Objective
At the endof this chapter, the student will be able to:
Carry out physical examination of urine such as
odor, volume, color, transparency, foam, specific
gravity of urine and interpretation of the test result.
Explain each interfering factors at the moment of
doing the test
Relate abnormal macroscopic appearance of urine
with pathologic states.
3.
Physical Examination ofurine
o Volume
o Color
o Transparency
o Odor
o Foam
o Specific gravity
4.
Introduction
Physical examinationof urine is macroscopic
examination of urine
The first part of routine urinalysis.
It is simplest procedure of all urine examination
But this simplicity doesn’t mean that any one can do it
without any background knowledge and experiences.
Despite its simplicity, it provides hint for the subsequent
chemical and microscopic urinalysis
It includes measurement of the volume of urine,
examination of color and appearance, detecting the foam,
odor, and measuring the specific gravity.
5.
Volume
Not measuredas part of a routine urinalysis
But volume of urine excreted in 24 hours aids for
clinical diagnosis.
The 24-hour urine voided by a healthy
Adult range 600-2000ml
Children (6 to 12 years) about 1000ml
Infants about 600ml.
6.
Volume Cont’d…
Factorsthat affect the urine output
Fluid intake
Diet
Physiological and environmental factors of the
body
7.
Volume Cont’d…
Proceduresfor measurement of urine volume
Collect 24-hour urine specimen in a container of clean and
dry, brown colored.
Add appropriate preservative for the desired urine chemical
test
Label on the container that indicates name of patient,
collection time and date, type of chemical test ordered and
preservative used.
Pour the collected urine into a graduated cylinder of
suitable size (500ml or 2000ml)
Measure the volume and report in terms of ml in 24hrs
8.
Volume Cont’d…
ClinicalSignificance
Abnormal urine volume
Suggests several renal diseases but it is confirmed by
confirmatory tests
Helps for determination of protein
Indicates some clinical features like abnormal execration of
urine/ day
9.
Volume Cont’d…
Measurementof urine volume used for:
Quantitative tests
GFR
Clearance tests
Evaluation of fluid balance and kidney function
Volume Cont’d…
Oliguria:urine volume is less normal <400ml per 24 hours for
prolonged period
Dehydration or poor blood supply to the kidneys
Mechanical obstruction of the urinary system [e.g. due to
renal calculi or tumors]
Excessive salt intake.
Diuresis: temporal increment of urine due to excessive fluid
intake
12.
Color
Normal urinehas pale yellow, yellow, and dark yellow
Urochrome, uroerythrin and urobilin give the urine its
pale yellow color
Urine color is recorded within 30 minute after collection
Pale to colorless urine may indicate
Large fluid intake
Diabetic mellitus
Alcohol consumption
13.
Color cont’d…
Darkyellow or brown red urine may indicate
Concentrated urine
Decreased fluid intake
Fever
Dehydration
Yellow brown or beer brown (amber) color may indicate
the presence of bilirubin.
Clear red color may indicate presence of
hemoglobin/myoglobin
Cloudy red or smoky red color indicates hematuria.
Brown /Black due to methemoglobin
Distinguishing between hemoglobinuria and myoglobinuria may be possible by examining the
patient’s plasma. HOW?
14.
Odour
Normally freshlyvoided urine from healthy individuals has
faint aromatic odor
The test is conducted by smelling of urine and the result is not
used for reporting but for the purpose of comparison with the
subsequent chemical test result.
If the urine specimen is old, it will have ammonical or pungent
odor, which results from the break down and conversion of urea
in the urine into ammonia by the action of bacteria.
Sweet fruity odor of urine results from the presence of ketone
bodies due to diabetes mellitus, prolonged vomiting, starvation
or strenuous exercise.
15.
Foam
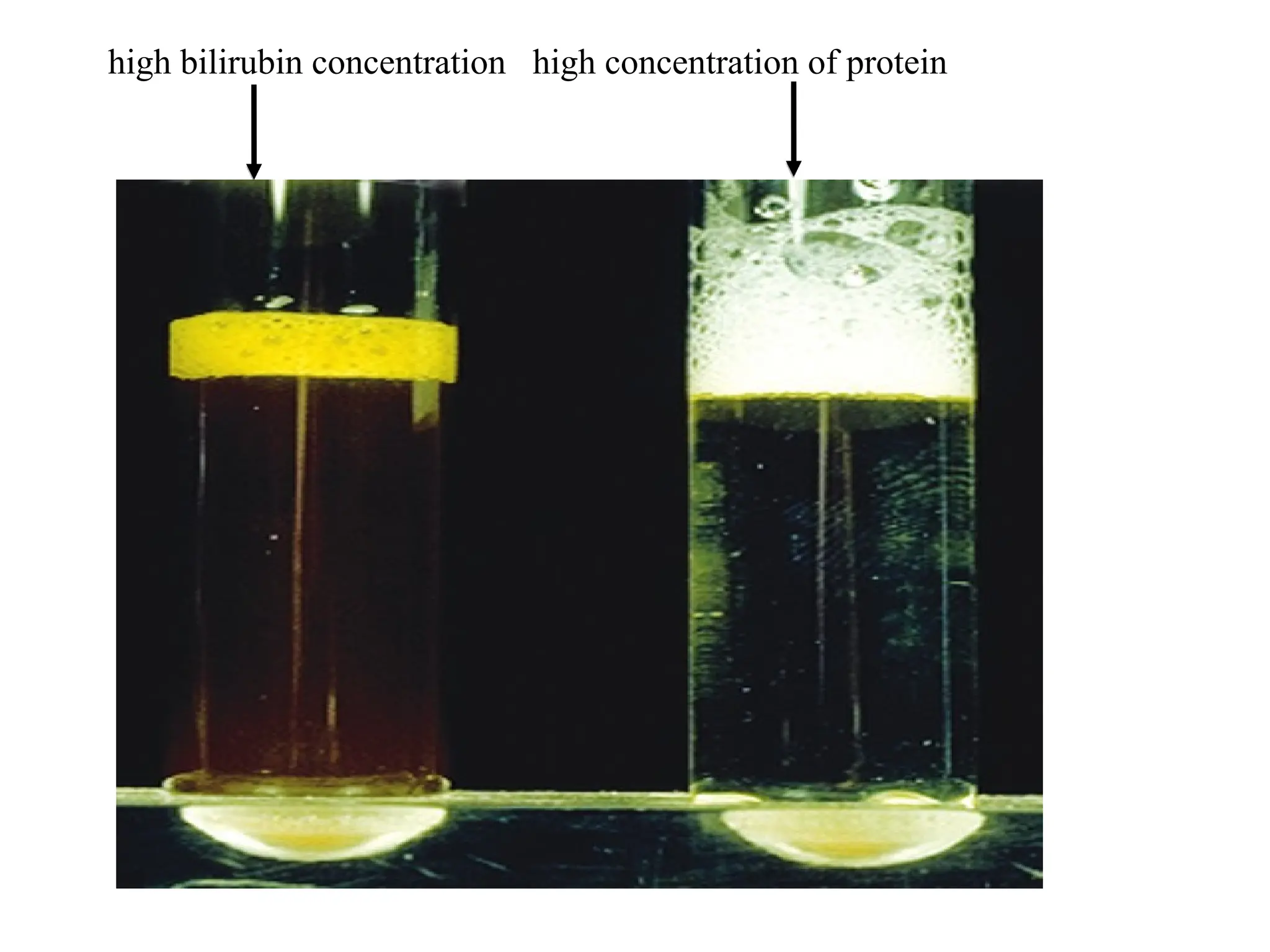
Normally freshurine produces small amount of white foam, but
during certain abnormal conditions, it may be changed.
Yellowish foam indicates the presence of bilirubin in the urine
o must be confirmed by chemical test
When high concentrations of protein are present in the urine, a
large amount of white foam may be seen (for prolonged period
of time)
Transparency/clarity
Freshly voidedurine specimen is normally clear and
transparent
Excretion of turbid urine is not always abnormal
Refrigeration of urine results in the turbidity of the
urine.
Occasionally turbidity of urine may result from
White blood cells [pus cells]
Kidney stones
Yeast cells
High number of bacteria cells
High number of mucus treads
N.B All the above physical findings must be confirmed by
chemical and/or microscopic examination
18.
Degree of Urinetransparency
Clear: no visible particulate mater present
Hazy: some visible particulate mater present;
newsprint is not distorted or obscured when viewed
through the urine
Cloudy: Newsprint can be seen through the urine but
letters are distorted or blurry
Turbid: Newsprint cannot be seen through the urine
19.
Note:
If theurine is so cloudy, microscopical
examinations should be done for the suspended
solutes in the sample.
All urine specimens should be assessed for color
and transparency in similar containers to ensure
consistent results.
20.
Specific gravity (Sp.g)
Specificgravity
Is ratio of the weight of a fixed volume of solution to that of the
same volume of distilled water at a specified similar temperature
Indicator of the kidneys ability to concentrate or dilute urine.
Loss of concentrating or diluting capacity is an indication of
renal dysfunction.
Reflects degree of hydration or dehydration.
A concentrated urine may have a specific gravity of 1.025 –1.030
A diluted urine can have a specific gravity of 1.001-1.010.
Used to assess the kidney’s ability to reabsorb a necessary
component
21.
Measurement of SpecificGravity
There are different methods to measure the urine
specific gravity
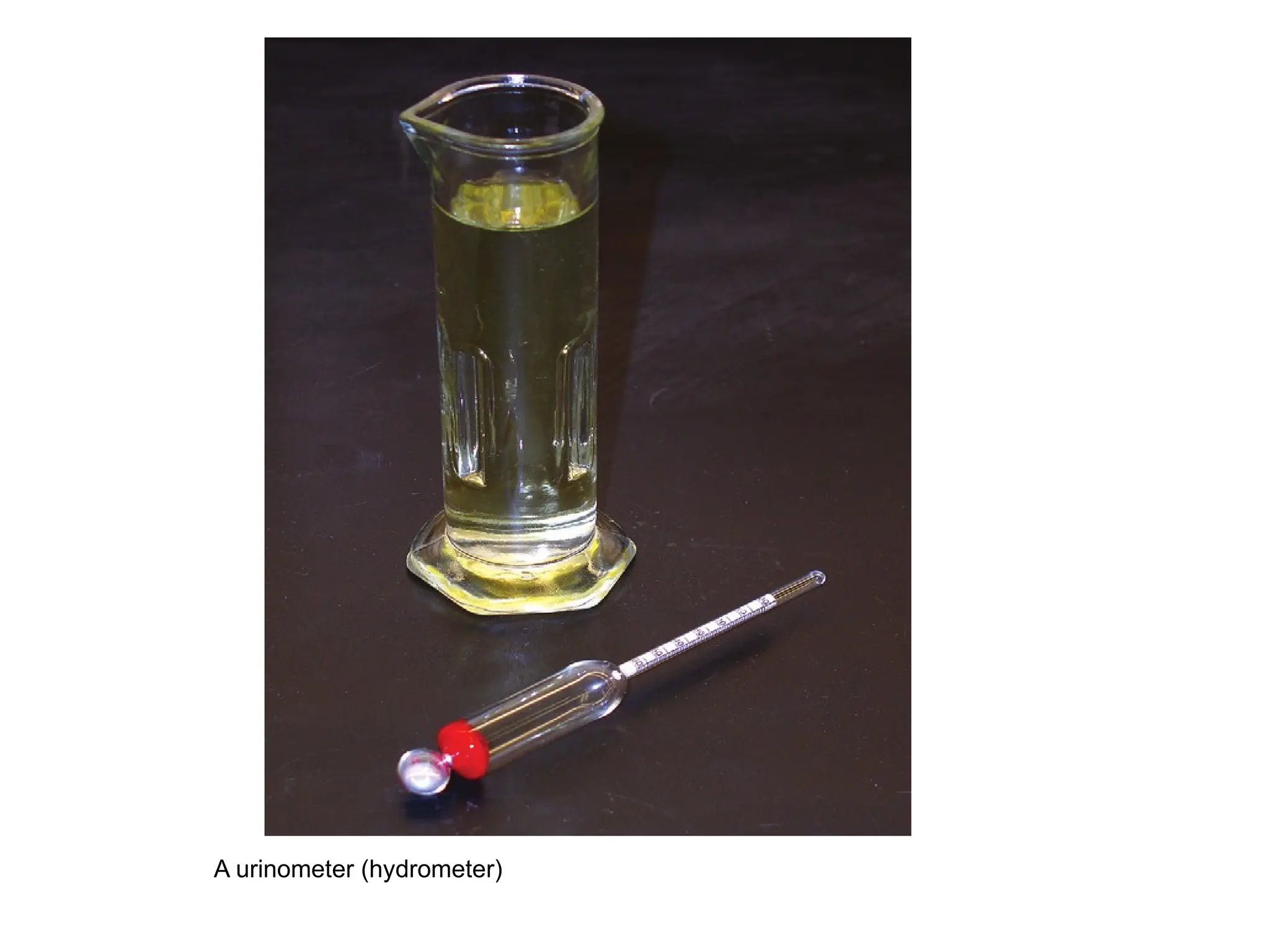
Direct method using Urinometer (hydrometer)
Indirect method using
Refractometer
Reagent strip
Falling drop method
Weighing technique
22.
A) Urinometer method
Urinometer : a glass float weighted with mercury, with an air bulb
above the weight and a graduated stem on the top.
Weighted to float at the 1.000 graduations in pure water when
placed in a glass Urinometer cylinder or appropriate sized test tube.
It is important that the cylinder, or test tube of the correct size so
that the Urinometer can float freely.
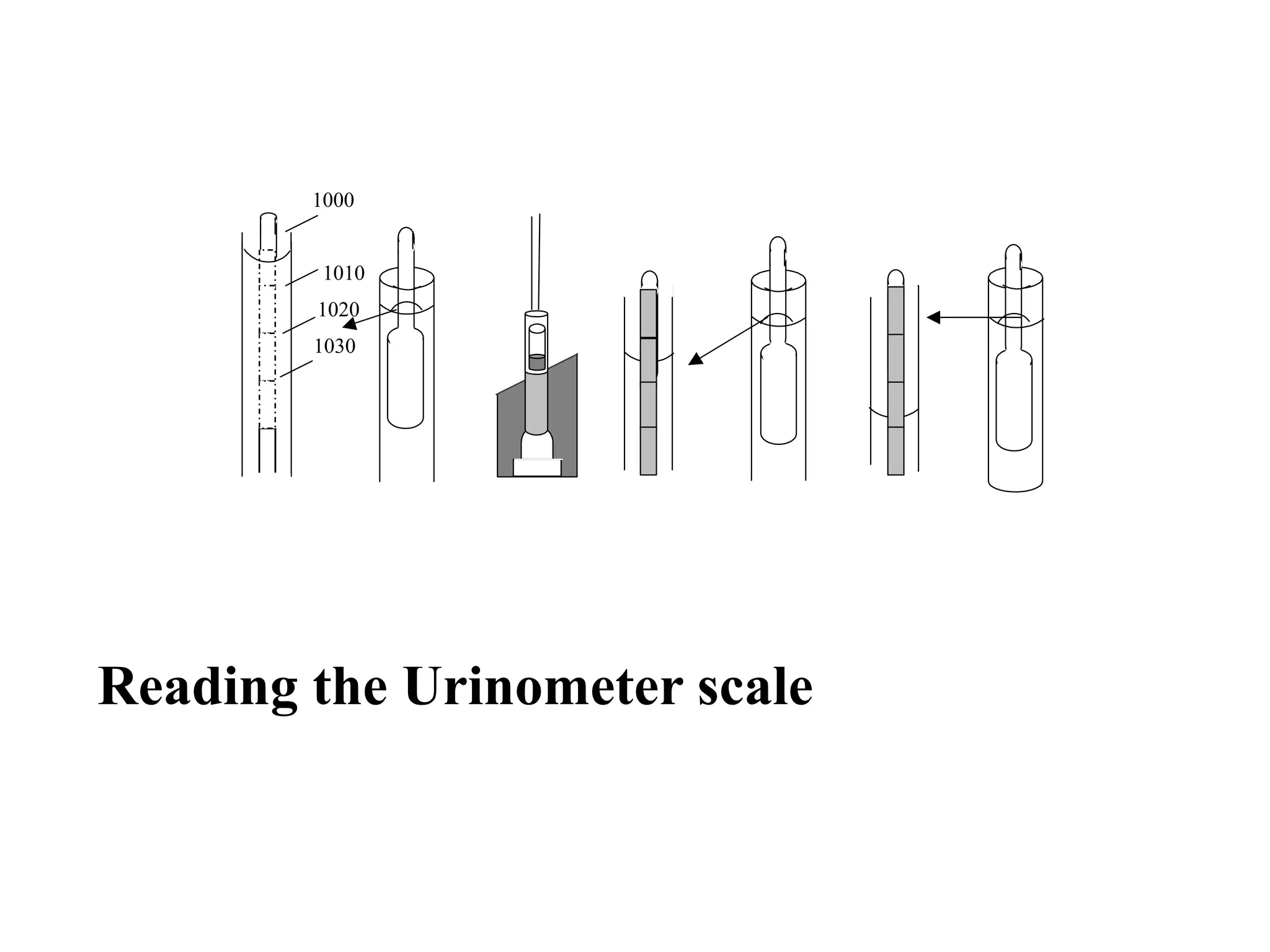
The specific gravity of the urine is read directly from the graduated
scale in the Urinometer stem at the lower meniscus.
The scale of the Urinometer is calibrated from 1.000 – 1.060 with
each division being equal to 0.001.
It is not longer considered an accurate device for determination of
urine specific gravity
Calibration of urinometer
The urinometer must be calibrated everyday.
Distilled water should read 1.000.
Following two standards may also be used for calibrating the
urinometer at different specific gravities
a. Specific gravity 1.011 (750 mOsm/kg): This is prepared by
weighing 24.03 g of oven-dried sodium chloride and adding it
to 1000mL of distilled water .
b. Specific gravity 1.023 (1600 mOsm/kg): Weigh 51.37 g of
oven-dried sodium chloride and add it to 1000 mL of distilled
water
26.
Correction or urinometerreading
Temperature Correction
Most urinometer are calibrated at 20 o
C( sometimes at 15
o
C ) .
For each 3o
C difference 0.001 must be added if above
Subtracted if lower than the calibration temperature.
For example, if the specific gravity of the urine is 1.022 at
23o
C, and the urinometer has been calibrated at 20 o
C, the
correct reading is 1.022+0.001= 1.023.
27.
Correction or urinometerreading
Correction for abnormal Dissolved Substances
The specific gravity increases by
0.004 for every 1% glucose (g/dL) in urine
0.003 for every 1% protein (g/dL) in urine.
Therefore subtract 0.004 from the specific gravity reading for
every 1% glucose in urine.
And subtract 0.003 from the specific gravity reading for every
1% protein in the urine.
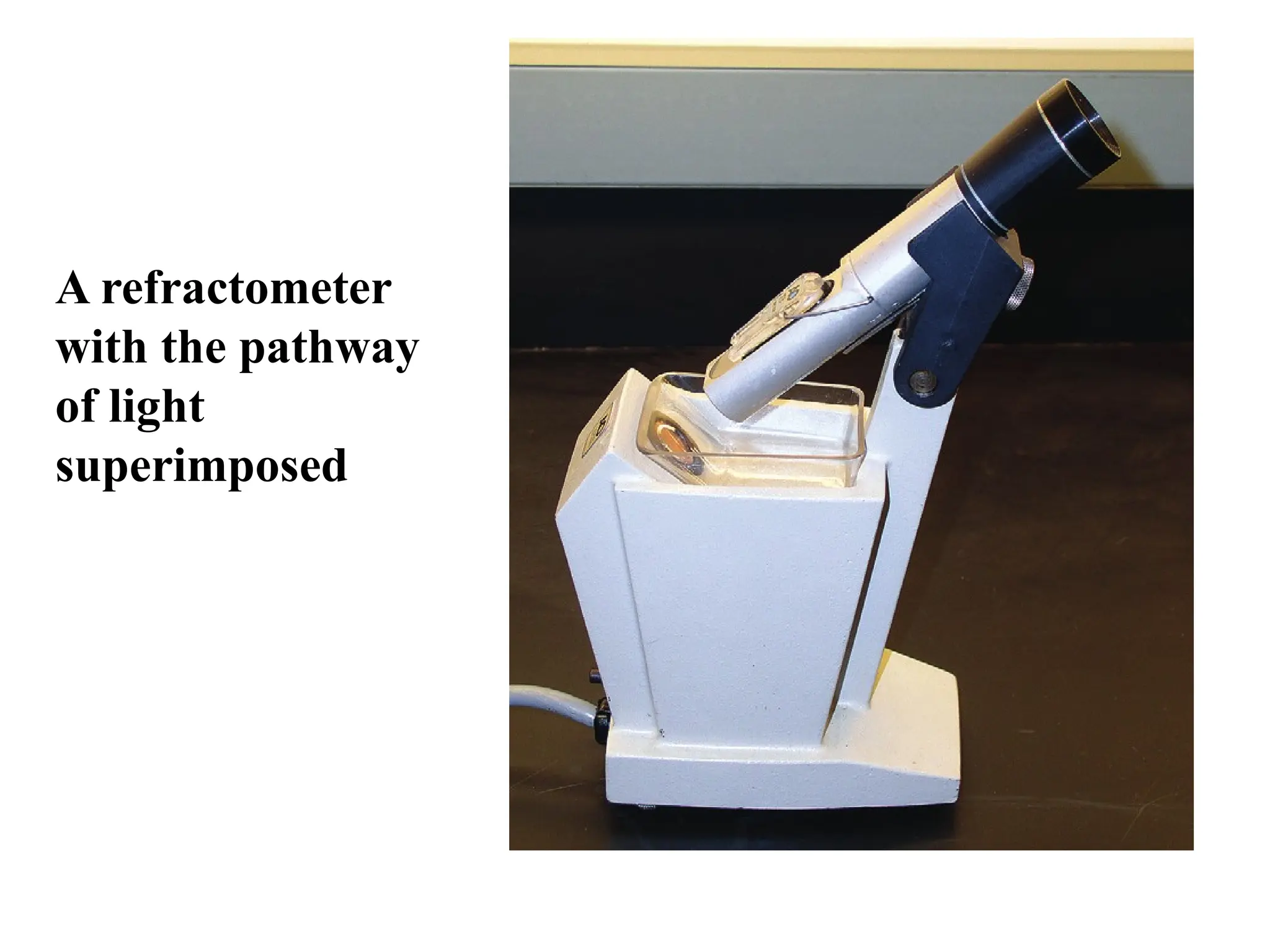
Refractometer method
Refractometeris an instrument, which indirectly measures the
specific gravity by measuring the refractive index
The ratio of the velocity of light in air to the velocity of light
in solution.
This ratio varies directly with the number of dissolved
particles in solution.
The concentration of the specimen determines the angle at
which the light beam enters the prism.
specific gravity scale is calibrated in terms of the angles at
which light passes through the specimen
31.
Factors affect refractiveindex
Wavelength of light used
Temperature of the solution
The concentration of the solution
32.
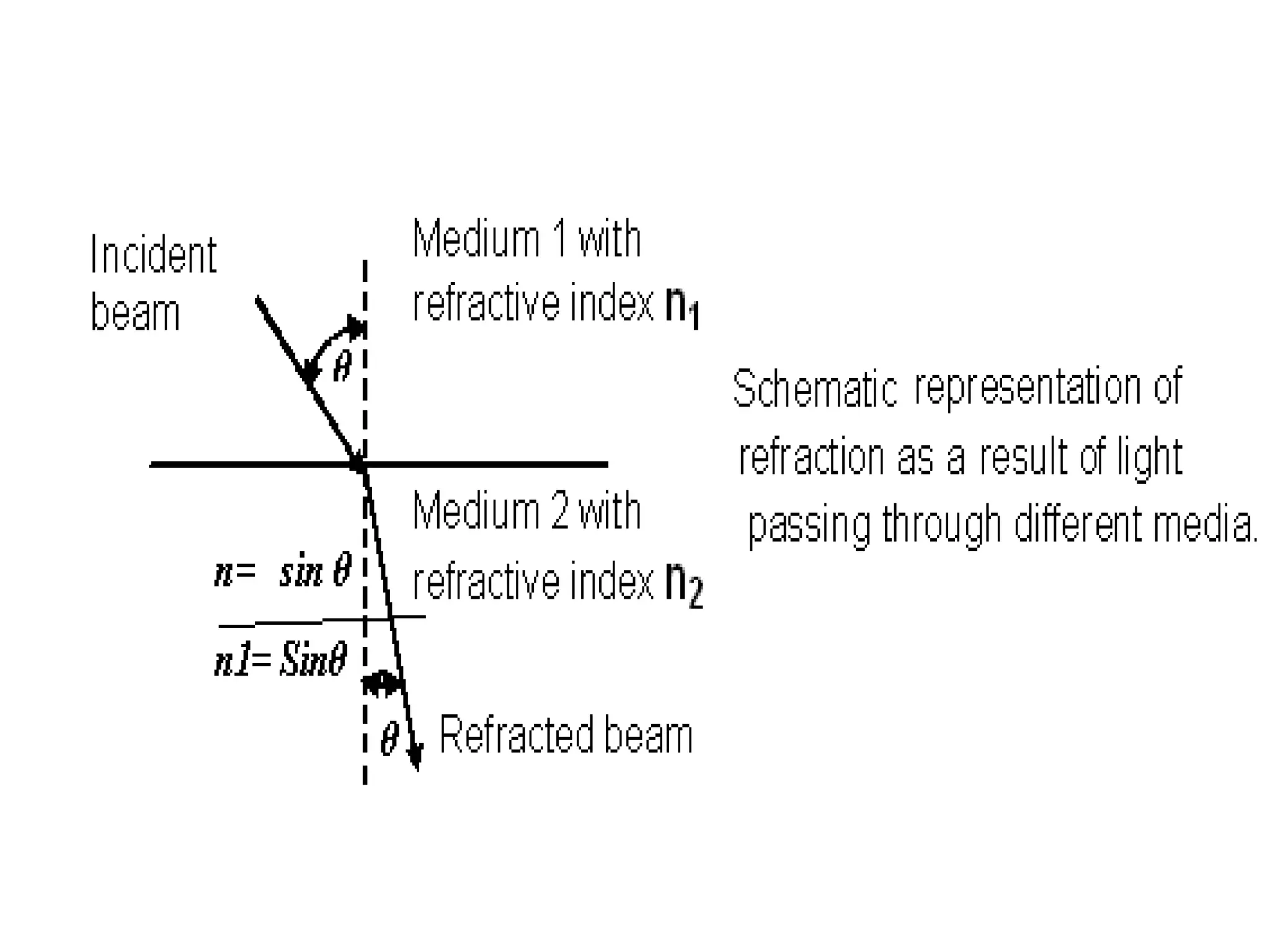
Principle:
Refractometer isbased on the principle of light
refraction.
When a ray of light passes through the optical
system of the refractometer, the path of light going
through air and glass deviates when it meets the fluid
or the urine specimen.
The degree of refraction is proportional to the amount
of solute concentration or the specific gravity of the
fluid.
33.
procedure
Put oneor two drops of sample on the prism
Close the daylight plate gently
The sample must spread all over the prism
surface.
Look at the scale through the eyepiece.
Read the scale where the boundary line
intercepts it.
35.
Refractometer cont’d…
Advantage
Temperature corrections are not necessary
compensated between 15C and 38 C
Limitation:
It require pure test tube transparent to light
Needs skilled professional about handling of the test tube
Corrections for glucose and protein are still calculated
Clinical significance:
the same as urine sp.gv. measurment using urinometer
36.
Reagent Strip Test
Reagent strips have been developed as an indirect method of
measuring specific gravity of urine.
These strips actually measure ionic concentration, which is
related to specific gravity.
Weighing technique
o Thistechnique requires the use of an analytical balance
o As urinometer method, adjustments to the value are necessary
if the urine contains large amount of protein or glucose. :
o Assume that 10 ml of urine weighs 10.15gm
o Assume that 10ml of distilled water is10gm.
o specific gravity urine should be:
10.15gm =1.015
10gm
39.
Clinical Significance
usedto obtain information about two general functions:
the state of the renal epithelium, and
the state of hydration of the patient.
If the kidney is performing adequately, it is capable of
producing urine with a specific gravity ranging from 1.003-
1.030 or higher.
40.
Exercise
1. Define thefollowing term
Specific gravity
Oliguria
Refractive index
2. Describe abnormal color and transparency of urine
specimen and the significance of each.
3. Describe normal and abnormal odour and foam of
urine specimen and the significant of each.
4. How can you correct specific gravity value measured
by urinometer for temperature glucose and protein?
5. Describe the terminologies that indicates abnormal
urine volume and the significance of each.
6. List the method used for determining the specific
gravity of urine and write the principle of each method.
Editor's Notes
#4 The significance of the macroscopic examination of urine (color and turbidity) is frequently overlooked, but it can provide with useful diagnostic information and also give clue for subsequent tests. For example, if a urine specimen is cloudy and red, the presence of red blood cells will probably be revealed by microscopic analysis of the urinary sediment and the chemical examination with positive for haemoglobin or non haemolysed red blood cell.
#6 Under normal conditions, there is a direct relationship between urine volume and water intake. That is if water intake is increased, the kidney will protect the body from excessive retention of water by eliminating a larger volume of urine than normal. Conversely, if water intake is decreased the kidney will protect the body against dehydration by eliminating a smaller volume of urine.
#7 ** Brown colored container that uses for urine collection helps to avoid direct sunlight that causes urine constituent deterioration, like bilirubilin, urobilinogen**
Clinical Significance
Abnormal urine volume has several possible causes, such as reflecting various abnormal conditions. The actual cause and significance of volume changes will be determined with the aid of the routine urinalysis, together with other clinical and laboratory finding
#11 Terminologies: Polyuria: The term polyuria refers to the consistent elimination of an abnormally large volume of urine, over 2000ml/24hr. It may occur due to
A) Pathological conditions
- Diabetes mellitus
- Diabetes insipidus
B) Physiological conditions
- after consumption of coffee, alcohol, tea, caffeine
- Intravenous glucose or saline infusion
- pharmacological agent, such as thiazids and other Oliguria: refers to the excretion of an abnormally small volume of urine, less than 500ml/24 hr consistently. It may occur due to:
Dehydration due to prolonged vomiting, diarrhea etc
Obstruction of some area of the urinary tract/system (mechanical)
Poor supply to kidney that may be due to cardiac insufficiency
Fasting
Anuria: is the nearly complete absence of urine formation. It is less than 100ml of urine per 24hr. It may occur due to:
Complete urinary tract obstruction due to kidney stones, tumors, etc
Acute renal failure
Acute glomerulonephritis
Hemolytic transfusion reaction etc
#12 The color of urine may vary within a day, it may vary from straw [light yellow] to dark amber [dark yellow]
#13 Red/Pink/Brown (RBCs) remaining
in an acidic urine for several hours produce a brown urine due to the oxidation of hemoglobin to methemoglobin.
A fresh brown urine containing blood may also indicate glomerular bleeding resulting from the conversion of hemoglobin to methemoglobin
#15 This is a simple test for detection of bilirubin, which should be performed on abnormally dark or beer brown urine specimen. However, it is not a confirmatory test, and all urine specimens suspected of containing bilirubin should be tested chemically whether the foam test is positive or negative
#20 Specific gravity is defined as the density of a solution compared with the density of a similar volume of distilled water at a similar temperature
#21 Hyposthenuria is a term that is used to describe a urine
with a consistently low specific gravity (1.007). The specific
gravity of the glomerular filtrate is believed to be
around 1.007.4,13 In hyposthenuria there is a concentration
problem. The excretion of urine of unusually high specific
gravity is called hypersthenuria, and this can result from deprivation
of water. Isosthenuria refers to a fixed specific gravity
of 1.010, which indicates poor tubular reabsorption (1.010
was formerly thought to be the specific gravity of the
glomerular filtrate).
Some of the causes of increased specific gravity include
dehydration, proteinuria, glycosuria, eclampsia, heart failure,
renal stenosis, syndrome of inappropriate antidiuretic
hormone secretion, lipid nephrosis, and water restriction
#22 Principle: The urinometer method of measuring specific gravity of urine is based on the principle of buoyancy. As increased solute concentration or specific gravity increases the upthrust of the solution correspondingly increases. The scale of the urinometer reflects the increased up thrust as the latter is pushed up.
#26 The specific gravity of a solution is dependent on temperature. Most urinometers are calibrated for use at 20 oC. For each 3 oC difference 0.001 must be added if above, or subtracted if lower than the calibration temperature. For example, if the specific gravity of the urine is 1.022 at 23 oC, and the urinometer has been calibrated at 20 oC, the correct reading is 1.022+0.001= 1.023.However, significant error will result if the reading is taken on the urine specimen that has been refrigerated. Instead of applying this correction, the urine specimen should be allowed to warm up to room temperature before its specific gravity is determined.
ii. Correction for abnormal Dissolved Substances
The specific gravity increases by 0.004 for every 1% glucose in urine and 0.003 for every 1% protein in solution. Therefore subtract 0.004 from the specific gravity reading for every 1% glucose in urine. And subtract 0.003 from the specific gravity reading for every 1% protein in the urine.
It is not usual however for the Laboratory Technician to correct specific gravity readings for the presence of sugar or protein when laboratory results are reported. Instead, the clinician will be aware that the specific gravity is elevated because of the presence of sugar or protein and takes this into account in the assessment of kidney function.
Procedure
Mix the urine and pour in to the urinometer cylinder. Leave about one inch space at the top so that the fluid does not over flow when the urinometer is floated. Remove any air bubbles from the top of the urine with the gauze or filter paper.
Float the urinometer in the by rotting it rapidly to prevent its touching the bottom or side of the cylinder.
When it comes to rest, read the graduation on the stem of the urinometer at the level of the lower part of the meniscus. When the reading is taken, the urinometer must not be touching the sides of the container.
Record the reading.
If the quantity of the urine is too small to float the urinometer, the urine must be diluted with distilled water. The specific gravity is read and the last two digits of the specific gravity are multiplied by the amount of the dilution. This method is also used if the urine specific gravity is greater than the calibration on the urinometer.
#32 This physical relationship is good only up to a limit of 1.035. Few normal urines have values greater than 1.035; higher values suggest the presence of unusual solutes in the specimen such as glucose, protein or other substances. In such cases, the specific gravity should be reported as “greater than 1035”, rather than extrapolated to a higher value.
#36 pKa is the negative base-10 logarithm of the acid dissociation constant (Ka) of a solution. pKa = -log10Ka
The lower the pKa value, the stronger the acid. For example, the pKa of acetic acid is 4.8, while the pKa of lactic acid is 3.8. Using the pKa values, one can see lactic acid is a stronger acid than acetic acid.
How To Balance Equations In Chemistry
The reason pKa is used is because it describes acid dissociation using small decimal numbers. The same type of information may be obtained from Ka values, but they are typically extremely small numbers given in scientific notation that are hard for most people to understand.
#37 Procedure:
Follow the manufacturer instruction and reporting protocol.
Source of error
Falsely high value may be obtained because of proteinuria greater than 0.1gm/dl and large quantities of divalent cation such as Ca ++, Mg ++
Falsely low value obtained in highly alkaline urine
#38 Example: assume that 10 ml of urine weighs 10.15gm
In addition assume that 10ml of distilled water at the same temperature weighs
10gm.
The specific gravity urine should be:
=1.015
10.15gm
10gm
This method is extremely time consuming
![Volume Cont’d…
Oliguria :urine volume is less normal <400ml per 24 hours for
prolonged period
Dehydration or poor blood supply to the kidneys
Mechanical obstruction of the urinary system [e.g. due to
renal calculi or tumors]
Excessive salt intake.
Diuresis: temporal increment of urine due to excessive fluid
intake](https://image.slidesharecdn.com/3chapterthreephysicalexaminationofurine2-251128184418-51ee3090/75/3-Chapter-three-_-Physical-Examination-of-Urine-2-ppt-11-2048.jpg)
![Transparency/clarity
Freshly voided urine specimen is normally clear and
transparent
Excretion of turbid urine is not always abnormal
Refrigeration of urine results in the turbidity of the
urine.
Occasionally turbidity of urine may result from
White blood cells [pus cells]
Kidney stones
Yeast cells
High number of bacteria cells
High number of mucus treads
N.B All the above physical findings must be confirmed by
chemical and/or microscopic examination](https://image.slidesharecdn.com/3chapterthreephysicalexaminationofurine2-251128184418-51ee3090/75/3-Chapter-three-_-Physical-Examination-of-Urine-2-ppt-17-2048.jpg)