Case Selection onEndodontic Treatment, Treatment Planning,
and Assess Endodontic Case Complexity
D R . K H A L I D A L R A S H E D I
R E S T O R A T I V E D E N T A L S C I E N C E S
2.
INTRODUCTION
• Proper caseselection minimizes risks and increases
the chances of success.
• A study by Ingle and Beveridge found that 22% of
failures resulted from errors in case selection.
• Advances in technology, such as rotary instruments,
ultrasonics, microscopy, and new materials, have
improved treatment outcomes. However, case
selection remains the crucial first step in saving a
tooth.
3.
1st
step always shouldbe examination of the teeth and oral cavity . Clinician should
judge whether the teeth needed any kind of endodontic treatment or not.
• Indication
1. Teeth with pulpal inflammation
pulpal inflammation like irreversible pulpitis, pulpal necrosis require endodontic
treatment.
4.
2. Traumatized teeth
Fracturedteeth often require endodontic treatment which helps to maintain its
normal esthetic form and functional properties.
Vertical crown fracture in multi rooted teeth involving furcation can also be
treated by endodontic procedures like hemisection followed by root canal
therapy.
5.
3. Facilitation ofrestoration (Intentional Endodontic Treatment).
Occasionally, intentional endodontic treatment of teeth with perfectly vital
pulps may be necessary. Examples of situations requiring intentional endodontic
treatments include hyper erupted teeth or drifted teeth that must be reduced so
drastically that the pulp is certain to be involved.
On other occasions, a pulp is intentionally removed and the canal filled so that
a post and core may be placed for increased crown retention.
6.
Contraindicating
1- Insufficient periodontalsupport. In Teeth having grade three mobility extraction is
preferred over endodontic treatment
A tooth with a poor periodontal prognosis may have to be sacrificed, despite a favorable
endodontic prognosis.
7.
2. Improper positioningof teeth.
Partially erupted, impacted and mal-positioned teeth are
contraindicated for endodontic treatment.
It is very difficult to make proper accessibility and isolation while doing
endodontic treatment in these malposed teeth.
8.
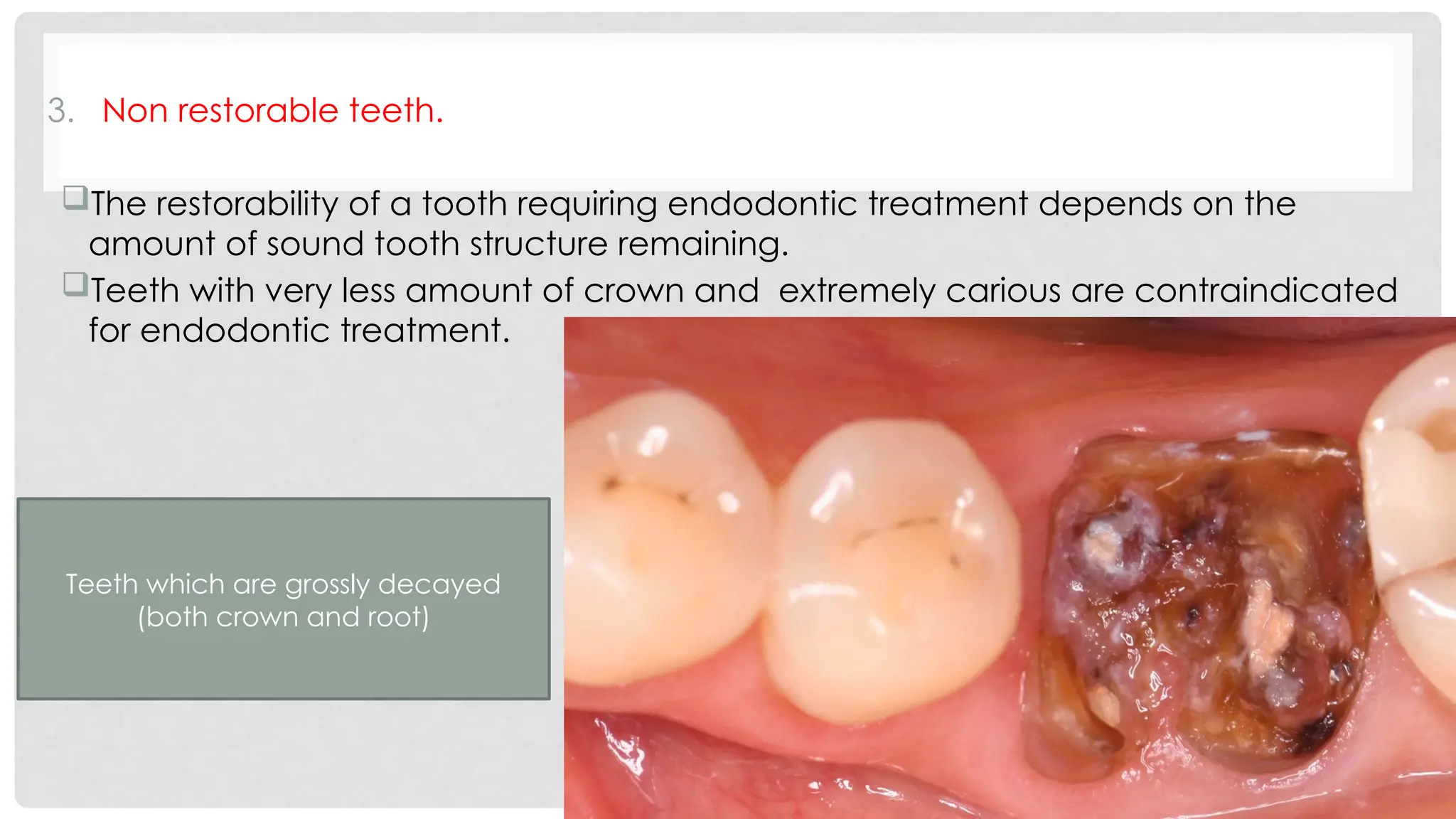
3. Non restorableteeth.
The restorability of a tooth requiring endodontic treatment depends on the
amount of sound tooth structure remaining.
Teeth with very less amount of crown and extremely carious are contraindicated
for endodontic treatment.
Teeth which are grossly decayed
(both crown and root)
9.
4. Abnormal canalconfiguration.
Severely curved canal, aberrant extra canals are very difficult for instrumentation
Teeth with such canal configuration are not ideal for endodontic treatment.
Curvature of 20º in a narrow root canal is very difficult to negotiate also a curvature of
30º with a wide canal is not easily negotiable.
The degree of curvature ,size
and constriction of the root
canal must be judged prior to
endodontic treatment
10.
5. Iatrogenic error.
PainfulTeeth where previous attempt of endodontic treatment has been
done often show ledges, perforations, broken instruments in the canals.
Prognosis of such cases are questionable if not treated properly.
11.
FACTORS OF CASESELECTION
Case selection is broadly based upon three factors
• Factors associated with teeth.
• Factors associated with patients' health.
• Factors associated with clinician.
12.
FACTORS ASSOCIATED WITHTEETH.
1.Is the tooth needed or important? Could it some day serve as an abutment
for prosthesis?
Non-functional
Over-erupted
Not abutment
13.
2. Is thetooth salvageable, or is it so badly destroyed that it cannot be restored?
14.
3. Is thetooth serving esthetically, or would the patient be better served by
its extraction and a more cosmetic replacement?
4. Is the tooth so severely involved periodontally that it would be lost soon
for this reason?
15.
FACTORS ASSOCIATED WITHPATIENT’S HEALTH
• Before starting endodontic treatment, the clinician must take proper medical
history about the patient, The clinician should search for following
information's -
Anxiety (past experiences and management strategy).
Bleeding disorder.
Presence of prosthetic valves, joints, stents, pacemakers.
Unstable angina: required Antibiotics (prophylactic or therapeutic).
Reduced mouth opening.
16.
FACTORS ASSOCIATED WITHCLINICIAN
The clinician should have
proper endodontic
instruments and clinical set
up for the treatment.
The clinician should have
well equipped hands for
treatment.
17.
AAE CASE DIFFICULTYASSESSMENT FORM AND
GUIDELINES
The American Association of Endodontists has developed a practical
tool that makes case selection more efficient, more consistent and
easier to document.
The Endodontic Case Difficulty Assessment Form is intended to assist
practitioners with endodontic treatment planning, but can also be
used to help with referral decisions and record keeping
18.
The assessment formidentifies three categories of considerations which may
affect treatment complexity: patient considerations, diagnostic and treatment
considerations, and additional considerations. Within each category, levels of
difficulty are assigned based upon potential risk factors. The levels of difficulty
are sets of conditions that may not be controllable by the dentist.
For each level of difficulty, guidelines are given to aid the dentist in
determining whether the complexity of the case is appropriate for his or her
experience or comfort level.
CASE 1 VSCASE 2
• Fit and well 21- old cooperative male
patient who presented with mild pain
related to #11.
• Extraoral: NAD
• 72- old male patient who presented with
severe pain related to LL area.
• Extraoral: swelling related to LL.
• Trismus.