American Academy of Pain Management-September 2010
•
1 like•304 views

The 21st Annual Clinical Meeting of the American Academy entitled Exploring the Science, Practicing the Art: Integrative Pain Management for Optimal Patient Care, in Las Vegas, Nevada, from September 21-24, 2010. This poster was presented on Wednesday, September 22, and Thursday, September 23

Recommended
More Related Content
What's hot
What's hot (18)
Viewers also liked
Viewers also liked (9)
Similar to American Academy of Pain Management-September 2010
Similar to American Academy of Pain Management-September 2010 (20)
Recently uploaded
Recently uploaded (20)
American Academy of Pain Management-September 2010
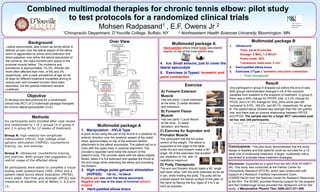
- 1. Combined of HVLA manipulation, exercise and physical therapy for treatment of Lateral multimodal therapies for chronic tennis elbow: pilot study Combination to test protocols for a randomized clinical trials epicondylitis 1, Radpasand Over View Lateral epicondylitis, also known as tennis elbow is defined as pain over the lateral aspect of the elbow which is aggravated by active wrist extension and direct palpation over either the lateral epicondyle of the humerus, the radio-humeral joint space or the proximal muscle bellies. The incidence and prevalence is approximately 1%-3%. Women are more often affected than men, of 9% and 3% respectively, with a peak prevalence at age 42-44. At least 40 different treatment modalities aiming to reduce pain and increase function have been described, but the optimal treatment remains undefined. Hard-padded elbow brace knob was placed exactly on top of the most painful area 4. Ice: Small amount, just to cover the lateral epicondyle 5. Exercises (4 Types): Isometric end point contraction Exercise A) Forearm Extensor Muscle Objective Has two parts 1) pure extension at the wrist, 2) radial deviation and extension To develop and test protocols for a randomized clinical trial (RCT) of 2 multimodal package therapies for chronic lateral epicondylitis (CLE). B) Forearm Flexor Muscle Methods Six participants were enrolled after case review and randomized to 1 of 2 groups (4 in group A and 2 in group B) for 12 weeks of treatment. Group A: high-velocity-low-amplitude manipulation (HVLA), high-voltage pulse galvanic stimulation (HVPGS), counterforce bracing, ice, and exercise. Group B: ultrasound, counterforce bracing, and exercise. Both groups had suggestion to restrict usage of the affected elbow. All participants were asked to complete a visual analog scale questionnaire (VAS_24hs) and a patient-rated tennis elbow evaluation (PRTEE) every week. Pain-free grip strength (PFGS) was measured at baseline, and at Weeks 3, 6,9,and 12. Multimodal package A Multimodal package A 1. Manipulation - HVLA Type A quick thrust using the pad of the thumb in a posterior to anterior direction over the posterior aspect of the radial head, approximately on top of the extensor tendon attachment to the lateral epicondyle. The patient sat on a chair with the upper body in postural alignment. The provider’s opposite hand holds the dorsum of the patient’s wrist. The provider starts with the elbow slightly flexed, takes it to full extension and applies the thrust at the end-range while extending the elbow and pronating the forearm 2. High-voltage pulse galvanic stimulation (HVPGS): 150 Hz ; 19-29mA Positive pad was over the lateral epicondyle Negative pad was at the base of involved elbow’s scapula 3. Hard-padded elbow brace Has two parts 1) pure flexion at the wrist, 2) radial deviation, and flexion Multimodal package B 1. 2. 3. Ultrasound Time: set at 8 minutes Dosage: 3 MHz, 1.5 W/cm² Pulse mode: 20% Transducer head area: 2 cm² Hard-padded elbow brace Exercises (1Type ): Isometric end point contraction Putty therapeutic Result One participant in group A dropped out before the end of care. Both groups demonstrated changes in all of the outcome variables from baseline to the endpoint of treatment. In group A, there was a 59% change for PRTEE total, a 3.2% change for PFGS, and a 51.4% change for VAS_24hs worst pain felt compared to 9.5%, 169.0%, and 65.1%, respectively, for group B. The painful elbow showed less strength than the non-painful one, and there was an inverse relationship between PRTEE and PFGS. The sample size for a larger RCT calculated post ad hoc was 246 participants. Pain Free Grip Strength Patient-Rated Tennis Elbow Evaluation VAS 24hs Worst Pain Group A 70 90 60 50 80 50 C) Exercise for Supinator and Pronator Muscle 40 70 40 30 20 10 D) Putty Therapeutic The arm and forearm should make a 90° angle with each other, with the wrist extended as far as it can, while holding the putty. The putty will be pushed toward the thenar surface of the palm of the hand by flexing the four digits of 2 to 5 as hard as possible. 30 20 10 0 Pre -20 Time Point 40 20 Post Post -10 50 0 -10 Pre 60 30 10 Pre 0 The participant has the full active control of the weight. The elbow is supported at the edge of the table, while the arm and forearm make a 90° angle. All of the exercises had duration per repetition of 10s, with 10 repetitions maximum. Group A Group B 100 Group A Group B 60 Group B Kilograms Background 2 Northwestern Health Sciences University, Bloomington, MN Department, D’Youville College, Buffalo, NY Palmer Center for Chiropractic Research, Davenport, IA, USA PRTEE Score (0-50) 1Chiropractic VAS (0-100) 1 Mohsen E.F. Owens Mohsen Radpasand, DC, MD Jr 2 Time Point Post Time Point Conclusions: This pilot study demonstrated that the study design is feasible and that patients could be recruited for a 12week trial of multimodal treatment. A larger, multicenter trial is warranted to evaluate these treatment strategies. Disclosure: Supported by a grant from the NIH (K30-AT-0097704). This study was conducted at the Palmer Center for Chiropractic Research (PCCR), which was constructed with support of a Research Facilities Improvement Grant (C06RR15433) from the National Center for Research Resources at the NIH. The NCMIC provided financial support for the program, and the Chattanooga Group provided the ultrasound unit for this study. J Manipulative Physiol Ther. 2009;32(7):571-585