retin
such
IL6)
there
genes
inflam
retin
retinoic acid form, and only a very small fraction is isomerized into
13-cis-RA. at-RA is the primary active ligand that binds to the three
known nuclear RARs, which mediate, at least in part, the molecular
and cellular effects of retinoic acid.
Retinoid Receptors
Retinoids exert most of their physiologic effects on DNA transcription
by binding to two distinct families of nuclear receptors, RARs and
RXRs. These receptor families belong to a superfamily of nuclear recep-
Fig. 126.1 Chemistry of retinoids.
Adapalene
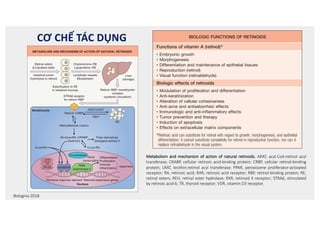
Table 126.1 Biologic functions of retinoids.
BIOLOGIC FUNCTIONS OF RETINOIDS
Functions of vitamin A (retinol)*
• Embryonic growth
• Morphogenesis
• Differentiation and maintenance of epithelial tissues
• Reproduction (retinol)
• Visual function (retinaldehyde)
Biologic effects of retinoids
• Modulation of proliferation and differentiation
• Anti-keratinization
• Alteration of cellular cohesiveness
• Anti-acne and antiseborrheic effects
• Immunologic and anti-inflammatory effects
• Tumor prevention and therapy
• Induction of apoptosis
• Effects on extracellular matrix components
*Retinoic acid can substitute for retinol with regard to growth, morphogenesis, and epithelial
differentiation; it cannot substitute completely for retinol in reproductive function, nor can it
replace retinaldehyde in the visual system.
S E C T I O N
19
MEDICAL
THERAPY
oxidative stress can also lead to lowered retinoid levels in the skin9
.
There has been an ongoing debate regarding possible generation of
reactive oxygen species upon the interaction of UVA radiation with
retinyl esters (e.g. retinyl palmitate) present in cosmetics and sun-
screens, but the theoretical potential for photocarcinogenicity has not
been shown to be clinically relevant.
Synthetic Retinoids
Three generations of synthetic retinoids have been developed (see Fig.
126.1). The first-generation non-aromatic retinoids (tretinoin, isotreti-
noin, alitretinoin) are produced by chemically modifying the polar end
group and the polyene side chain of vitamin A. Second-generation
mono-aromatic retinoids (etretinate, acitretin) are formed by replacing
the cyclic moiety of vitamin A with different substituted and unsubsti-
tuted ring systems. The third-generation poly-aromatic retinoids (ada-
palene, bexarotene, tazarotene), called arotinoids, are produced by
cyclization of the polyene side chain.
Commercially available retinoids differ not only in their spectrum of
clinical efficacy but also in their observed toxicity and pharmacokinet-
ics. Each retinoid should be investigated as a unique drug, and the lack
of disease response to one retinoid does not necessarily signify unre-
sponsiveness to other retinoids.
The oral bioavailability of all retinoids is considerably enhanced
when administrated with food, especially with a fatty meal, due to their
lipophilic properties. Retinoid metabolism is predominantly hepatic; it
involves oxidation and chain shortening to biologically inactive and
polar metabolites, facilitating biliary and/or renal elimination. The
oxidative metabolism is induced by the retinoids themselves and pos-
sibly also by other agents known to stimulate hepatic cytochrome P450
isoforms. Table 126.2 summarizes the key pharmacologic features and
nuclear binding profiles of retinoids used in dermatology.
Adapalene
Adapalene is a photostable, rigid, and highly lipophilic synthetic reti-
noid with higher affinity for RAR-β/γ than for RAR-α. Since RAR-β is
not expressed in keratinocytes, RAR-γ is the primary target receptor for
adapalene in the epidermis. Adapalene does not bind to cellular retinoic
acid-binding proteins (CRABPs) but does induce expression of CRABP-II.
Its lipophilic properties may contribute to better pilosebaceous uptake
and anti-acne activity. Given its negligible transdermal absorption, the
teratogenic risks of topical adapalene appear to be minimal. While
adapalene affects the cellular differentiation, keratinization, and inflam-
matory processes that are abnormal in acne, it has no sebostatic effect.
Fig. 126.2 Metabolism and mechanism of action of natural retinoids. ARAT,
acyl-CoA:retinol acyl transferase; CRABP, cellular retinoic acid-binding protein;
CRBP, cellular retinol-binding protein; LRAT, lecithin:retinol acyl transferase;
PPAR, peroxisome proliferator-activated receptor; RA, retinoic acid; RAR,
retinoic acid receptor; RBP, retinol-binding protein; RE, retinyl esters; REH,
retinyl ester hydrolase; RXR, retinoid X receptor; STRA6, stimulated by retinoic
acid 6; TR, thyroid receptor; VDR, vitamin D3 receptor.
METABOLISM AND MECHANISM OF ACTION OF NATURAL RETINOIDS
Liver
(storage)
Retinol−RBP−transthyretin
complex
(systemic circulation)
STRA6 receptor
for retinol−RBP
Retinol−CRBP
ARAT/LRAT
REH
Retinaldehyde (vision)
All-trans-RA−CRABP
(tretinoin)
Polar derivatives
(biological activity?)
13-cis-RA
RE
Keratinocyte
9-cis-RA
Gene
transcription
Lymphatic vessels
Bloodstream
Intestinal lumen
(hydrolysis to retinol)
Chylomicrons−RE
Lipoproteins−RE
Esterification to RE
in intestinal mucosa
Retinyl esters
β-Carotene (diet)
Co-activators
Nucleus
Differentiation
Proliferation
Immune
Inflammatory
responses
RXR
RAR
Hormone response element Retinoid-responsive genes
PPAR
TR
VDR
RNA
polymerase II
Metabolism and mechanism of action of natural retinoids. ARAT, acyl-CoA:retinol acyl
transferase; CRABP, cellular retinoic acid-binding protein; CRBP, cellular retinol-binding
protein; LRAT, lecithin:retinol acyl transferase; PPAR, peroxisome proliferator-activated
receptor; RA, retinoic acid; RAR, retinoic acid receptor; RBP, retinol-binding protein; RE,
retinyl esters; REH, retinyl ester hydrolase; RXR, retinoid X receptor; STRA6, stimulated
by retinoic acid 6; TR, thyroid receptor; VDR, vitamin D3 receptor.
Bolognia 2018
9
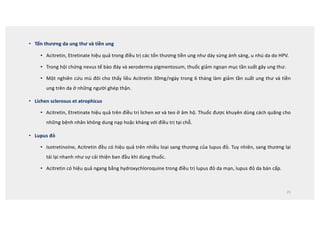
Tên thuốc Thế
hệ
Hấpthu và sinh khả dụng Thải trừ
Đỉnh
(giờ)
Sinh khả
dụng (%)
Gắn protein T1/2 Chuyển hóa Thải trừ
Tretinoin 1 1-2 - Albumin 99% 40-60
phút
Gan Mật, nước tiểu
Isotretinoin 1 3 25 Albumin 99% 10-20h Gan Mật, nước tiểu
Etretinate 2 4 44 Lipoprotein
99%
80-160
ngày
Gan Mật, nước tiểu
Acitretin 2 4 60 Albumin 95% 50h Gan Mật, nước tiểu
Bexarotene 3 2 Không có
dữ kiện
Protein HT
99%
7-9h Gan Gan mật
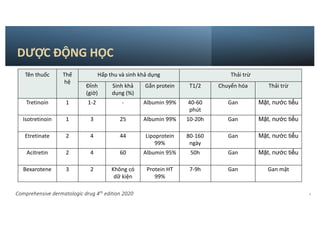
DƯỢC ĐỘNG HỌC
Comprehensive dermatologic drug 4th
edition 2020
10.
DƯỢC ĐỘNG HỌC
•Isotretinoin, Acitretin/Etretinate, Bexarotene khác nhau về độc tính, dược động học
và hiệu quả lâm sàng.
• Do tính chất ưa mỡ nên sinh khả dụng của tất cả các thuốc này đều tăng nếu dùng
chung với thức ăn, đặc biệt thức ăn nhiều dầu mỡ.
• Chuyển hoá bằng con đường oxy hoá và được cắt nhỏ thành chất không hoạt tính và
có tính ưa nước, sau đó thải ra bởi thận.
10
11.
Isotretinoin
• T ½20h (T ½ của ATRA là 1h)
• > 99% thuốc gắn với protein(Albumin)
• Dự trữ tại gan và mô mỡ
• Sau điều trị, lượng thuốc nội sinh và chất chuyển hoá vẫn còn tồn tại 2
tuần à do đó phải ngừa thai cho đến 1 tháng sau khi ngưng điều trị.
11
12.
Acitretin và Etretinate
•Những thí nghiệm trên động vật và các thử nghiệm lâm sàng cho thấy hiệu quả ngang nhau giữa Acitretin và Etretinate khi
điều trị các rối loạn về sừng hoá.
• Acitretin đào thải nhanh hơn Etretinate vì Etretinate ưa mỡ gấp 50 lần, gắn chặt với các lipoprotein trong khi Acitretin gắn
với albumin. Dù có dùng chung với thức ăn, sự hấp thu của thuốc cũng thay đổi nhiều.
• T ½ bán thải của Acitretin là 2 ngày. Trong khi đó Etretinate tích tụ trong mô mỡ và phóng thích một cách từ từ, T ½ ban
thải có thể lên đến 120 ngày. Do đó một số nhà sản xuất khuyến cao nên nới rộng thời gian ngừa thai lên 2 năm (tại Mỹ là
3 năm) nếu trong khi dùng Acitretin mà có uống rượu vì Etretinate có thể được tạo thành từ Acitretin khi uống rượu.
• Acitretine có nhiều ưu điểm vượt trội hơn Etretinate về dược động học vì nó được đào thải nhanh hơn, do đó để sử dụng
Acitretine an toàn, cấm uống rượu trong và sau 2 tháng kể từ khi ngưng sử dụng Acitretin.
12
13.
Bexarotene
• Mạnh hơngấp 100 lần về khả năng tác dụng trên receptors X
• Dùng chung với thức ăn có mỡ
• > 99% gắn với protein
• T ½ là 7-9h
• Không thải qua nước tiểu
13
15
CHỈ ĐỊNH
NA)-binding proteinsand functioning as trans-acting tran-
iption modulating factors.
The genes regulated by retinoids contain a retinoic acid
ponse element (RARE), which is a DNA sequence to which
RAR-RXR heterodimer binds. Upon binding of a ligand, the
AR-RXR heterodimer acts a transcription factor, resulting in the
pression of a number of proteins involved in growth and regula-
n.24 The retinoid-receptor complex can also act in an indirect
hion by antagonizing the action of other transcription factors,
cifically activating protein 1 (AP-1).25 The clinical effects of
temic retinoids in dermatology are related to their ability to
ect pathways involved in inflammation,26,27 cellular differentia-
n,28 apoptosis,29 and sebaceous gland activity.30 In addition to
ir actions on the skin, retinoids exert broad effects in multiple
ues, a complete description of which is beyond the scope of
s chapter.
inical Use
x 22.13,4,31,32 lists indications for the various systemic retinoids.
actical Considerations
ncomitant vitamin A therapy should be limited to less than
00 IU vitamin A daily. Oral administration with milk or
ty foods (ideally in moderation) enhances retinoid absorp-
n. Patients should be advised to avoid an excessively fatty diet.
omen with childbearing potential must not consume ethanol
ring and up to 2 months after cessation of acitretin therapy. In
male patients of nonreproductive potential and in males, this
nversion of acitretin to etretinate is not clinically important.
S Food and Drug Administration-Approved
dications
ree dermatoses have FDA approval for systemic retinoid use
severe subsets, as outlined in Box 22.1 and in the sections that
low:
Acitretin (Soriatane) for psoriasis;
Tazarotene – + + – – – RAR-β, γ > α
No RXR
CRABP, Cytosolic retinoic acid-binding protein; RA, retinoic acid; RAR, retinoic acid receptor; RXR, retinoid X receptor.
US Food and Drug Administration-Approved Indications
Psoriasis (Acitretin)
Severe plaque-type
psoriasis31-35
Pustular psoriasis—
generalized36
Pustular psoriasis—localized37
Combination Therapy
With UVB or PUVA39-45
With cyclosporine46
With biologic therapies47,48
Acne Vulgaris (Isotretinoin)
Nodulocystic acne 50-54
Recalcitrant, especially if any scarring
tendency55
Mycosis Fungoides (Bexarotene)
Resistant to at least one systemic
therapy56-57
Other Dermatologic Usesa
Follicular Disorders
Acne-related conditions
Gram-negative folliculitis
HIV-associated eosinophilic
folliculitis
Acne with solid facial edema
Rosacea63-66
Papulopustular (recalcitrant
to other therapies)
Granulomatous rosacea
Hidradenitis suppurativa67-69
Dissecting cellulitis of scalp70-72
Disorders of Keratinization
Darier disease73-75
Pityriasis rubra pilaris76-81
Ichthyosis spectrum82-86
Keratodermas
Chemoprevention of Malignancies
Organ transplantation patients88-90, 92
Syndromes with increased risk
cutaneous malignancy
Bazex syndrome
Nevoid basal cell carcinoma
syndrome93
Muir-Torre syndrome
Xeroderma pigmentosa93
Frequent BCC or SCC
(nonimmunosuppressed)
Kaposi sarcoma
Other Inflammatory Dermatoses
Lupus erythematosus (cutaneous
features)95-97
Lichen planus—oral erosive,
palmoplantar98
Lichen sclerosus et atrophicus
Miscellaneous
Graft-versus-host disease
Human papillomavirus infections
aNot a comprehensive list of references for off-label uses—if no reference number listed earlier, see refer-
ences 61 and 62 for pertinent citations, as well as consulting various reviews in the Bibliography section.
BCC, Basal cell carcinoma; HIV, human immunodeficiency virus; PUVA, psoralen and ultraviolet A; SCC,
squamous cell carcinoma; UVB, ultraviolet B.
Systemic Retinoids Indications
’BOX 22.1
16.
Mụn trứng cá
•Chỉ duy nhất 1 loại retinoids hệ thống được chỉ định cho mụn trứng cá thông thường, đó là
isotretinoin.
• Trong tất cả các retinoids, chỉ có isotretinoine làm giảm tiết bã nhờn và giảm kích thước tuyến bã.
Sử dụng với loại mụn trứng cá nang nốt, mụn trứng cá kháng trị. Isotretinoin rất hiệu quả do tác
động lên tất cả các yếu tố sinh bệnh: tăng tiết bã nhờn, rối loạn sừng hoá (tạo comedon), vi khuẩn.
• FDA approved cho chỉ định Isotretinoin với mụn trứng cá nang nốt kháng trị, được định nghĩa là các
sang thương viêm 5mm không đáp ứng với các phương pháp can thiệp trước đó, kể cả kháng sinh
hệ thống. Một đồng thuận hiện nay là định nghĩa nặng là bệnh ảnh hưởng nhiều đến chất lượng
cuộc sống, không dựa trên chỉ số lượng sang thương nữa.
16
17.
Mụn trứng cá
•Trong các nghiên cứu trước đó cho thấy tỉ lệ đáp ứng lui bệnh là như nhau với các liều 0.1-0.5 và
1.0mg/kg/ngày trong 20 tuần. Dùng liều thấp được ghi nhận tỉ lệ tái phát cao hơn.
• Liều trung bình 0.5-1mg/kg/ngày cho đến khi liều tích luỹ đạt 120-150mg/kg là hợp lý cho đa số
các trường hợp. Khởi đầu liều như thế nào tuỳ thuộc vào độ nặng của mụn.
• Mụn có thể nặng hơn trong 4-6 tuần đầu, nhưng sau đó sẽ giảm dần và đạt hiệu quả khống chế
sau 4-5 tháng.
• Nếu có tái phát thì việc sử dụng Isotretinoin đợt sau cũng cho hiệu quả đáp ứng kiểm soát bệnh
tốt hơn.
17
18.
Vảy nến: RetinoidsAs Monotherapy
• FDA approved cho chỉ định vảy nến.
• Liều cao 50mg và 75mg hiệu quả cao hơn liều thấp (10 và 25 mg).
• Hiệu quả PASI-50 và PASI-75 là 76% và 46%
• Hiệu quả lâm sàng giảm vảy, giảm dỏ, giảm ngứa nhưng có thể không giảm BSA.
• Hiệu quả có thể thấy sau 4-6ws nhưng có thể cần 3-4 tháng để có hiệu quả đầy đủ.
• Một nghiên cứu cho thấy tỉ lệ hiệu quả của acitretin so với các điều trị khác: Vảy nến GPP hiệu quả trên 84%
methotrexate in 76% cyclosporine CsA 71% PUVA 46%
• Hiệu quả tốt trên thể mụn mủ lòng bàn tay, mụn mủ toàn thân
• Liều khởi đầu nên là 25mg/ngày tăng dần lên cân bằng hiệu quả và dung nạp của bệnh nhân. Duy trì 10 hoặc
25mg/ngày cho giai đoạn duy trì lâu dài.
18
19.
• So vớiAcitretin đơn trị liệu hoặc ánh sáng đơn trị liệu thì kết hợp 2 biện pháp trên đem lại hiệu quả có thể
giảm tần suất điều trị, thời gian và liều tích luỹ. Liều thấp Acitretin 10-25mg/ngày hiệu quả khi dùng phối
hợp chung với liệu pháp ánh sáng. Thuốc làm đáp ứng với UVB và PUVA nhanh hơn, hoàn toàn hơn.
• Kết hợp acitretin-UV therapy: bắt đầu liều thấp (25 mg) acitretin x 2 weeks trước khi bắt đầu phototherapy.
Lưu ý điều chỉnh liều UV thấp xuống vì có tác động của acitretin. Ví dụ nếu BN đang dùng liều chiếu UV mà
có thêm acitretin thì liều cần giảm xuống 30-50% sau khi bắt đầu acitretin 7 ngày.
• Acitretin có thể kết hợp với MTX hoặc cyclosporine nhưng lưu ý nguy cơ tác dụng phụ à hết sức cân nhắc.
• ‘Sequential regimen’: cyclosporine khởi động trước, đạt hiệu quả à giảm liều và ngưng trong 3-4 tháng à
trong thời gian đó thì thêm acitretin và duy trì tiếp acitretin sau ngưng cyclosporine.
19
Vảy nến: Retinoids in Combination Therapy
20.
• Acitretin khônggây ức chế miễn dịch, kết hợp với thuốc sinh học cho hiệu quả cao.
• RCT: Hiệu quả của Etanercept 25 mg mỗi tuần + acitretin 0.4 mg/kg daily = etanercept 25
mg 2 lần/tuần acitretin 0.4 mg/kg mỗi ngày đơn trị liệu (an toàn tương đương)
• Chưa có data về kết hợp với thuốc khác.
20
Vảy nến: Retinoids with Biologic Agents
21.
21
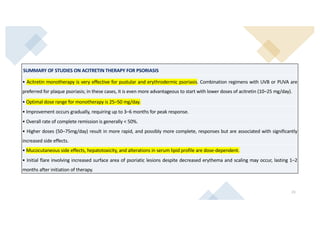
SUMMARY OF STUDIESON ACITRETIN THERAPY FOR PSORIASIS
• Acitretin monotherapy is very effective for pustular and erythrodermic psoriasis. Combination regimens with UVB or PUVA are
preferred for plaque psoriasis; in these cases, it is even more advantageous to start with lower doses of acitretin (10–25 mg/day).
• Optimal dose range for monotherapy is 25–50 mg/day.
• Improvement occurs gradually, requiring up to 3–6 months for peak response.
• Overall rate of complete remission is generally 50%.
• Higher doses (50–75mg/day) result in more rapid, and possibly more complete, responses but are associated with significantly
increased side effects.
• Mucocutaneous side effects, hepatotoxicity, and alterations in serum lipid profile are dose-dependent.
• Initial flare involving increased surface area of psoriatic lesions despite decreased erythema and scaling may occur, lasting 1–2
months after initiation of therapy.
22.
Lymphoma tế bàoT ở da
• Năm 1999, FDA chính thức công nhận Bexarotene là phương pháp điều trị CTCL
khi đã kháng với ít nhất 1 thuốc điều trị toàn thân.
• Trong giai đoạn sớm cũng như muộn, Bexarotene đơn trị liệu có hiệu quả cải
thiện 50-60% trong đó hầu hết bệnh nhân đáp ứng với liều mỗi ngày là
300mg/m2 hoặc hơn trong 2 tháng đầu điều trị.
• Cơ chế chưa rõ, nhưng được cho là do apoptosis tế bào ác tính.
22
23.
Các chỉ địnhkhác
• Bệnh vảy cá
• Hiệu quả tốt nhất được thấy khi điều trị vảy cả bẩm sinh không có bóng nước (lamellar ichthyosis).
• Điều trị đỏ da toàn thân dạng vảy cá có bóng nước có thể gây tăng tạo bóng nước.
• Kết quả tốt cũng được ghi nhận khi điều trị vảy cá thường và vảy các liên quan nhiễm sắc thể X, tuy nhiên vì bệnh cũng
giới hạn nên ít cần phải điều trị thuốc.
• Bệnh Darier
• Dạng nặng của bệnh Darier là một chỉ định tốt cho retinoids
• Thận trọng khởi đầu với liều 10mg/ngày để tránh bùng phát bệnh, thường tăng lên đến 20mg/ngày là có thể cải thiện
được bệnh.
• Dùng lâu dài để tránh tái phát
• Liều thấp Isotretinoine được dùng trên phụ nữ bị bệnh Darier.
• Kết hợp với kháng sinh làm tăng hiệu quả lâm sàng vì thực tế các tổn thương thường bị nhiễm trùng.
23
24.
• Vảy phấnđỏ nang lông (Etretinate Isotretinoine)
• Điều trị sớm làm tăng hi vọng chữa sạch sang thương.
• Ở những ca nặng, cần phối hợp thêm Methotrexate để đạt hiệu quả nhưng nguy cơ tăng độc.
• Etretinate hiệu quả hơn hẳn Isotretinoine trong điều trị vảy phấn đỏ nang lông khởi phát ở tuổi trưởng thành.
• Trứng cá đỏ
• Chỉ định: bệnh nặng hoặc kháng trị, tác dụng trên các thương tổn viêm thương tổn mạch máu.
• Liều 10mg/ngày là đủ có hiệu quả.
• Chỉ định: trứng cá đỏ kèm theo tăng tiết bã nhờn.
• Viêm tuyến mồ hôi nung mủ
• Isotretinoine ít hiệu quả, tuy nhiên có thể dùng trong vòng vài tuần, vài tháng trước phẫu thuật.
• Acitretin, Etretinate thành công trong một số ca mà sang thương viêm nhiều không thích hợp cho phẫu thuật.
24
25.
• Tổn thươngda ung thư và tiền ung
• Acitretin, Etretinate hiệu quả trong điều trị các tổn thương tiền ung như dày sừng ánh sáng, u nhú da do HPV.
• Trong hội chứng nevus tế bào đáy và xeroderma pigmentosum, thuốc giảm ngoạn mục tần suất gây ung thư.
• Một nghiên cứu mù đôi cho thấy liều Acitretin 30mg/ngày trong 6 tháng làm giảm tần suất ung thư và tiền
ung trên da ở những người ghép thận.
• Lichen sclerosus et atrophicus
• Acitretin, Etretinate hiệu quả trên điều trị lichen xơ và teo ở âm hộ. Thuốc được khuyên dùng cách quãng cho
những bệnh nhân không dung nạp hoặc kháng với điều trị tại chỗ.
• Lupus đỏ
• Isotretinoine, Acitretin đều có hiệu quả trên nhiều loại sang thương của lupus đỏ. Tuy nhiên, sang thương lại
tái lại nhanh như sự cải thiện ban đầu khi dùng thuốc.
• Acitretin có hiệu quả ngang bằng hydroxychloroquine trong điều trị lupus đỏ da mạn, lupus đỏ da bán cấp.
25
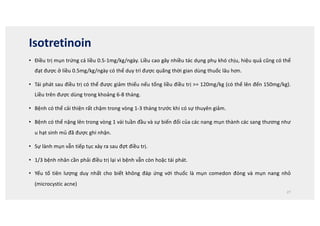
Isotretinoin
• Điều trịmụn trứng cá liều 0.5-1mg/kg/ngày. Liều cao gây nhiều tác dụng phụ khó chịu, hiệu quả cũng có thể
đạt được ở liều 0.5mg/kg/ngày có thể duy trì được quãng thời gian dùng thuốc lâu hơn.
• Tái phát sau điều trị có thể được giảm thiểu nếu tổng liều điều trị = 120mg/kg (có thể lên đến 150mg/kg).
Liều trên được dùng trong khoảng 6-8 tháng.
• Bệnh có thể cải thiện rất chậm trong vòng 1-3 tháng trước khi có sự thuyên giảm.
• Bệnh có thể nặng lên trong vòng 1 vài tuần đầu và sự biến đổi của các nang mụn thành các sang thương như
u hạt sinh mủ đã được ghi nhận.
• Sự lành mụn vẫn tiếp tục xảy ra sau đợt điều trị.
• 1/3 bệnh nhân cần phải điều trị lại vì bệnh vẫn còn hoặc tái phát.
• Yếu tố tiên lượng duy nhất cho biết không đáp ứng với thuốc là mụn comedon đóng và mụn nang nhỏ
(microcystic acne)
27
28.
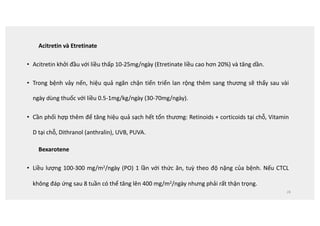
Acitretin và Etretinate
•Acitretin khởi đầu với liều thấp 10-25mg/ngày (Etretinate liều cao hơn 20%) và tăng dần.
• Trong bệnh vảy nến, hiệu quả ngăn chặn tiến triển lan rộng thêm sang thương sẽ thấy sau vài
ngày dùng thuốc với liều 0.5-1mg/kg/ngày (30-70mg/ngày).
• Cần phối hợp thêm để tăng hiệu quả sạch hết tổn thương: Retinoids + corticoids tại chỗ, Vitamin
D tại chỗ, Dithranol (anthralin), UVB, PUVA.
Bexarotene
• Liều lượng 100-300 mg/m2/ngày (PO) 1 lần với thức ăn, tuỳ theo độ nặng của bệnh. Nếu CTCL
không đáp ứng sau 8 tuần có thể tăng lên 400 mg/m2/ngày nhưng phải rất thận trọng.
28
29.
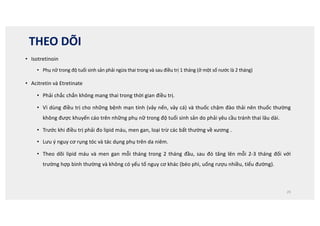
THEO DÕI
• Isotretinoin
•Phụ nữ trong độ tuổi sinh sản phải ngừa thai trong và sau điều trị 1 tháng (ở một số nước là 2 tháng)
• Acitretin và Etretinate
• Phải chắc chắn không mang thai trong thời gian điều trị.
• Vì dùng điều trị cho những bệnh mạn tính (vảy nến, vảy cá) và thuốc chậm đào thải nên thuốc thường
không được khuyến cáo trên những phụ nữ trong độ tuổi sinh sản do phải yêu cầu tránh thai lâu dài.
• Trước khi điều trị phải đo lipid máu, men gan, loại trừ các bất thường về xương .
• Lưu ý nguy cơ rụng tóc và tác dụng phụ trên da niêm.
• Theo dõi lipid máu và men gan mỗi tháng trong 2 tháng đầu, sau đó tăng lên mỗi 2-3 tháng đối với
trường hợp bình thường và không có yếu tố nguy cơ khác (béo phì, uống rượu nhiều, tiểu đường).
29
30.
30
259
CHAPTER 22 SystemicRetinoids
Baseline
Examination
t
$BSFGVMIJTUPSZBOEQIZTJDBMFYBNJOBUJPO
t
*EFOUJGZUIPTFQBUJFOUTBUJODSFBTFESJTLGPSUPYJDJUZPSBEWFSTFFGGFDUT
t
%PDVNFOUDPODPNJUBOUNFEJDBUJPOTUIBUNBZJOUFSBDUXJUISFUJOPJET TFF
Table 22.4)
Laboratorya
t
4FSVNPSVSJOFQSFHOBODZUFTUb (in women of childbearing potential)
t
$PNQMFUFCMPPEDPVOU $#$ XJUIQMBUFMFUT
t
-JWFSGVODUJPOUFTUT 45-5BMLBMJOFQIPTQIBUBTF CJMJSVCJO
t
-JQJEQSPmMFEVSJOHGBTUJOHc (triglycerides, total cholesterol, LDL and HDL
cholesterol)
t
3FOBMGVODUJPOUFTUT CMPPEVSFBOJUSPHFO DSFBUJOJOF
t
0QUJPOBMVSJOBMZTJT JGQBUJFOUTIBWFSFOBMEJTFBTF QSPUFJOVSJB EJBCFUFT
or hypertension)
Special Tests
t
$POTJEFSCBTFMJOFYSBZTPGXSJTUT BOLMFTPSUIPSBDJDTQJOFJGQMBOlong-
term retinoid therapy
t
$POTJEFSPQIUIBMNPMPHJDFYBNJOBUJPOJGQBUJFOUTIBWFBIJTUPSZPG
cataracts or retinopathy
Follow-Up
Examination
Clinical evaluation monthly for first 3–6 months, then every 3 months
t
TTFTTNFOUPGQBUJFOUSFTQPOTF JNQSPWFNFOU BOEDPNQMBJOUTPG
adverse effects
t
3PVUJOFQIZTJDBMFYBNJOBUJPOPGMFTJPOBMTLJO
t
EEJUJPOBMGPDVTFEQIZTJDBMFYBNJOBUJPOPGBOZSFQPSUFEBEWFSTFFGGFDUT
Laboratorya,d
Monthly for the first 3–6 months, then every 3 months
t
$PNQMFUFCMPPEDPVOU $#$ XJUIQMBUFMFUb
t
-JWFSGVODUJPOUFTUT 45-5
t
'BTUJOHMJQJETUVEJFTc (triglycerides, cholesterol–order LDL and HDL
cholesterol periodically)
t
3FOBMGVODUJPOUFTUTe (optional urinalysis)
t
4FSVNPSVSJOFQSFHOBODZUFTUNPOUIMZGPSXPNFOPGDIJMECFBSJOH
potential (and at end of therapy)
Special Tests
Periodically as indicated by symptoms
t
$POTJEFSZFBSMZYSBZTPGXSJTUT BOLMFTPSUIPSBDJDTQJOFXJUIMPOHUFSN
retinoid therapy
t
3BEJPHSBQIJDTUVEJFTPGTJHOJmDBOUMZTZNQUPNBUJDKPJOUTXJUIMPOHUFSN
therapy
t
$PNQMFUFPQIUIBMNPMPHJDFYBNJOBUJPOJGQBUJFOUTSFQPSUWJTVBMDIBOHFT
(see text for components)
aMore frequent surveillance is needed if laboratory parameters are abnormal or with high-risk
patients
bGuidelines require two pregnancy tests before isotretinoin therapy. Isotretinoin therapy should
be initiated on the second day of next normal menstrual cycle or 11 or more days after last
unprotected intercourse
cCheck lipids after a 12 hours fast and 36 hour or longer abstinence from ethanol
dWhen isotretinoin is used for a 20 week acne course, it is reasonable to discontinue monitoring
(other than pregnancy testing) after 8-12 weeks if laboratory results have been normal and the
dose is constant in asymptomatic patients
eRenal function and hematologic tests are infrequently altered by retinoids. Consider ordering
these tests every other time laboratory testing is done
ALT, Alanine transaminase; AST, aspartate transaminase, HDL, high density lipoprotein; LDH,
lactate dehydrogenase.
Isotretinoin and Acitretin Monitoring Guidelines
’BOX 22.8
Baseline
t
TTFTTNFOUPGQBUJFOUDMJOJDBMSFTQPOTFBOEGPSBEWFSTFTJEFFGGFDUT
Bexarotene Monitoring Guidelines
’BOX 22.9
31.
31
adverse effects
t
3PVUJOFQIZTJDBMFYBNJOBUJPOPGMFTJPOBMTLJO
t
EEJUJPOBMGPDVTFEQIZTJDBMFYBNJOBUJPOPGBOZSFQPSUFEBEWFSTFFGGFDUT
Renal function and hematologic tests are infrequently altered by retinoids. Consider ordering
these tests every other time laboratory testing is done
ALT, Alanine transaminase; AST, aspartate transaminase, HDL, high density lipoprotein; LDH,
lactate dehydrogenase.
Baseline
Examination
t
$BSFGVMIJTUPSZBOEQIZTJDBMFYBNJOBUJPO
t
*EFOUJGZUIPTFQBUJFOUTBUJODSFBTFESJTLGPSUPYJDJUZPSBEWFSTFFGGFDUTMJWFS
disease or cirrhosis, biliary tract disease, excessive alcohol consumption,
prior pancreatitis, thyroid disease, uncontrolled hyperlipidemia, uncontrolled
diabetes mellitus, HIV, leukopenia, chronic infection, cataracts
t
%PDVNFOUDPODPNJUBOUNFEJDBUJPOTUIBUNBZJOUFSBDUXJUISFUJOPJET TFF
Table 22.4)
Laboratorya
t
4FSVNQSFHOBODZUFTU JOXPNFOPGDIJMECFBSJOHQPUFOUJBM
t
$PNQMFUFCMPPEDPVOU $#$ XJUIQMBUFMFUTBOEEJGGFSFOUJBMDPVOU
t
-JWFSGVODUJPOUFTUT 45-5BMLBMJOFQIPTQIBUBTF CJMJSVCJO
t
-JQJEQSPmMFEVSJOHGBTUJOHb(triglycerides, total cholesterol, LDL and HDL
cholesterol)
t
3FOBMGVODUJPOUFTUT CMPPEVSFBOJUSPHFO DSFBUJOJOF
t
5IZSPJEGVODUJPOUFTUT54) 54
t
0QUJPOBMVSJOBMZTJT JGQBUJFOUTIBWFSFOBMEJTFBTFT QSPUFJOVSJB EJBCFUFT
or hypertension)
Special Tests
t
#BTFMJOFPQIUIBMNPMPHJDFYBNJOBUJPOJGQBUJFOUTIBWFBIJTUPSZPG
cataracts
Follow-Up
Examination
Clinical evaluation every 2 weeks for first 4–8 weeks, then monthly for the next
3 months; long-term clinical evaluation every 2–3 months
t
TTFTTNFOUPGQBUJFOUDMJOJDBMSFTQPOTFBOEGPSBEWFSTFTJEFFGGFDUT
t
EEJUJPOBMGPDVTFEQIZTJDBMFYBNJOBUJPOPGBOZSFQPSUFETJEFFGGFDUT
Laboratory
Every 1–2 weeks until the lipid response to Targretin is established (usually 2–4
wks), then as subsequently
t
-JQJEQSPmMFEVSJOHGBTUJOHb (triglycerides, total cholesterol, LDL and HDL
cholesterol)
Monthly for the first 3–6 months, then every 3 months
t
$PNQMFUFCMPPEDPVOU $#$ XJUIQMBUFMFUTBOEEJGGFSFOUJBMDPVOU
t
-JWFSGVODUJPOUFTUT 45-5 JGFMFWBUFEDBOBMTPPSEFSCJMJSVCJO
alkaline phosphatase
t
3FOBMGVODUJPOUFTUTc (optional urinalysis)
t
4FSVNPSVSJOFQSFHOBODZUFTUGPSXPNFOPGDIJMECFBSJOHQPUFOUJBM
(continue monthly indefinitely)
t
5IZSPJEGVODUJPOUFTUT54) BUMFBTU QPTTJCMZ54 as well (reasonable to
follow-up just 1–2 times)
Special Tests
t
3FQFBUPQIUIBMNPMPHJDFYBNJOBUJPOQFSJPEJDBMMZEVSJOHUSFBUNFOUJG
patients have a history of abnormal ocular findings before retinoid therapy
aMore frequent surveillance is needed if laboratory parameters are abnormal or with high-risk
patients
bCheck lipids after a 12 hours fast and 36 hour or longer abstinence from ethanol
cRenal function tests and urinalysis are infrequently altered by bexarotene. Consider ordering
these tests every other time laboratory testing is done
ALT, Alanine transaminase; AST, aspartate transaminase, HDL, high density lipoprotein; HIV,
human immunodeficiency virus; LDH, lactate dehydrogenase, TSH, thyroid stimulating hormone;
T4, thyroxine.
Bexarotene Monitoring Guidelines
’BOX 22.9
32.
32
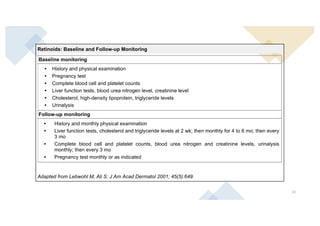
Retinoids: Baseline andFollow-up Monitoring
Baseline monitoring
• History and physical examination
• Pregnancy test
• Complete blood cell and platelet counts
• Liver function tests, blood urea nitrogen level, creatinine level
• Cholesterol, high-density lipoprotein, triglyceride levels
• Urinalysis
Follow-up monitoring
• History and monthly physical examination
• Liver function tests, cholesterol and triglyceride levels at 2 wk; then monthly for 4 to 6 mo; then every
3 mo
• Complete blood cell and platelet counts, blood urea nitrogen and creatinine levels, urinalysis
monthly; then every 3 mo
• Pregnancy test monthly or as indicated
Adapted from Lebwohl M, Ali S: J Am Acad Dermatol 2001; 45(5):649.
VII. NGUY CƠ VÀ THẬN TRỌNG
Tác dụng phụ nặng
Quái thai
- Bệnh lí bào thai do retinoid
Tiêu hóa
Comprehensive dermatologic drugtherapy, 2020
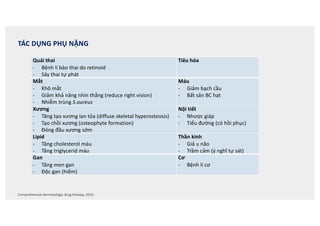
TÁC DỤNG PHỤ NẶNG
Quái thai
- Bệnh lí bào thai do retinoid
- Sảy thai tự phát
Tiêu hóa
Mắt
- Khô mắt
- Giảm khả năng nhìn thẳng (reduce right vision)
- Nhiễm trùng S.aureus
Máu
- Giảm bạch cầu
- Bất sản BC hạt
Xương
- Tăng tạo xương lan tỏa (diffuse skeletal hyperosteosis)
- Tạo chồi xương (osteophyte formation)
- Đóng đầu xương sớm
Nội tiết
- Nhược giáp
- Tiểu đường (có hồi phục)
Lipid
- Tăng cholesterol máu
- Tăng triglycerid máu
Thần kinh
- Giả u não
- Trầm cảm (ý nghĩ tự sát)
Gan
- Tăng men gan
- Độc gan (hiếm)
Cơ
- Bệnh lí cơ
35.
35
Da
• Khô da
•Bong vảy lòng bàn tay bàn chân và ngón tay
• Viêm da do retinoid
• Nhạy cảm ánh sáng
• U hạt sinh mủ
• Cảm giác châm chích ở lòng bàn tay, lòng bàn chân
• Nhiễm trùng do S.aureus
Mũi
• Khô niêm mạc mũi
• Giảm tiết nhày niêm mạc mũi
• Chảy máu cam (Epistaxis)
Cơ xương
• Đau cơ
• Đau khớp
• Mệt, yếu cơ
• Viêm gân
Tóc
• Telogen effluvium
• Khô tóc
Thần kinh
• Nhức đầu
• Trầm cảm nhẹ
Móng
• Dễ gãy móng do móng mềm
• Li móng
• Viêm quanh móng
Tiêu hóa
• Nôn
• Tiêu chảy
Miệng
• Viêm môi, nhất là môi dưới
• Khô miệng
• Đau miệng và lưỡi
Mắt
• Khô mắt
• Viêm kết mạc mi
• Chói mắt
36.
Nguy cơ quáithai
• Khả năng sinh quái thai là tác dụng phụ nguy hiểm nhất.
• Những tác dụng phụ của retinoids là do hội chứng tăng vitamin A, bao gồm: cấp (tổn thương da niêm, bất thường xét
nghiệm), mạn (bất thường xương, hiếm xảy ra)
• Tác dụng sinh quái thai: Acitretin gây quái thai. Trong môi trường có rượu, acitretin bị ester hoá thành Etretinate,
Etretinate tồn tại rất lâu trong mô à acitretin không dùng cho phụ nữ có khả năng sinh sản và muốn có con trong vòng 3
năm tới.
• Tổn thương: Hệ thính giác (auditory), tim mạch, hàm mặt, mắt, xương chi và xương trục, thần kinh trung ương (não úng
thuỷ, não nhỏ), bất thường tuyến ức
• Cơ chế: độc trên các tế bào thần kinh “nghỉ ngơi”, đặc biệt nếu tiếp xúc trong suốt tuần thứ 4 của thai kì. Ở nam, thuốc
không gây bất thường quá trình tạo tinh trùng, hình dạng hay gây chết tinh trùng, tuy nhiên cũng cần phải tránh.
36
37.
HƯỚNG DẪN THỬTHAI VÀ NGỪA THAI AN TOÀN
37
• 2 test âm tính thử nước tiểu hoặc máu với độ nhạy ít nhất là 25mUI/mL trước khi kê toa điều trị.
• Test thử thai lần 2 được làm trong 5 ngày đầu của chu kì kinh trước khi bắt đầu uống thuốc.
• Với bệnh nhân vòng chu kì không đều thì test lần 2 thực hiện ít nhất 11 ngày sau khi quan hệ tình dục không bảo vệ
(không dùng ít nhất 2 biện pháp ngừa thai).
• Mỗi tháng bệnh nhân phải thử test thai (nước tiểu hoặc máu).
Cần sử dụng phối hợp ít nhất 2 biện pháp ngừa thai (ít nhất 1 biện pháp nguyên phát), thời gian là ít nhất 1 tháng trước điều
trị và ít nhất 1 tháng sau điều trị.
Hiệu quả của ngừa thai chia làm 2 loại:
- Nguyên phát (primary): thắt ống dẫn trứng, người cùng quan hệ đã cắt ống dẫn tinh, dụng cụ tử cung, thuốc ngừa thai
uống, hormone ngừa thai tiêm/cấy.
- Thứ phát (secondary): chu kì kinh, bao cao su, mũ tử cung (tất cả phải kèm theo chất diệt tinh trùng)
Không cần phối hợp 2 biện pháp ngừa thai nếu bệnh nhân kiêng không quan hệ hoặc đã cắt tử cung
38.
Tác dụng trênda niêm
• Thường ở liều 50mg/ngày. Hầu hết đều có khô môi, da, niêm (tác dụng này có liên quan liều, nguyên nhân do giảm
tiết nhờn, giảm độ này lớp sừng). Viêm môi xảy ra sớm nhất và thường gặp nhất, sau đó là đến viêm kết mạc mi,
khô mắt, khô mũi, khô miệng. Khô da kết hợp với mề đay, tróc da (nhất là bàn chân, bàn tay). Da dễ tổn thương và
nứt ngón tay.
• Tăng nhạy cảm ánh sáng do giảm độ dày lớp sừng.
• Bexarotene có ít tác dụng phụ trên da niêm và mắt hơn những thuốc khác. Viêm da tróc vảy là tác dụng phụ
thường gặp nhất của Bexarotene.
• Vi khuẩn S.aureus dường như có thể gây nhiễm trùng da do hiện tượng giảm tiết bã nhờn do retinoids.
• Rất nhiều phát ban ở da, gọi là viêm da do retinoids đôi khi rất khó phân biệt với một bệnh vảy nến hay bệnh chàm
thể tạng tiềm ẩn. 38
39.
Tác dụng trênmắt
• Viêm kết mạc mi: xảy ra ở 1/3 bệnh nhân với những mức độ khác nhau, cần tránh đeo kính sát tròng.
• Cần khám chuyên khoa mắt nếu dùng nước mắt nhân tạo và kháng sinh nhỏ mắt thất bại.
Tóc-móng
• Rụng tóc lan toả hay từng vùng (tellogen effluvium) khi dùng liều cao và sau nhiều tháng sử dụng: Acitretin Isotretinoine
• Móng mỏng và bất thường giống viêm mé móng (paronychia) với mô hạt quanh móng.
Cơ xương: Xảy ra khi dùng liều cao và điều trị dài ngày các rối loạn về sự keratin hoá.
• Đau xương
• Biến đổi tăng tạo xương, calci hoá gân và dây chằng (liều cao dài ngày)
• Loãng xương
• Đau cơ (có thể tăng CPK), bệnh lí cơ: hiếm
39
40.
Tác dụng trênhệ thần kinh: Hiếm gặp
• Tăng áp lự nội sọ (nhức đầu, ói, bất thường thị giác…)
• Dùng chung Isotretinoine và tetracycline gây tăng nguy cơ tăng áp lực nội sọ.
Viêm tuỵ
• 1 trường hợp tử vong đã được báo cáo.
• Viêm tuỵ trên 3 bệnh nhân điều trị Bexarotene liều = 300mg/m2/ngày kèm với tăng
triglyceride máu.
Nhược giáp: 40% bệnh nhân CTCL điều trị với bexarotene có nhược giáp lâm sàng và xét nghiệm
(hồi phục hoàn toàn sau ngưng thuốc)
Thận: Độc thận không phải là tác dụng độc của retinoids, tuy nhiên cẩn theo dõi sát.
Bệnh ruột viêm: rất hiếm
40
41.
Tăng lipid máu:Thường gặp
• Isotretinoin, Bexarotene Acitretin
• Tuỳ theo loại và liều dùng mà triglyceride tăng từ 50-80%, cholesterol tăng 30-50% à có thể gây ban vàng và
viêm tuỵ.
• Tăng nhẹ triglyceride (300-500mg/dL) có thể kiểm soát bằng giảm cân, tăng vận động thể lực, hạn chế
ngọt, béo và rượu. Nếu tăng trên 500mg/dL cần giảm liều retinoids và dùng thêm thuốc giảm lipid máu
(statin, niacin) và theo dõi lipid máu thường xuyên hơn. Ngưng điều trị nếu triglyceride 800mg/dL vì có
nguy cơ gây viêm tuỵ.
• Tăng lipid máu có thể trở về bình thường sau khi ngưng thuốc.
• Gemfibrozil là một chất ức chế mạnh con đường cytochrome P-450, cùng một con đường chuyển hoá của
bexarotene. Do đó, khi dùng chung với bexarotene, gemfibrozil gây tăng nồng độ bexarotne và triglycerides
máu. Chống chỉ định dùng chung Gemfibrozil và bexarotene.
• Cơ chế: tăng biểu hiện apolipo C3 ngăn hấp thu lipid từ VDRL vào tế bào.
41
42.
Độc gan
• Tăngmen gan (Acitretin, Etretinate bexarotene, Isotretinoine)
• Xảy ra 2-8 tuần sau điều trị
• Ngưng điều trị nếu men gan tăng 3 lần trị số bình thường trên.
• Độc gan nặng 1% trường hợp.
Độc máu
• Giảm bạch cầu hạt (28% bệnh nhân dùng bexarotene điều trị CTCL): xảy ra 2-4 tuần sau khởi đầu
điều trị, ít gặp hơn ở những retinoids khác.
• Chảy máu do Isotretinoine do li giải fibrin đã được báo cáo.
42
43.
BIẾN CHỨNG
• Hầuhết các biến chứng do retinoids đều có thể phòng chống bằng cách lựa chọn bệnh nhân, liều lượng,
ngưng điều trị, theo dõi thường xuyên.
• Chống chỉ định tuyệt đối: thai kì, người có ý định mang thai, không có biện pháp ngừa thai hiệu quả, người
đang cho con bú.
• Chống chỉ định tương đối: giảm bạch cầu, nghiện rượu, tăng cholesterol, tăng triglyceride, suy gan thận,
nhược giáp (Bexarotene).
43
44.
ISOTRETINOIN
44
253
CHAPTER 22 SystemicRetinoids
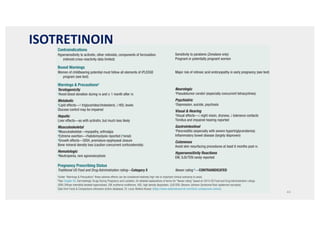
Contraindications
Hypersensitivity to acitretin, other retinoids, components of formulation
(retinoid cross-reactivity data limited)
Sensitivity to parabens (Zenatane only)
Pregnant or potentially pregnant women
Boxed Warnings
Women of childbearing potential must follow all elements of iPLEDGE
program (see text)
Major risk of retinoic acid embryopathy in early pregnancy (see text)
Warnings Precautionsa
Teratogenicity
aAvoid blood donation during rx and ≥ 1 month after rx
Metabolic
aLipid effects—↑ triglycerides/cholesterol, ↓ HDL levels
Glucose control may be impaired
Hepatic
Liver effects—as with acitretin, but much less likely
Musculoskeletal
aMusculoskeletal—myopathy, arthralgia
aExtreme exertion—rhabdomyolysis reported (arenal)
aGrowth effects—DISH, premature epiphyseal closure
Bone mineral density loss (caution concurrent corticosteroids)
Hematologic
aNeutropenia, rare agranulocytosis
Neurologic
aPseudotumor cerebri (especially concurrent tetracyclines)
Psychiatric
aDepression, suicide, psychosis
Visual Hearing
aVisual effects—↓ night vision, dryness, ↓ tolerance contacts
Tinnitus and impaired hearing reported
Gastrointestinal
aPancreatitis (especially with severe hypertriglyceridemia)
Inflammatory bowel disease (largely disproven)
Cutaneous
Avoid skin resurfacing procedures at least 6 months post rx
Hypersensitivity Reactions
EM, SJS/TEN rarely reported
Pregnancy Prescribing Status
Traditional US Food and Drug Administration rating—Category X Newer rating b—CONTRAINDICATED
aUnder “Warnings Precautions” these adverse effects can be considered relatively high risk or important clinical scenarios to avoid.
bSee Chapter 65, Dermatologic Drugs During Pregnancy and Lactation, for detailed explanations of terms for “Newer rating” based on 2015 US Food and Drug Administration rulings.
DISH, Diffuse interstitial skeletal hyperostosis; EM, erythema multiforme; HDL, high density lipoprotein; SJS/TEN, Stevens-Johnson Syndrome/Toxic epidermal necrolysis.
Data from Facts Comparisons eAnswers (online database). St. Louis: Wolters Kluwer. (https://www.wolterskluwercdi.com/facts-comparisons-online/).
Drug Risks Profile—Isotretinoin
’BOX 22.2
Contraindications
Hypersensitivity to acitretin, other retinoids, components of formulation (retinoid Women of childbearing potential (see exceptions in text)
Drug Risks Profile—Acitretin
’BOX 22.3
45.
45
aUnder “Warnings Precautions” these adverse effects can be considered relatively high risk or important clinical scenarios to avoid.
bSee Chapter 65, Dermatologic Drugs During Pregnancy and Lactation, for detailed explanations of terms for “Newer rating” based on 2015 US Food and Drug Administration rulings.
DISH, Diffuse interstitial skeletal hyperostosis; EM, erythema multiforme; HDL, high density lipoprotein; SJS/TEN, Stevens-Johnson Syndrome/Toxic epidermal necrolysis.
Data from Facts Comparisons eAnswers (online database). St. Louis: Wolters Kluwer. (https://www.wolterskluwercdi.com/facts-comparisons-online/).
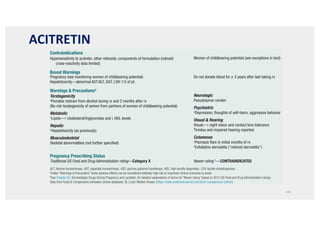
Contraindications
Hypersensitivity to acitretin, other retinoids, components of formulation (retinoid
cross-reactivity data limited)
Women of childbearing potential (see exceptions in text)
Boxed Warnings
Pregnancy (see monitoring women of childbearing potential)
Hepatotoxicity—abnormal AST/ALT, GGT, LDH 1/3 of pt.
Do not donate blood for ≥ 3 years after last taking rx
Warnings Precautionsa
Teratogenicity
aFemales restrain from alcohol during rx and 2 months after rx
(No risk teratogenicity of semen from partners of women of childbearing potential)
Metabolic
aLipids—↑ cholesterol/triglycerides and ↓ HDL levels
Hepatic
aHepatotoxicity (as previously)
Musculoskeletal
Skeletal abnormalities (not further specified)
Neurologic
Pseudotumor cerebri
Psychiatric
aDepression, thoughts of self-harm, aggressive behavior
Visual Hearing
Visual—↓ night vision and contact lens tolerance
Tinnitus and impaired hearing reported
Cutaneous
aPsoriasis flare in initial months of rx
aExfoliative dermatitis (“retinoid dermatitis”)
Pregnancy Prescribing Status
Traditional US Food and Drug Administration rating—Category X Newer rating b—CONTRAINDICATED
ALT, Alanine transaminase; AST, aspartate transaminase, GGT, gamma-glutamyl transferase; HDL, high density lipoprotein; LDH, lactate dehydrogenase.
aUnder “Warnings Precautions” these adverse effects can be considered relatively high risk or important clinical scenarios to avoid.
bSee Chapter 65, Dermatologic Drugs During Pregnancy and Lactation, for detailed explanations of terms for “Newer rating” based on 2015 US Food and Drug Administration rulings.
Data from Facts Comparisons eAnswers (online database). St. Louis: Wolters Kluwer. (https://www.wolterskluwercdi.com/facts-comparisons-online/).
Drug Risks Profile—Acitretin
’BOX 22.3
ACITRETIN
46.
TƯƠNG TÁC THUỐC
•Lưu ý không dùng chung với
• Tetracycline (tăng áp lực nội sọ, độc ánh sáng)
• Rượu (tăng chuyển acitretine - etretinate độc gan)
• Thuốc chứa vitamin A (tăng nhiễm độc viamin A)
• Gemfibrozil (làm tăng nồng độ bexarotene).
46
47.
47
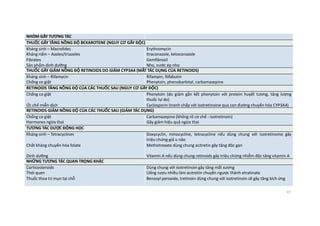
NHÓM GÂY TƯƠNGTÁC
THUỐC GÂY TĂNG NỒNG ĐỘ BEXAROTENE (NGUY CƠ GÂY ĐỘC)
Kháng sinh – Macrolides
Kháng nấm – Azoles/triazoles
Fibrates
Sản phẩm dinh dưỡng
Erythromycin
Itraconazole, ketoconazole
Gemfibrozil
Nho, nước ép nho
THUỐC GÂY GIẢM NỒNG ĐỘ RETINOIDS DO GIẢM CYP3A4 (MẤT TÁC DỤNG CỦA RETINOIDS)
Kháng sinh – Rifamycin
Chống co giật
Rifampin, Rifabutin
Phenytoin, phenobarbital, carbamazepine
RETINOIDS TĂNG NỒNG ĐỘ CỦA CÁC THUỐC SAU (NGUY CƠ GÂY ĐỘC)
Chống co giật
Ức chế miễn dịch
Phenytoin (do giảm gắn kết phenytoin với protein huyết tương, tăng lượng
thuốc tự do)
Cyclosporin (tranh chấp với isotretinoine qua con đường chuyển hóa CYP3A4)
RETINOIDS GIẢM NỒNG ĐỘ CỦA CÁC THUỐC SAU (GIẢM TÁC DỤNG)
Chống co giật
Hormones ngừa thai
Carbamazepine (không rõ cơ chế - Isotretinoin)
Gây giảm hiệu quả ngừa thai
TƯƠNG TÁC DƯỢC ĐỘNG HỌC
Kháng sinh – Tetracyclines
Chất kháng chuyển hóa folate
Dinh dưỡng
Doxycyclin, minocycline, tetracycline nếu dùng chung với isotretinoine gây
triệu chứng giả u não
Methotrexate dùng chung acitretin gây tăng độc gan
Vitamin A nếu dùng chung retinoids gây triệu chứng nhiễm độc tăng vitamin A
NHỮNG TƯƠNG TÁC QUAN TRỌNG KHÁC
Corticosteroids
Thói quen
Thuốc thoa trị mụn tại chỗ
Dùng chung với isotretinoin gây tăng mất xương
Uống rượu nhiều làm acitretin chuyển ngược thành etratinate
Benzoyl peroxide, tretinoin dùng chung với isotretinoin sẽ gây tăng kích ứng
48.
TÀI LIỆU THAMKHẢO
1. Alders Vahlquist, Stephane Kuenzli, and Jean-Hilaire Saurat - Fitzpatick’s dermatology in genernal medicine 7th
edition 2008 – Chapter 229 p. 2181-2185
2. Timothy J. Patton, Matthew J. Zirwas, and Stephen E. Wolverton – Comprehensive dermatologic drug 2nd
edition
2007 - Chapter 14 Systemic retinoids p. 275-300
3. Thomas P. Habif - Clinical dermatology - Chapter 8 - Psoriasis and Other Papulosquamous Diseases
4. Stephane Kuenzli, and Jean-Hilaire Saurat – Dermatology (Bolognia) 2003 - Chapter 127 retinoids p. 1991-2006
48